Evaluation of an infectious‑disease response training program for primary care physicians in Korea using Kirkpatrick’s 4 levels and the Context, Input, Process, and Product model: a mixed‑methods study
Kyung Hee Chun, Jin Seo Lee, Seon Young Jeong, Young Soon Park

TL;DR
This study evaluated a training program for Korean primary care physicians to improve their infectious disease response skills, finding it effective across multiple levels of assessment.
Contribution
The study integrates Kirkpatrick’s 4-level model and the CIPP framework to evaluate training effectiveness in infectious disease response for primary care physicians.
Findings
Training satisfaction was high (3.96±0.72) among participants.
Learning achievement showed significant improvement (F=12.922, P<0.001) from pre- to post-training.
Participants demonstrated motivation to apply new knowledge and institutional readiness for response strategies.
Abstract
This study systematically evaluated the effectiveness of a training program designed to enhance infectious disease response capabilities among primary care physicians. Using a mixed-methods design, the evaluation applied Kirkpatrick’s 4-level model and the Context, Input, Process, and Product (CIPP) framework to assess program outcomes and identify areas for improvement. The study focused on a national infectious disease training program for primary care physicians conducted in 2022 (N=1,718). Quantitative pre- and post-training data were analyzed from 100 randomly selected participants, along with qualitative data obtained through in-depth interviews with 10 participants. Validated assessment tools, developed by psychometricians and content experts, were used to measure satisfaction (Kirkpatrick level 1), learning achievement (level 2), practical application (level 3), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
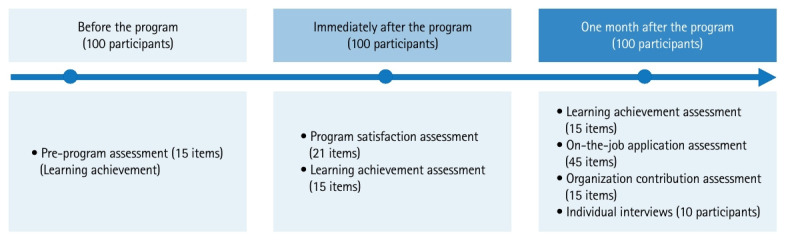 Figure 1
Figure 1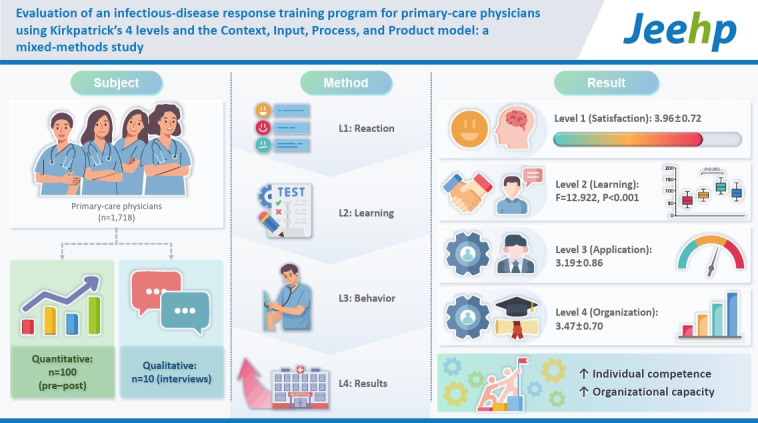 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Health Policy Implementation Science · Simulation-Based Education in Healthcare
Graphical abstract
Introduction
Background/rationale
The coronavirus disease 2019 (COVID-19) pandemic demonstrated that the response competency of healthcare professionals is a critical determinant of public health outcomes [1]. Although this recognition led to the introduction of new national-level training programs in Korea, substantial gaps persist across healthcare settings, and the overall support infrastructure remains limited [1,2]. The urgency of strengthening response capacity underscores the need for systematic and multidimensional evaluations to verify training effectiveness and inform continuous program improvement. Kirkpatrick’s 4-level model is a widely used evaluation framework that enables assessment of training transfer from learner reactions (Level 1) and learning outcomes (Level 2) to changes in workplace behavior (Level 3) and organizational results (Level 4) [3]. This model can be complemented by Stufflebeam’s Context, Input, Process, and Product (CIPP) model, a decision-oriented framework designed to assess program relevance, implementation quality, and overall effectiveness [4]. Despite the availability of these comprehensive models, prior evaluations have largely been limited to Level 1 (satisfaction) or Level 2 (learning achievement) outcomes [5-8]. Empirical evidence addressing Level 3 (behavioral change) and Level 4 (organizational impact) remains scarce, largely due to methodological and measurement challenges [9]. This limitation has hindered efforts to establish the true effectiveness of training programs.
Objectives
Accordingly, this study aimed to systematically evaluate the 2022 Korea Disease Control and Prevention Agency (KDCA)–supported training program for primary care physicians, focusing on infectious disease prevention and management. We applied a mixed-methods design using both Kirkpatrick’s 4-level model and the CIPP model to assess outcomes (including the often-overlooked Levels 3 and 4) and derive quality management strategies. This study was guided by the following research questions (RQs), aligned with Kirkpatrick’s 4 levels of evaluation:
(1) RQ1 (Level 1: reaction): What was the level of participant satisfaction with the infectious disease response training program?
(2) RQ2 (Level 2: learning): What was the impact of the training program on participants’ learning achievement?
(3) RQ3 (Level 3: behavior): What was the impact of the training program on participants’ practical application of learned content in their clinical practice?
(4) RQ4 (Level 4: results): What was the impact of the training program on organizational contributions?
Methods
Ethics statement
This study was conducted in strict adherence to research ethics and received approval from the Institutional Review Board (IRB) of Konyang University Hospital (IRB number: KYUH 2021-10-008-004). Written informed consent was obtained from all participants prior to study participation.
Study design
This study employed a mixed-methods design. A before-and-after study was conducted and reported in accordance with the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) statement, available at: https://www.cdc.gov/hivpartners/php/trend-statement/index.html. The quantitative component adopted Kirkpatrick’s 4-level model as the primary evaluative framework (Levels 1–4). Level 1 (reaction) evaluation assessed participants’ satisfaction with the training program, with subdomains constructed by integrating Stufflebeam’s CIPP model (Table 1). To assess the effectiveness of the training program at Level 2 (learning), Level 3 (behavior), and Level 4 (results), a pre- and post-test design with a 1-month follow-up assessment was implemented.
Setting
The training program was conducted from September 26 to October 26, 2022. Quantitative data corresponding to Levels 1–4 were collected using online self-report questionnaires at 3 time points: before the training (September–October 2022), immediately after the training (September–October 2022), and 1 month after the training (October–November 2022). Qualitative data were collected through individual Zoom interviews with high-achieving participants 1 month after the training, between November and December 2022.
Interventions
The intervention consisted of a 2-hour online continuing medical education (CME) program developed by 4 infectious disease specialists. Detailed information regarding the program structure and content is provided in Supplement 1.
Participants
The study population comprised 1,718 primary care physicians who participated in the 2022 infectious disease response training program. Among them, 864 individuals who provided consent for evaluation constituted the potential sampling frame. From this pool, 100 participants were selected using random sampling. Demographic analysis of the participants is shown in Table 2.
For the qualitative component (n=10), participants were purposively selected. This subsample (mean age, 53 years; 6 males and 4 females) included specialists in internal medicine (n=2), anesthesiology and pain medicine (n=2), family medicine (n=2), urology (n=2), obstetrics and gynecology (n=1), and pediatrics (n=1).
Variables
The intervention (exposure) was participation in the 2022 KDCA-supported infectious disease response online CME program for primary care physicians. The primary outcome was Kirkpatrick Level 2 (learning). Secondary outcomes included Kirkpatrick Level 1 (reaction), Kirkpatrick Level 3 (behavior), and Kirkpatrick Level 4 (results). Baseline characteristics and potential covariates included participant sex and clinical practice type (Table 2).
Data sources
Data collection took place in 2022 in accordance with the program schedule (Dataset 1). Quantitative data for Levels 1–4 were collected through online self-report surveys administered at the 3 predefined time points. Qualitative data were collected 1 month after the training through individual Zoom interviews with 10 participants, selected through purposive sampling based on high performance. This criterion was chosen to identify key informants who could provide rich, detailed insights into the successful application of the training and identify best practices, rather than to achieve statistical generalization.
Measurement
Level 1 (reaction) was assessed using a 21-item Training Satisfaction Survey developed specifically for this study by integrating Stufflebeam’s CIPP model. The model defined 4 subfactors: Context (necessity), Input (logistics), Process (operation and content), and Product (impact and satisfaction). All items were rated on a 5-point Likert scale. The reliability of the scale is presented in Table 3. Level 2 (learning) was assessed using a 15-item Learning Achievement Test comprising true/false and multiple-choice questions, administered at all 3 assessment points. Level 3 (behavior) was assessed at the 1-month follow-up using a 45-item Practical Application Survey (5-point Likert scale), which measured knowledge dissemination at the individual level and the implementation of response measures at the individual and organizational levels. Level 4 (results) was assessed at the 1-month follow-up using a 15-item Organizational Contribution Survey (5-point Likert scale), which evaluated perceived organizational contribution as a proxy indicator of organizational readiness and system enhancement.
All 4 quantitative instruments (Levels 1–4) were developed specifically for this study. Items were drafted based on existing literature ([10] for Level 1) and consultations with 2 psychometrics experts. Content validity was established through a rigorous expert panel review involving 2 education specialists and 2 infection control specialists. Items were finalized only when all 4 experts rated them as appropriate (defined as ≥4 on a 5-point scale). For the qualitative component, a semi-structured interview guide was developed based on the CIPP framework to derive specific recommendations for program improvement. The content validity of the interview guide was reviewed and refined by 2 education experts.
Bias
Selection bias is possible because participation in the national training program and consent for evaluation were voluntary; therefore, evaluated participants may have differed systematically from nonparticipants (e.g., higher motivation or greater baseline interest in infection control). To reduce additional selection bias within the evaluation, the quantitative analytic sample was randomly selected from the pool of consenting trainees. However, residual self-selection into both the program and the consent process may still limit the generalizability of the findings.
Information (measurement) bias may have affected Kirkpatrick Levels 1, 3, and 4 because these outcomes relied on self-reported Likert-scale responses, which are vulnerable to social desirability and recall effects. To mitigate these concerns, standardized instruments with explicit anchors were used, and outcomes were assessed at prespecified time points (immediately post-training and at the 1-month follow-up) to minimize long recall intervals. For Level 2, the use of an objective knowledge test reduced susceptibility to social desirability bias relative to self-reported outcomes.
For the qualitative component, sampling bias is possible because interviewees were purposively selected as high performers. While this approach increased the depth of insight into successful implementation, it may have underrepresented barriers experienced by average or lower-performing participants. This limitation should be considered when interpreting the transferability of the qualitative themes.
Study size
The sample size was determined to ensure sufficient statistical power for the analysis while optimizing data collection efficiency. A priori power analysis indicated power exceeding 95% to detect a medium effect size in repeated-measures analysis of variance (ANOVA). The analysis was conducted using G*Power ver. 3.1 (F test, repeated-measures ANOVA: within factors; Heinrich-Heine-Universität Düsseldorf). Given the single-group design, the number of groups was set to 1. For the power calculation, within-subject changes across 3 time points (pre-intervention, immediately post-intervention, and 1-month follow-up) were modeled for the primary outcome, the learning achievement score. Assuming a medium effect size (f=0.25), a significance level (α) of 0.05, statistical power of 0.95, and a correlation among repeated measures of 0.5, the minimum required sample size was n=43. The final analytic sample in this study (n=100) substantially exceeded this requirement.
There was no investigator-controlled assignment to intervention versus comparison conditions. All trainees received the same training program as implemented at the national level.
Unit of analysis
The unit of analysis for the quantitative component was the individual physician participant. For the qualitative component, the unit of analysis was also the individual interviewee, and themes were derived from interview transcripts using a CIPP-informed analytic framework.
Qualitative research
In-depth interviews were conducted using a semi-structured interview guide developed based on the CIPP model. This approach was designed to explore participants’ experiences and perceptions that are difficult to capture through structured surveys alone. Through this process, the Process and Product components were examined in greater depth, including learners’ actual experiences, the appropriateness of program operations, and perceived organizational impacts. This qualitative inquiry complemented the quantitative findings and supported the derivation of specific strategies for program improvement. A mixed-methods approach aligned with Kirkpatrick’s model is shown in Table 4.
Statistical methods
All quantitative data were analyzed using IBM SPSS Statistics ver. 25.0 (IBM Corp.). Descriptive statistics, including frequencies, means, and standard deviations, were calculated. Repeated-measures ANOVA was used to compare mean scores across the 3 assessment time points. Qualitative data were transcribed verbatim and analyzed using a thematic analysis approach, with the CIPP model applied as an a priori analytical framework. To enhance trustworthiness, coding results were cross-checked by 2 education experts through peer debriefing, and key findings were verified through member checking.
Results
Participants
Fig. 1 shows the flow diagram of the present study.
Main results
Level 1: Reaction (training satisfaction)
Overall satisfaction with the training program was high (mean=3.96±0.72). As shown in Table 5, participants reported the highest levels of satisfaction for Product items (e.g., willingness to recommend or reattend the program), whereas relatively lower scores were observed for Process items (e.g., program volume and difficulty). Qualitative interviews triangulated these quantitative findings, confirming strong motivation (Context) and high overall satisfaction (Product; mean score 8.5/10). Participants also offered specific and actionable feedback related to Input (e.g., pre-distribution of learning materials) and Process (e.g., the need for adjustable difficulty levels and access to on-demand recordings).
Level 2: Learning achievement
As presented in Table 6, repeated-measures ANOVA demonstrated a significant main effect of time on learning achievement (F(2, 198)=12.922, P<0.001, partial ηp^2^=0.115). Post hoc pairwise comparisons using Bonferroni correction indicated that learning achievement scores measured immediately after the intervention and at the 1-month follow-up were significantly higher than pre-intervention scores.
Qualitative interviews further contextualized these results by emphasizing the high relevance and immediate applicability of the content. A key theme was the program’s utility in systematically organizing participants’ existing knowledge. Modules addressing practical prevention strategies (learning outcome [LO]-B) and disease reporting procedures (LO-C) were perceived as particularly useful. Although some participants described the equipment reprocessing module (LO-D) as “dull,” others identified it as new and essential information, underscoring variability in prior knowledge and learning needs (Table 7).
Level 3: Practical application (behavior)
Level 3 evaluation, conducted at the 1-month follow-up, yielded a mean score of 3.19±0.86 for individual-level knowledge dissemination (Table 8, Supplement 2). A bimodal response pattern was observed: for common topics (e.g., COVID-19), the most frequent response was “mostly educated” (Level 4), whereas for less common topics (e.g., mpox), the most frequent response was “willing to educate” (Level 3). This pattern suggests a strong motivational effect of the training program. At the individual–organizational level (Table 9, Supplement 3), application of learned content was consistently rated at the “basic” level (Level 3) for both the development (mean=3.13) and implementation (mean=3.13) of response measures across topic categories.
In-depth interviews strongly supported these Level 3 findings, highlighting significant behavioral and attitudinal shifts after the program.
Application of practical knowledge: Participants reported an enhanced state of vigilance. “I learned about the infection control manuals, the proper disinfection procedures, and precautions when treating patients. I now approach (COVID) patients with a heightened sense of awareness.” (A4, A8).
Enhanced patient response competency: The training translated directly into confidence in practice. “Because I learned the knowledge, I can respond to patients with practical confidence and evidence,” and “It was helpful for correcting patients’ misconceptions; I gained confidence in explaining (these topics) to them.” Another noted, “I am using the content for resident and student education.” (A1, A2, A3, A5, A6, A7).
Shift in interprofessional perception: The training also fostered new attitudinal changes. “I used to take it for granted that the nurse cleans up after an endoscopy. After the training on medical equipment reprocessing, I realized how hard they [the nurses] work. I felt a new gratitude for my colleagues and have become more considerate.” (A10).
Level 4: Organizational contribution (results)
Level 4 assessment results indicated a positive perceived organizational contribution, with an overall mean score of 3.47±0.70 (Table 10). Participants generally agreed that the program led to tangible increases in awareness and implementation of infection control practices among colleagues and patients, particularly in relation to aerosol prevention (mean=3.60±0.79) and sterilization practices (mean=3.61±0.71).
The interviews provided concrete examples of participants functioning as knowledge brokers and agents of change within their organizations. One participant stated, “I delivered the mpox information to our manager … [and] shared the sterilization knowledge with staff in dentistry and clinical pathology, which helped strengthen our multi-departmental infection control system” (A5).
Another described standardizing departmental practices: “I standardized our department’s infection control practices by creating and distributing a 1-page A4 manual” (A6).
Finally, participants identified a critical future direction for program development: expansion of the training to include nurses and other healthcare staff. This interprofessional approach was viewed as essential for strengthening infection control capacity across the entire organizational system (A7, A8).
Discussion
Key results
This mixed-methods study confirmed the effectiveness of the training program across all 4 Kirkpatrick levels. The evaluation demonstrated high satisfaction (Level 1), significant and sustained learning (Level 2), and, most critically, clear evidence of translation into practice (Level 3) and perceived organizational contribution (Level 4). Participants not only acquired knowledge but also reported increased confidence, improved interprofessional appreciation, and active engagement as change agents within their organizations. In addition, the CIPP-based analysis identified actionable areas for improvement, particularly within the Process domain (e.g., program volume and difficulty), thereby demonstrating the added value and synergy of applying both evaluation models concurrently.
Interpretation
The consistently positive outcomes across all 4 levels suggest that the program’s impact successfully extended from individual learners to the organizational level. The favorable findings at Levels 3 and 4 provide critical evidence that learning outcomes bridged the gap between knowledge acquisition and real-world performance, with meaningful implications for infection control capacity and organizational culture. Furthermore, this study underscores the synergistic value of applying the CIPP model alongside the Kirkpatrick model. While the Kirkpatrick framework confirmed program effectiveness, the CIPP model offered a diagnostic perspective that elucidated how and why the program functioned effectively, yielding specific and actionable strategies for quality management.
However, varying degrees of application were observed across topic areas. The relatively lower scores for mpox-related items in perceived practical application (Level 3) and organizational contribution (Level 4) appear attributable to 2 primary factors. First, at the time of training and analysis, the likelihood of encountering mpox in routine primary care settings was low, resulting in limited perceived relevance. Second, compared with high-frequency and high-risk infectious diseases such as COVID-19, the perceived urgency of responding to mpox was lower. Consequently, the impetus to translate learned content into immediate practice was less pronounced. These findings suggest that the behavioral impact of infectious disease training may vary according to the urgency and contextual relevance of specific topics within real-world clinical environments. Accordingly, when designing CME programs at national or regional levels, careful consideration should be given to aligning educational content and timing with prevailing public health priorities and clinical needs.
Comparison with previous studies
The findings of this study align with existing literature indicating that infectious disease training enhances not only healthcare professionals’ knowledge and skills but also the transfer of learning into clinical practice [11,12]. Prior studies have further shown that repetitive and participatory training approaches improve knowledge retention and strengthen intentions to implement infection control practices [13,14]. However, a notable limitation of much of the previous research is its emphasis on short-term outcomes, often restricted to Kirkpatrick Levels 1 or 2 [5-8]. A key distinguishing feature of the present study is its longitudinal and multidimensional evaluation. By incorporating a 1-month follow-up assessment and qualitative interviews, this study was able to demonstrate not only sustained learning (Level 2) but also tangible behavior change (Level 3). Moreover, the identification of perceived organizational-level effects (Level 4), including changes in awareness and the adoption of standardized practices, represents an outcome rarely documented in prior studies. These findings suggest that well-designed infectious disease training programs can function as catalysts for improvement, extending beyond individual competency to foster broader enhancements in organizational infection control culture.
Limitations
This study has several limitations that warrant consideration. First, selection bias arising from voluntary participation may limit generalizability. Although 100 participants were randomly selected from a larger pool of 864 consenting individuals, sampling bias cannot be entirely excluded, and the findings should therefore be interpreted cautiously. Second, the qualitative component relied on purposive sampling of the top 10 performers in the quantitative assessment. While the strong Level 3 and Level 4 outcomes underscore the program’s potential effectiveness, these findings may partly reflect the exceptional baseline characteristics of highly motivated participants. As a result, the experiences and challenges of middle- and lower-performing participants may not have been fully captured, limiting the representativeness of the qualitative insights. Third, reliance on self-reported measures for Levels 3 and 4 introduces the possibility of social desirability bias. In particular, the assessment of Level 4 (results) was based on participants’ perceived organizational impact rather than objective indicators such as return on investment or infection rate metrics. Although collecting such objective data in dispersed primary care settings is inherently challenging, prior research suggests that perceived organizational readiness may serve as a meaningful leading indicator of actual response performance during public health crises [15]. Fourth, the 1-month follow-up period may be insufficient to confirm long-term sustainability of behavioral and organizational change. Longer follow-up intervals of 3 to 6 months or more are generally recommended to assess enduring changes in practice and system-level performance. Finally, the intervention was a web-based program developed by infectious disease specialists and delivered as four 30-minute modules with interactive components and quizzes. Although overall satisfaction was high, feedback indicated a relative need for refinement in program volume, difficulty, and content alignment. To further strengthen field-based infection response competencies, future programs should incorporate diverse educational modalities beyond online delivery, including practice-oriented and problem-solving-focused offline training such as simulations or tabletop exercises.
Notwithstanding these limitations, the mixed-methods design of this study provided a comprehensive and multidimensional assessment of the training program’s effectiveness.
Suggestion for further studies
Based on these findings, several directions for future research are proposed. First, longitudinal studies are needed to validate the long-term sustainability of learning transfer and behavioral change. Second, future research should prioritize the development of objective assessment tools (e.g., observational checklists or audit-based indicators) to more rigorously evaluate Kirkpatrick Levels 3 and 4. Third, the intervention itself should be further refined through the development of customized modules with adjustable levels of difficulty to better accommodate diverse learner needs. In addition, exploration of hybrid or blended learning models is recommended to enhance learner engagement and facilitate practical application.
The core workforce for infection response is not limited to physicians but includes a broad range of healthcare personnel, such as nurses, administrative staff, and environmental services staff. Accordingly, effective training programs should be expanded to address this wider healthcare workforce. Moreover, given the persistent threat of emerging infectious diseases, effective management increasingly depends on interprofessional collaboration and coordinated response efforts, underscoring the importance of interprofessional education. Ultimately, continued efforts are needed to develop diverse infection response training programs, conduct systematic and theory-informed evaluations, and disseminate successful outcomes to the broader healthcare community.
Conclusion
This study empirically demonstrated that an infectious disease response training program for primary care physicians can produce substantive outcomes that extend beyond the individual learner. The program not only improved participant satisfaction (Level 1) and learning achievement (Level 2) but also translated into demonstrable behavioral changes in clinical practice (Level 3) and tangible contributions at the organizational level (Level 4). By integratively applying Kirkpatrick’s 4-level model to assess learning transfer and the CIPP model to guide program improvement, this research provided detailed insights into the mechanisms underlying effective learning transfer and identified clear pathways for quality enhancement. This dual-model approach offers a valuable contribution to the advancement of evaluation frameworks in health professions education. Ultimately, the findings of this study illustrate that infectious disease response training is not merely a vehicle for knowledge dissemination but a practical and impactful intervention capable of strengthening both the professionalism of healthcare providers and the overall response capacity of healthcare organizations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Korea Disease Control and Prevention Agency Development and operation plan of national disaster response education curriculum: focusing on infectious disease crisis response education [Internet]Korea Disease Control and Prevention Agency 2021[cited 2025 Feb 5]. Available from: https://www.rihp.re.kr/bbs/board.php?bo_table=research_report&wr_id=323&sfl=wr_subject&stx=%EA%B 5%AD%EA%B 0%80+%EC%9E%AC%EB%82%9C+%EB%8C%80%EC%9D%91%EC%9D%84+%EC%9C%84%ED%95%9C+%EA%B 5%90%EC%9C%A 1%EA%B 3%BC%EC%A 0%95+%EA%B 0%9C%
- 2Park YM Coronavirus volunteer group planned to recruit 5,000 in 2 weeks but gathered only 500 after 3 weeks. Medical Times [Internet]2020 Dec 12[cited 2025 Feb 5]. Available from: https://www.medicaltimes.com/Users/News/News View.html?ID=1137696
- 3Kirkpatrick DL Kirkpatrick JD Evaluating training programs: the four levels 3rd ed Berrett-Koehler Publishers 2006
- 4Stufflebeam DL The CIPP model for program evaluation Madaus GF Scriven M Stufflebeam DL Evaluation models: viewpoints on educational and human services evaluation Springer 198311714110.1007/978-94-009-6669-7_1 · doi ↗
- 5Aljahany M Alassaf W Alibrahim AA Kentab O Alotaibi A Alresseeni A Algarni A Algaeed HA Aljaber MI Alruwaili B Aljohani K Use of in situ simulation to improve emergency department readiness for the COVID-19 pandemic Prehosp Disaster Med 202136613 https://doi.org/10.1017/S 1049023 X 2000134 X 10.1017/S 1049023 X 2000134 X 33081859 PMC 7653231 · doi ↗ · pubmed ↗
- 6Li L Lin M Wang X Bao P Li Y Preparing and responding to 2019 novel coronavirus with simulation and technology-enhanced learning for healthcare professionals: challenges and opportunities in China BMJ Simul Technol Enhanc Learn 20206196198 https://doi.org/10.1136/bmjstel-2020-000609 10.1136/bmjstel-2020-00060932832099 PMC 7410111 · doi ↗ · pubmed ↗
- 7Kim Y Gwack J Kwon Y Cheong MJ Lee JH Needs assessment for public health competency in infection prevention and control: importance and performance analysis (IPA) of infectious disease response practitioners J Korean Med Sci 202540 e 23 https://doi.org/10.3346/jkms.2025.40.e 23 10.3346/jkms.2025.40.e 2339763309 PMC 11707661 · doi ↗ · pubmed ↗
- 8Yu M Kim EK Kim K Lee J Jeon JH Kim S Lee S Kwon Y Development and evaluation of the Korea Disease Control and Prevention Agency's scenario-based training program for effective response to emerging infectious disease outbreaks Osong Public Health Res Perspect 202516373380 https://doi.org/10.24171/j.phrp.2025.0103 10.24171/j.phrp.2025.010340629962 PMC 12666395 · doi ↗ · pubmed ↗