Clinical Interventions During Inter‐hospital Transfer of Infants With Moderate‐to‐Severe Bronchiolitis: Implications for Advanced Nursing Practice
Arthur Gaudaire, Christophe Milesi, Alexia Morel, Julien Baleine, Maliha Badr, Alexandra Deveze, Sylvain Paulhac, Marion Palpacuer, Gilles Cambonie, Arthur Gavotto

TL;DR
This study identifies specific oxygen and blood gas thresholds to determine if nurse-led teams can safely transport infants with severe bronchiolitis without a doctor.
Contribution
The paper introduces evidence-based thresholds for FiO2 and pCO2 to guide triage decisions for nurse-led transport teams.
Findings
Higher FiO2, lower pH, and higher pCO2 levels were associated with the need for clinical intervention during transport.
FiO2 > 40% on HFNC or pCO2 > 65 mmHg predicted the need for a medicalised team with high accuracy.
Most transfers can be safely managed by nurse-led teams when these thresholds are not exceeded.
Abstract
Bronchiolitis is a leading cause of hospitalisation and paediatric intensive care admissions in infants. Moderate‐to‐severe cases often require inter‐hospital transfer for respiratory support, usually organised by specialised paediatric emergency transport services (PETS). The optimal composition of transport teams, whether nurse‐led or medicalised, remains uncertain. To identify predictive factors available during the regulation call that can help determine when an inter‐hospital transfer of infants with moderate‐to‐severe bronchiolitis can be safely conducted by a nurse‐led team without a paediatrician, by predicting the need for clinical intervention during transport. A retrospective observational study was conducted from 2021 to 2023 within the PETS of a French University Hospital. Infants under 2 years transferred for moderate‐to‐severe bronchiolitis were included. The primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
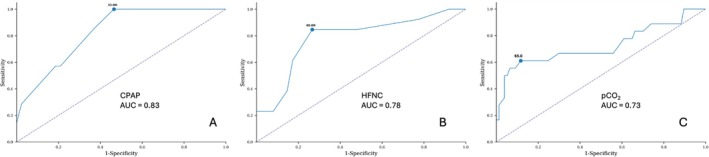 FIGURE 1
FIGURE 1| Variables | Total | 2021 | 2022 | 2023 | |
|---|---|---|---|---|---|
|
| 167 | 47 | 71 | 49 | |
| Patient's characteristics | |||||
| Male (yes) | 77 (46) | 23 (49) | 28 (39) | 26 (53) | |
| Age (days) | 157 ± 169 | 137 ± 145 | 138 ± 168 | 202 ± 184 | |
| Weight (Kg) | 5.9 ± 2.7 | 5.7 ± 2.3 | 5.4 ± 2.5 | 6.7 ± 2.9 | |
| Virus ( | RSV | 90 (81) | 34 (87) | 37 (79) | 19 (76) |
| Others | 21 (19) | 5 (13) | 10 (21) | 6 (24) | |
| Significant history | Prematurity | 21 (13) | 3 (6) | 10 (14) | 8 (16) |
| CHD | 13 (8) | 3 (6) | 6 (9) | 4 (8) | |
| Description of regulation call | |||||
| Chest X‐ray ( | Atelectasis | 19 (20) | 3 (10) | 12 (34) | 4 (12) |
| Pneumopathy | 18 (19) | 4 (14) | 5 (14) | 9 (27) | |
| mWCAS ( | 4.8 ± 1.7 | 4.2 ± 1.2 | 5.0 ± 2.0 | 5.2 ± 1.7 | |
| Blood gas ( | pH | 7.33 ± 0.07 | 7.35 ± 0.06 | 7.34 ± 0.08 | 7.31 ± 0.08 |
| pCO2 (mmHg) | 52.1 ± 13.5 | 50.0 ± 10.4 | 53.0 ± 15.9 | 53.4 ± 13.1 | |
| CRP (mg/L) ( | 33.1 ± 49.8 | 34.0 ± 42.5 | 26.4 ± 40.2 | 39.4 ± 63.5 | |
| Venous access (yes) | 112 (67) | 36 (77) | 42 (59) | 35 (71) | |
| Nasogastric tube (yes) | 73 (44) | 20 (43) | 32 (45) | 21 (43) | |
| Ventilatory support | Low‐flow O2 | 29 (17) | 6 (13) | 15 (21) | 8 (16) |
| HFNC | 88 (53) | 28 (59) | 34 (48) | 26 (53) | |
| CPAP | 50 (30) | 13 (28) | 22 (31) | 15 (31) | |
| FiO2 (%) | 37.2 ± 13.1 | 38.3 ± 11.4 | 38.7 ± 15.6 | 33.9 ± 10.1 | |
| Paediatric emergency medical service | |||||
| Full team (yes) | 158 (95) | 46 (98) | 66 (93) | 46 (94) | |
| Upgrade in respiratory support (yes) | 47 (28) | 19 (40) | 15 (21) | 13 (26) | |
| Upgrade to NIV or intubation (yes) | 15 (9) | 7 (15) | 2 (3) | 6 (12) | |
| Ventilatory support | Low‐flow O2 | 23 (14) | 5 (11) | 11 (15) | 7 (14) |
| HFNC | 58 (35) | 11 (23) | 27 (38) | 20 (41) | |
| CPAP | 70 (42) | 25 (53) | 31 (44) | 14 (29) | |
| NIV | 16 (10) | 6 (13) | 2 (3) | 8 (16) |
| Variables | Simple transport ( | Medical intervention ( |
| |
|---|---|---|---|---|
| Male (yes) | 68 (46) | 9 (45) | 0.99 | |
| Age (days) | 162 ± 176 | 116 ± 108 | 0.51 | |
| Weight (Kg) | 5.9 ± 2.7 | 5.2 ± 2.4 | 0.33 | |
| RSV (yes) | 78/97 (81) | 12/14 (86) | 0.40 | |
| Description of regulation call | ||||
| Chest X‐ray ( | Atelectasis | 17/83 (20) | 2/14 (14) | 0.10 |
| Pneumopathy | 18/83 (22) | 0/14 (0) | ||
| Blood gas ( | pH | 7.34 ± 0.07 | 7.30 ± 0.08 | 0.03 |
| pCO2 (mmHg) | 49.6 ± 11.2 | 62.9 ± 17.9 | 0.01 | |
| CRP (mg/L) ( | 35.4 ± 51.1 | 18.5 ± 41.4 | 0.11 | |
| mWCAS ( | 4.6 ± 1.8 | 5.6 ± 0.8 | 0.06 | |
| Ventilatory support | Low‐flow O2 | 29 (20) | 0 (0) | 0.09 |
| HFNC | 75 (51) | 13 (65) | ||
| CPAP | 43 (29) | 7 (35) | ||
| FiO2 (%) | 34.8 ± 10.2 | 51.3 ± 19.3 | < 0.01 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Trauma and Emergency Care Studies · Travel-related health issues
Introduction
1
Infant bronchiolitis is a contagious viral infection that affects approximately 480 000 children each winter in France, including nearly 30% of infants under 2 years of age. It accounts for 15%–17% of hospital admissions in this population [1, 2]. The main causative viruses are respiratory syncytial virus (RSV), responsible for about half of hospitalisations in infants under 6 months and rhinovirus [2]. First‐line treatment of bronchiolitis is symptomatic, consisting primarily of nasal suction. Oxygen dependency may occur, requiring oxygen therapy through a low‐flow system. In more severe cases, positive‐pressure respiratory support such as high‐flow nasal cannula (HFNC), continuous positive airway pressure (CPAP) or two‐level non‐invasive ventilation (NIV) may be needed [3, 4, 5, 6]. Intubation and mechanical ventilation are required in 4%–7% of patients admitted to paediatric intensive care units (PICUs) [5, 7].
Because these advanced respiratory techniques (HFNC, CPAP and NIV) are only available in PICUs, which are primarily located in tertiary or university hospitals, infants frequently require inter‐hospital transfer from non‐specialised facilities to a centre with intensive care capacity [8]. These secondary transfers are organised by specialised paediatric emergency transport services (PETS) [9].
Decisions regarding the composition of the transport team are made during a medical regulation call. Based on the infant's medical history, illness severity and the support required for vital functions, the regulating physician may dispatch either a nurse‐led inter‐hospital transfer, involving an advanced paediatric critical care nurse and an ambulance driver, or a medicalised transfer including a paediatrician. This decision has significant implications, as mobilising a full team temporarily reduces availability for primary emergency interventions, which remain the PETS' core mission.
The main objective of this study was to identify predictive criteria available during the regulation call to determine when an inter‐hospital transfer of infants with moderate‐to‐severe bronchiolitis can be safely performed by a nurse‐led team without a paediatrician.
Methods
2
Study Design and Population
2.1
This retrospective observational study was conducted within the Paediatric Emergency Transport Service (PETS) of Montpellier University Hospital, France, from January 2021 to December 2023. All infants under 2 years of age requiring inter‐hospital transfer for moderate‐to‐severe bronchiolitis were eligible. As no universally accepted definition of bronchiolitis severity exists, patient selection was based on the need for respiratory support (low‐flow oxygen, HFNC or CPAP).
Exclusion criteria were: (i) patients already intubated or receiving two‐level NIV at the time of the regulation call, (ii) patients breathing spontaneously without any ventilatory support at the time of the call, and (iii) patients with incomplete data. Infants breathing spontaneously (i.e., receiving no low‐flow oxygen, HFNC or CPAP) were excluded because they would not normally require PETS intervention, whereas intubated infants or those on two‐level NIV were excluded because our institutional protocol mandates paediatrician presence for their transport.
Regional Organisation of Paediatric Intensive Care and Moderate‐To‐Severe Bronchiolitis Management Protocol
2.2
When healthcare professionals request an inter‐hospital transfer, they contact the regional transfer regulation centre based at Montpellier University Hospital, which assigns a PETS team. The Montpellier PETS is the only service operating 24/7 in the eastern Occitanie region, where the only regional PICU is also located.
In France, the formal status of advanced paediatric or neonatal nurse is not officially recognised. However, in our institution, experienced nurses have developed advanced clinical and procedural expertise through structured in‐house training inspired by advanced nursing practice models from English‐speaking healthcare systems with formally recognised advanced nursing roles. These nurses are fully integrated into PETS activities and play a central role in both medicalised and nurse‐led inter‐hospital transfers.
Advanced paediatric critical care nurses working at PETS Montpellier are state‐registered paediatric nurses with postgraduate experience in neonatal and paediatric intensive care. Their scope of practice includes management of non‐invasive respiratory support (HFNC and CPAP), airway monitoring, peripheral venous access, gastric tube placement and administration of emergency treatments under predefined protocols. All are certified in Newborn Life Support (NLS) [10] and European Paediatric Advanced Life Support (EPALS) [11].
The core PETS team consists of a paediatrician and an advanced paediatric critical care nurse and is available 24 h a day, 7 days a week. In addition, a second senior nurse, also available 24/7 and based within the tertiary hospital, supports nurse‐led inter‐hospital transfers and provides delivery room assistance and participation in the in‐hospital mobile resuscitation team when required. During the study period, the mobile nursing team comprised 12 senior nurses and remained stable.
The management of infants with bronchiolitis during transfer follows a predefined service protocol based on ventilatory support. For moderate bronchiolitis (modified Wood's Clinical Asthma Score [mWCAS] [4] ≤ 4), transport is performed under low‐flow oxygen or high‐flow nasal cannula (HFNC). For severe bronchiolitis (mWCAS > 4), continuous positive airway pressure (CPAP) with a positive end‐expiratory pressure (PEEP) of 7 cmH_2_O is initiated, with escalation to two‐level NIV if the clinical condition worsens. Intubation is considered only as a last resort in cases of refractory hypoxia, recurrent apnoea or altered consciousness despite well‐administered NIV.
In France, while most emergency departments are able to initiate HFNC or CPAP in infants with bronchiolitis, the prolonged management of such non‐invasive respiratory support is usually limited to tertiary, university‐affiliated centres.
Data Collected
2.3
The following data were recorded: age at transfer, weight, identified virus, relevant comorbidities, capillary blood gas results (pH, pCO_2_ in mmHg) from the referring hospital, C‐reactive protein (CRP) levels (mg/L), chest X‐ray findings, mWCAS score and the presence of venous access or a nasogastric tube.
During the regulation call and throughout transport, ventilatory mode and FiO_2_ (%) were noted. The type of transfer decided by the regulating physician—nurse‐led or medicalised—was also documented.
Outcomes
2.4
The primary outcome was the occurrence of a clinical intervention during inter‐hospital transfer. This outcome was deliberately chosen as a pragmatic and clinically meaningful surrogate for situations requiring physician‐level management during transport. A clinical intervention was defined as any event requiring medical decision or advanced airway and haemodynamic management, including management of apnoea or respiratory distress requiring manual ventilation with a self‐inflating bag, fluid bolus administration, initiation of two‐level NIV, endotracheal intubation or cardiopulmonary resuscitation.
The secondary objective was to identify which clinical or paraclinical parameters available at the time of the regulation call could predict the occurrence of such interventions, in order to support decision‐making regarding team allocation (nurse‐led versus medicalised transfer).
Ethical and Institutional Approvals
2.5
The study complied with the principles of Good Clinical Practice and the Declaration of Helsinki. It was approved by the Institutional Review Board of Montpellier University Hospital (CSE‐2024‐06‐072) on July 24, 2024. In accordance with French legislation, written informed consent from participants or their legal guardians was not required.
Statistical Analysis
2.6
Comparisons were performed using Fisher's exact test, chi‐squared test, Student's t‐test or Wilcoxon–Mann–Whitney test, as appropriate. Predictive performance of the data provided during the regulation call was assessed using sensitivity, specificity, positive and negative predictive values and the area under the receiver operating characteristic (ROC) curve.
A p‐value < 0.05 was considered statistically significant. Analyses were performed using EasyMedStat version 3.21.5 (Paris, France).
Results
3
Study Population
3.1
Over the 3‐year study period, the PETS completed 2219 secondary transports. Among these, 190 (8.6%) involved infants with moderate‐to‐severe bronchiolitis. Forty‐three were excluded: 2 already intubated, 9 on two‐level NIV, 12 breathing spontaneously and 20 with incomplete data.
A total of 167 infants (77 boys, 90 girls) were included. The mean age was 157 ± 169 days, and mean weight was 5.9 ± 2.7 kg. Comorbidities included prematurity in 13% and congenital heart disease (CHD) in 8%. Viral identification was available in 66% of cases, among which RSV accounted for 81%. Table 1 summarises population characteristics by year.
Data Available at the Regulation Call
3.2
At the time of the regulation call, 88 infants (53%) were receiving HFNC (mean FiO_2_ 36.8% ± 13.0%), 50 (30%) were on CPAP (mean FiO_2_ 37.8% ± 13.6%) and 29 (17%) were on low‐flow oxygen.
The mWCAS score was reported in 28% of cases (mean 4.8 ± 1.7). Chest X‐rays were performed in 97 infants (58%), revealing atelectasis in 20% and pneumonia in 19% of cases. A capillary blood gas was available in 95 cases (57%), and CRP levels in 103 (62%). Venous access was present in 67% of infants, and 44% had a nasogastric tube (Table 1).
Clinical Intervention During Transport
3.3
A complete team (paediatrician, advanced paediatric critical care nurse and driver) was dispatched in 158 transfers (95%).
A clinical intervention occurred in 20 cases (12%), including 15 NIV initiations, 4 manual ventilations for apnoea and 1 previously undiagnosed cyanogenic CHD.
An additional 32 infants experienced escalation of respiratory support (25 from HFNC to CPAP, and 7 from low‐flow oxygen to HFNC), which were managed by nurse‐led teams according to protocol (Table 1).
Prediction of Clinical Intervention
3.4
Table 2 compares characteristics at the regulation call according to the occurrence of an intervention requiring a complete team. Infants who required intervention had higher FiO_2_ (51.3% ± 19.3% vs. 34.8% ± 10.2%; p < 0.01), lower pH (7.30 ± 0.08 vs. 7.34 ± 0.07; p = 0.03) and higher pCO_2_ (62.9 ± 17.9 vs. 49.6 ± 11.2 mmHg; p = 0.01). Other collected variables (e.g., age, comorbidities, CRP level, chest X‐ray findings and viral identification) were not significantly associated with clinical intervention.
ROC analyses showed that: (i) CPAP with FiO_2_ > 35% predicted the need for a medicalised team (AUC = 0.83; sensitivity 86%; specificity 63%), (ii) HFNC with FiO_2_ > 40% also predicted clinical intervention (AUC = 0.78; sensitivity 85%; specificity 73%), and (iii) pCO_2_ > 65 mmHg was a strong indicator (AUC = 0.73; sensitivity 56%; specificity 94%). Because mWCAS was available in only 28% of cases and was frequently missing at the time of the regulation call, it was not suitable for reliable ROC analysis.
Combining these three criteria at the regulation call (HFNC FiO_2_ > 40%, or CPAP FiO_2_ > 35%, or pCO_2_ > 65 mmHg) yielded a sensitivity of 90%, specificity of 78% and negative predictive value of 98% for predicting clinical intervention (Figure 1).
ROC curves. ROC curves predicting the occurrence of clinical intervention (A) CPAP FiO2, (B) HFNC FiO2 and (C) pCO2. AUC, area under the curve; CPAP, continuous positive airway pressure; HFNC, high‐flow nasal cannula.
Discussion
4
This 3‐year retrospective observational study included 167 infants under 2 years of age transferred for moderate‐to‐severe bronchiolitis. A complete medical team was mobilised in 95% of transports, yet clinical interventions requiring physician presence occurred in only 12% of cases. Most of these situations were predictable from parameters available at the regulation call, particularly HFNC with FiO_2_ > 40%, or CPAP with FiO_2_ > 35%, or pCO_2_ > 65 mmHg. Applying these thresholds would have allowed 70% of transfers to be safely managed by nurse‐led teams.
These findings confirm that simple, objective respiratory criteria can reliably guide the choice of transport team. Similar observations have been reported internationally, suggesting that optimising triage for medical versus nurse‐led retrieval could reduce unnecessary mobilisation of paediatricians while maintaining safety and efficiency [12]. Although the negative predictive value of this predictive model was not 100%, the few discordant cases reflected physician discretion rather than protocol failure. The indication for NIV remains variable among physicians, despite the lack of evidence that NIV offers advantages over CPAP during transport [13].
This study was designed with a pragmatic, real‐life perspective, reflecting the conditions under which triage decisions are actually made during paediatric emergency transport regulation. Rather than relying on idealised severity classifications or systematically recorded clinical scores, we chose to focus on objective parameters that are consistently available at the time of the regulation call, such as ventilatory support modality, FiO_2_ and blood gas values. This approach aims to enhance the clinical applicability of our findings and to support decision‐making in everyday practice.
The high proportion of infants initially supported with HFNC or CPAP by referring hospitals demonstrates the success of regional training and standardised care protocols [14]. These initiatives have enhanced local stabilisation capacity and decreased the need for invasive ventilation before transport. Most infants also had venous access and a nasogastric tube inserted before arrival of the transport team, highlighting improved anticipation by bedside nurses. Nasogastric decompression optimises positive‐pressure ventilation and enables enteral feeding, which has been associated with shorter hospital stays and lower ventilatory requirements [15, 16, 17, 18].
Our data suggest that, in most cases, the inter‐hospital transfer of infants with bronchiolitis can be safely performed by advanced paediatric critical care nurses. Within our PETS, these nurses are experienced in intensive and emergency care, certified in both NLS and EPALS and trained specifically for paediatric transport [10, 11]. Their role includes ensuring airway stability, adjusting FiO_2_, performing procedures such as venous or gastric tube placement, and administering treatments under pre‐established protocols. These findings are consistent with recent international literature describing the expanding role of advanced nursing practitioners in paediatric critical care transport services. In particular, Herring et al. highlighted the contribution of advanced clinical practitioners to paediatric retrieval teams, supporting the feasibility and safety of nurse‐led transport models within well‐defined governance frameworks [19]. It is important to note that the scope of practice of advanced paediatric critical care nurses in France differs from that of advanced nurse practitioners described in other healthcare systems, particularly in English‐speaking healthcare systems where such roles are formally recognised. French transport nurses do not perform endotracheal intubation or prescribe independently. Expanding the scope of nurse‐led transfers could therefore optimise resource allocation, maintain paediatrician availability for primary emergencies and reduce operational costs while preserving patient safety.
Study Limitations
4.1
This study has several limitations. Its retrospective design led to missing data, notably regarding the mWCAS, which plays a key role in assessing severity and guiding ventilatory management. The score was documented in only 28% of cases, particularly infrequently at the time of the regulation call, even though part of the clinical decision‐making relies on it. Because of this inconsistent documentation in routine practice, we deliberately adopted a pragmatic approach, prioritising clinical and paraclinical parameters that are routinely and reliably available at the time of the regulation call over formal severity scores. However, this limitation could be easily overcome in daily practice, as such clinical scoring is feasible even through videoconferencing.
The definition of ‘clinical intervention’ was based on pragmatic criteria and could be debated; some upgrades in respiratory support (low‐flow oxygen to HFNC or HFNC to CPAP) were not classified as interventions, as they are permitted within nursing competence under current protocols.
As a single‐centre study, our results may not be directly generalisable to other regions where paediatric emergency transport and nursing expertise differ. However, our findings are consistent with previous research from our team on bronchiolitis management and respiratory support in infants, which supports their internal validity and contextual relevance [3, 4, 5, 6]. This coherence supports the internal validity of our results and reinforces their potential applicability within similar organisational models.
Data on race or ethnicity were not available in this retrospective cohort, as their collection is strictly regulated by law in France and rarely included in routine clinical datasets outside specific ethically approved research frameworks.
Finally, data were collected between 2021 and 2023, a period marked by the major 2022 RSV epidemic and the subsequent introduction of preventive strategies such as maternal vaccination and monoclonal antibody prophylaxis [20, 21]. Ongoing surveillance is warranted to confirm whether these evolving epidemiological trends affect future transport needs and team composition.
Implications for Practice
4.2
This study highlights the potential for advanced paediatric critical care nurses to safely conduct most inter‐hospital transfers of infants with moderate‐to‐severe bronchiolitis. Objective respiratory thresholds, particularly HFNC with FiO_2_ > 40% or CPAP with FiO_2_ > 35% or pCO_2_ > 65 mmHg, can guide team allocation during the regulation call, helping to identify which situations require a medicalised team. Implementing these evidence‐based criteria within triage protocols could enhance nurses' clinical autonomy, standardise decision‐making and improve the efficiency of emergency transport systems.
Expanding nurse‐led transfers may also optimise resource utilisation by preserving paediatricians for primary emergencies while maintaining patient safety. Ongoing training in ventilatory management, simulation exercises and strong interprofessional collaboration remain essential to consolidate these advanced competencies and ensure consistent, high‐quality care during paediatric retrieval.
Conclusion
5
Most inter‐hospital transfers of infants with moderate‐to‐severe bronchiolitis can be safely conducted by nurse‐led teams when predefined respiratory and blood gas thresholds are not exceeded. FiO_2_ and pCO_2_ values available at the regulation call provide simple and reliable indicators to guide team allocation. These findings support the development of standardised, evidence‐based triage protocols to strengthen nurses' autonomy and optimise resource use in paediatric emergency transport.
Future multicentre studies should assess the safety and cost‐effectiveness of this nurse‐led model in different organisational contexts and explore its integration into advanced nursing education, competency assessment and practice frameworks.
Author Contributions
A.G., A.G., C.M. and PETS' advanced paediatric critical care nurses contributed to the study conception and design. Analysis was performed by A.G. Material preparation and data collection were performed by all authors. The first draft of the manuscript was written by A.G., A.G., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
This work was supported by the Montpellier University Hospital, France.
Ethics Statement
Approved by the Institutional Review Board of Montpellier University Hospital (CSE‐2024‐06‐072, approval date: June 2024).
Consent
In accordance with French legislation, written informed consent from participants or their legal guardians was not required.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Fujiogi , T. Goto , H. Yasunaga , et al., “Trends in Bronchiolitis Hospitalizations in the United States: 2000‐2016,” Pediatrics 144 (2019): e 20192614, 10.1542/peds.2019-2614.31699829 PMC 6889950 · doi ↗ · pubmed ↗
- 2S. R. Dalziel , L. Haskell , S. O'Brien , et al., “Bronchiolitis,” Lancet 400 (2022): 392–406, 10.1016/S 0140-6736(22)01016-9.35785792 · doi ↗ · pubmed ↗
- 3C. Milési , S. Matecki , S. Jaber , et al., “6 cm H 2O Continuous Positive Airway Pressure Versus Conventional Oxygen Therapy in Severe Viral Bronchiolitis: A Randomized Trial,” Pediatric Pulmonology 48 (2013): 45–51, 10.1002/ppul.22533.22431446 · doi ↗ · pubmed ↗
- 4G. Cambonie , C. Milési , S. Jaber , et al., “Nasal Continuous Positive Airway Pressure Decreases Respiratory Muscles Overload in Young Infants With Severe Acute Viral Bronchiolitis,” Intensive Care Medicine 34 (2008): 1865–1872, 10.1007/s 00134-008-1201-x.18607564 · doi ↗ · pubmed ↗
- 5C. Milési , S. Essouri , R. Pouyau , et al., “High Flow Nasal Cannula (HFNC) Versus Nasal Continuous Positive Airway Pressure (n CPAP) for the Initial Respiratory Management of Acute Viral Bronchiolitis in Young Infants: A Multicenter Randomized Controlled Trial (TRAMONTANE Study),” Intensive Care Medicine 43 (2017): 209–216, 10.1007/s 00134-016-4617-8.28124736 · doi ↗ · pubmed ↗
- 6C. Milési , A.‐F. Pierre , A. Deho , et al., “A Multicenter Randomized Controlled Trial of a 3‐L/Kg/Min Versus 2‐L/Kg/Min High‐Flow Nasal Cannula Flow Rate in Young Infants With Severe Viral Bronchiolitis (TRAMONTANE 2),” Intensive Care Medicine 44 (2018): 1870–1878, 10.1007/s 00134-018-5343-1.30343318 · doi ↗ · pubmed ↗
- 7S. O'Brien , S. Craig , F. E. Babl , et al., ““Rational Use of High‐Flow Therapy in Infants With Bronchiolitis. What Do the Latest Trials Tell Us?” A Paediatric Research in Emergency Departments International Collaborative Perspective,” Journal of Paediatrics and Child Health 55 (2019): 746–752, 10.1111/jpc.14496.31270867 · doi ↗ · pubmed ↗
- 8D. Lavilledieu , H. Abassi , G. Mercier , et al., “Implementation of an Organizational Infrastructure Paediatric Plan Adapted to Bronchiolitis Epidemics,” Journal of Infection and Public Health 13 (2020): 167–172, 10.1016/j.jiph.2019.07.007.31378693 · doi ↗ · pubmed ↗