Expanding Access to Orthopedic Trauma Care: Evaluation of a Task‐Sharing Model With a Remote Quality Assessment Tool for Open Tibia Shaft Fractures in Malawi
Leonard Banza, Olaf Bach, Faith Moyo, Claude Martin, William Harrison

TL;DR
A task-sharing model for treating open tibia fractures in Malawi showed good results at central hospitals but struggled at district hospitals due to lack of support.
Contribution
The study introduces a remote quality assessment tool (FFATEF) and evaluates a task-sharing model for orthopedic trauma care in low-resource settings.
Findings
Central hospitals achieved higher FFATEF scores (median 10.0) compared to district hospitals (median 6.0).
Satisfactory technical performance (≥8 FFATEF score) was 93% at central hospitals but only 32% at district hospitals.
Preoperative antibiotic compliance was 100% at central hospitals versus 47% at district hospitals.
Abstract
Timely care for open tibia fractures remains difficult in low‐resource settings. We evaluated a task‐sharing model in Malawi in which trained orthopedic clinical officers (OCOs) delivered external fixation supported by a remote quality assessment tool. We conducted a prospective implementation evaluation across one central and four district hospitals (May 2023–July 2024). The intervention bundled OR refurbishment assured external fixator supply, refresher training, mentoring (on‐site and remote), national guideline reinforcement, and a novel Fracture Fixation Assessment Tool for External Fixation (FFATEF). OCOs submitted postoperative radiographs and construct photographs for scoring across four domains (reduction, stability, implantation, and surgical impression; total 0–12 and satisfactory ≥ 8). Nonparametric tests compared performance by the hospital type; temporal trends were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
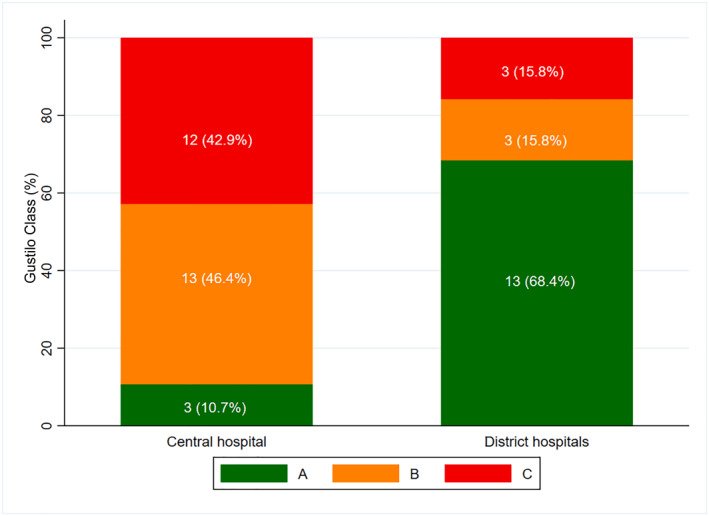 FIGURE 1
FIGURE 1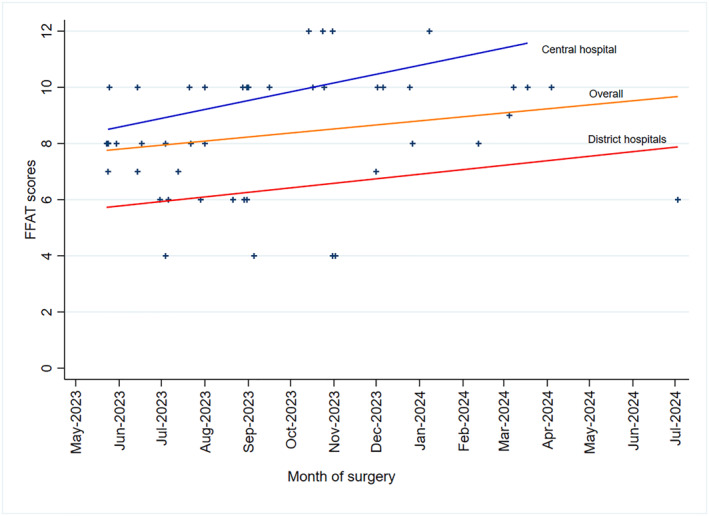 FIGURE 2
FIGURE 2| Domain | 0 (Poor) | 1 (Fair) | 2 (Good) | 3 (Excellent) |
|---|---|---|---|---|
| Reduction | Gross malalignment (> 10°/obvious translation) | Residual deformity 6°–10° or translation | ≤ 5° angulation and minimal translation | Anatomic alignment and axes restored |
| Stability | Insecure frame and obvious looseness | Some instability and questionable pin spread | Adequate stability and acceptable pin spread | Rigid construct and optimal pin spread and triangulation |
| Implantation | Pins near wound and multiple avoidable conflicts | Suboptimal pin placement and minor conflicts | Good pin position and safe corridors mostly respected | Ideal pin position, safe corridors, and soft tissues protected |
| Surgical impression | Poor technique and contamination risk | Technique acceptable with notable issues | Competent technique and minor issues only | Flawless technique and meticulous execution |
| Characteristic | Central ( | District ( | Total ( |
|---|---|---|---|
| Male sex— | 25 (89%) | 17 (89%) | 42 (89%) |
| Age—mean (years) | 32.3 | 32.3 | 32.3 |
| Motorcycle‐related injury— | 12 (43%) | 8 (42%) | 20 (42.6%) |
| Gustilo IIIA/B— | 16 (69.6%) | 3 (15.8%) | 19 (40.4%) |
| Time injury→surgery—median (days) | 1 | 2 | — |
| Pre‐op antibiotics— | 28 (100%) | 9 (47%) | 37 (78.7%) |
| Open tibia shaft fracture— | 28 (100%) | 19 (100%) | 47 (100%) |
| Outcome | Central | District |
|---|---|---|
| Total FFATEF—median (IQR) | 10 (9–11) | 6 (5–8) |
| Satisfactory (≥ 8)— | 26/28 (93%) | 6/19 (32%) |
| Trend over time (Spearman | 0.52; 0.005 | 0.15; 0.540 |
| Predictor | Odds ratio | 95% CI |
|
|---|---|---|---|
| Central hospital (vs. district) | 28.5 | 5.2–156.3 | < 0.001 |
| Gustilo grade (per grade increase) | 0.42 | 0.19–0.93 | 0.032 |
- —AO Alliance Foundation
- —Johnson and Johnson Foundation10.13039/100020137
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health and Surgery · Trauma and Emergency Care Studies · Bone fractures and treatments
Introduction
1
Open fractures are bellwether conditions for emergency surgical capacity and are highly time‐sensitive [1, 2]. Access to surgical care in low‐ and middle‐income countries is constrained by multiple contextual challenges [3], and open tibia fractures represent a significant burden in settings such as Malawi [4]. Task sharing—collaborative care by mixed cadres under supervision—has been proposed to expand access in low‐ and middle‐income countries [5, 6, 7, 8, 9]. In Malawi, orthopedic clinical officers (OCOs) have delivered essential orthopedic care for over two decades [10], yet evidence on their performance for complex trauma outside tertiary centers remains limited [11]. We report a prospective evaluation of a bundled task‐sharing program for open tibia shaft fractures across five hospitals, incorporating a remote quality assessment tool to guide mentoring.
Methods
2
Study design and setting: During prospective implementation evaluation in one central (Zomba) and four district hospitals (Dowa, Machinga, Ntcheu, and Salima) from May 2023 to July 2024, it was found that eligible cases were skeletally mature patients with open tibia fractures.
Intervention: Operating room refurbishment, assured external fixator supply chain [12], refresher training for OCOs [13], reinforcement of national guidelines [14, 15], a multimodal mentoring package (quarterly visits, remote reviews within 72 h, case conferences, and on‐call phone support), and the FFATEF remote assessment tool were involved.
FFATEF: Adapted from the Fracture Fixation Assessment Tool [16, 17], FFATEF scores four domains—reduction, stability, implantation, and overall surgical impression—each 0–3; total 0–12 with satisfactory performance defined a priori as ≥ 8 (Table 1). OCOs uploaded postoperative AP/lateral radiographs and construct photos plus AO/OTA [18] and Gustilo [19] classifications and intent (temporary vs. definitive). A national trauma surgeon performed all primary ratings; a second surgeon independently rated a subset (κ = 0.76) indicating substantial agreement.
Outcomes and analysis: Primary outcome was the total FFATEF score. Nonparametric statistics (Mann–Whitney U and Fisher exact) compared sites; Spearman ρ tested trends. An ordinal logistic model explored correlates of satisfactory performance controlling for injury severity and time. Analyses used Stata 17. Ethics of local audit approval were conducted as per national guidance.
Results
3
Case mix and access: 47 patients were treated—28 at the central and 19 at district hospitals (Table 2). Motorcycle‐related injuries comprised 42.6%. Central cases were more complex (Gustilo IIIA/B 69.6% vs. 15.8%). Time from injury to surgery was shorter at the central site (median 1 day) than districts (2 days). Preoperative antibiotics were administered in 100% versus. 47% of cases, respectively.
Technical quality: Median FFATEF scores were higher at the central hospital (10.0 [IQR 9–11]) than district hospitals (6.0 [7, 8, 10, 11] and p < 0.001; Figure 1, and Table 3). Satisfactory scores (≥ 8) occurred in 26/28 (93%) central versus 6/19 (32%) district cases. Across domains, central cases scored higher for reduction, stability, implantation, and surgical impression (all p < 0.01). Central performance improved over time (ρ = 0.52 and p = 0.005); district scores showed no temporal change (ρ = 0.15 and p = 0.540; Figure 2).
Gustilo Anderson open fracture classification grade among injury cases stratified by the treating hospital (N = 47). Stacked bar chart showing the distribution of AO/OTA fracture classifications (A, B, and C) at the central hospital versus district hospitals. At the central hospital (n = 28)—Type A 3 (10.7%), Type B 13 (46.4%), and Type C 12 (42.9%). At district hospitals (n = 19)—Type A 13 (68.4%), Type B 3 (15.8%), and Type C 3 (15.8%).
Distribution of FFATEF scores by the type of health facility and the trend over time. Scatter plot with linear trend lines showing FFATEF scores (y‐axis, 0–12) over time from May 2023 to July 2024 (x‐axis). Central hospital scores (blue) show an upward trend (ρ = 0.52 and p = 0.005); overall scores (orange) show moderate improvement, whereas district hospital scores (red) show no significant temporal change (ρ = 0.15 and p = 0.540).
Regression: Treatment at the central hospital was independently associated with higher odds of satisfactory FFATEF (OR 28.5, 95% CI 5.2–156.3, and p < 0.001), whereas higher Gustilo grade reduced the odds (OR 0.42 per grade, 95% CI 0.19–0.93, and p = 0.032; Table 4).
Discussion
4
This evaluation suggests that task sharing for open tibia external fixation can achieve satisfactory technical quality when delivered within integrated teams and adequate infrastructure, consistent with recent efforts to improve open fracture care in Malawi [20], but district‐level performance remained suboptimal despite training and remote reviews. Contributors likely include case volume and exposure, equipment availability (e.g., lack of fluoroscopy), team support, and inconsistent referral adherence. These findings support a shift from simple task shifting to true task sharing resulting in progressive scope, stronger mentoring cadence, and institutional prerequisites.
Policy and program implications involve (1) graduated implementation focusing initially on lower complexity cases, (2) minimum infrastructure standards (lighting, sterilization, instrumentation, and imaging where feasible), (3) defined mentoring intensity (e.g., weekly case reviews and periodic on‐site supervision), (4) real‐time quality monitoring using concise tools adaptable for local use and (5) robust referral networks matched to facility capability. Economic assessment is needed to compare decentralized care plus support versus strengthened centralization and transport systems.
Limitations include modest sample size, nonrandomized design, process‐oriented primary outcome, and lack of infection/union/function endpoints; future studies should assess long‐term functional outcomes as demonstrated elsewhere in Malawi [21]. FFATEF requires validation against patient outcomes and streamlining for routine adoption.
Conclusions
5
Task sharing for complex orthopedic trauma requires more than short‐course training. Central hospital embedding with integrated teams was associated with high rates of satisfactory technical performance, whereas district hospitals lagged in technical performance. Safe scale‐up will likely depend on institutional prerequisites, intensified mentoring, adherence to referral criteria, and continuous quality assurance. Future work should validate FFATEF against clinical outcomes and evaluate cost‐effectiveness of delivery models.
Author Contributions
L.B. and O.B.: investigation, supervision, writing – review and editing. W.H.: conceptualization, methodology, supervision, writing – review and editing. F.M.: formal analysis, validation, writing – review and editing. C.M.: funding acquisition, project administration, writing – original draft and review.
Funding
Johnson & Johnson Foundation Long Bone Fracture Program, KidsOR UK, and AO Alliance Foundation; funders had no role in study design, data collection, analysis, or reporting.
Ethics Statement
Local audit approval from Kamuzu Central Hospital Research Committee (KCHRC/001/23) was conducted in accordance with the Declaration of Helsinki, Good Clinical Practices, and national guidance.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. G. Meara , A. J. Leather , L. Hagander , et al., “Global Surgery 2030: Evidence and Solutions for Achieving Health, Welfare, and Economic Development,” Lancet 386, no. 9993 (2015): 569–624, 10.1016/s 0140-6736(15)60160-x.25924834 · doi ↗ · pubmed ↗
- 2P. Joosten , M. Noorlander‐Borgdorff , M. Botman , M. B. Bouman , D. Embden , and G. Giannakopoulos , “Comparing Outcomes Following Direct Admission and Early Transfer to Specialized Trauma Centres in Open Tibial Fracture Treatment: A Systematic Review and meta‐analysis,” European Journal of Trauma and Emergency Surgery 50 (2023): 1–10, 10.1007/s 00068-023-02366-x.PMC 1103541237776341 · doi ↗ · pubmed ↗
- 3N. P. Raykar , R. R. Yorlets , C. Liu , et al., “A Qualitative Study Exploring Contextual Challenges to Surgical Care Provision in 21 LMI Cs,” supplement, Lancet 385, no. S 2 (2015): S 15, 10.1016/s 0140-6736(15)60810-8.PMC 480346826313061 · doi ↗ · pubmed ↗
- 4K. Mwafulirwa , R. Munthali , I. Ghosten , and A. Schade , “Epidemiology of Open Tibia Fractures Presenting to a Tertiary Referral Centre in Southern Malawi: A Retrospective Study,” Malawi Medical Journal 34, no. 2 (2022): 118–122, 10.4314/mmj.v 34i 2.7.35991814 PMC 9356523 · doi ↗ · pubmed ↗
- 5W. Alemayehu , M. Melese , A. Bejiga , et al., “Surgery for Trichiasis by Ophthalmologists Versus Integrated Eye Care Workers: A Randomized Trial,” Ophthalmology 111, no. 3 (2004): 578–584, 10.1016/j.ophtha.2003.06.030.15019339 · doi ↗ · pubmed ↗
- 6J. Gajewski , M. Cheelo , L. Bijlmakers , J. Kachimba , C. Pittalis , and R. Brugha , “The Contribution of Non‐Physician Clinicians to the Provision of Surgery in Rural Zambia—A Randomized Controlled Trial,” Human Resources for Health 17, no. 1 (2019): 60, 10.1186/s 12960-019-0398-9.31331348 PMC 6647149 · doi ↗ · pubmed ↗
- 7C. Mc Cord , G. Mbaruku , C. Pereira , C. Nzabuhakwa , and S. Bergstrom , “The Quality of Emergency Obstetrical Surgery by Assistant Medical Officers in Tanzanian District Hospitals,” Health Affairs 28, no. 5 (2009): w 876–w 885, 10.1377/hlthaff.28.5.w 876.19661113 · doi ↗ · pubmed ↗
- 8T. J. Wilhelm , I. K. Thawe , B. Mwatibu , H. Mothes , and S. Post , “Efficacy of Major General Surgery Performed by Non‐physician Clinicians at a Central Hospital in Malawi,” Tropical Doctor 41, no. 2 (2011): 71–75, 10.1258/td.2010.100272.21303987 · doi ↗ · pubmed ↗