Effect of chlorhexidine pretreatment on clinical performance of adhesive restorations: a systematic review and meta-analysis
Rim Bourgi, Ahmed A. Holiel, Carlos Enrique Cuevas-Suárez, Miguel Ángel Fernández-Barrera, Evandro Piva, Louis Hardan, Tatiana Roman, Naji Kharouf, Youssef Haikel

TL;DR
This study finds that using chlorhexidine before dental restorations does not significantly improve their long-term performance, despite its ability to inhibit enzymes in lab settings.
Contribution
The study provides the first systematic review and meta-analysis on the clinical effectiveness of chlorhexidine pretreatment for resin-based dental restorations.
Findings
No significant difference in restoration retention between chlorhexidine and control groups.
No significant impact on postoperative sensitivity or secondary caries.
Current evidence does not support routine use of chlorhexidine with etch-and-rinse adhesives.
Abstract
The long-term stability of resin–dentin adhesion remains a major concern in restorative dentistry. Hydrolytic and enzymatic degradation of the hybrid layer contributes to the deterioration of resin-bonded restorations. Inhibition of matrix metalloproteinases (MMPs) by chlorhexidine digluconate (CHX) has been proposed to preserve the hybrid layer and improve adhesive durability. This systematic review and meta-analysis evaluated the effect of dentin pretreatment with CHX on the clinical performance and longevity of resin-based restorations compared with no CHX application. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, electronic searches were conducted in PubMed, Scopus, Web of Science, and the Cochrane Library up to September 2025. Randomized and non-randomized clinical trials assessing CHX pretreatment before adhesive application…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
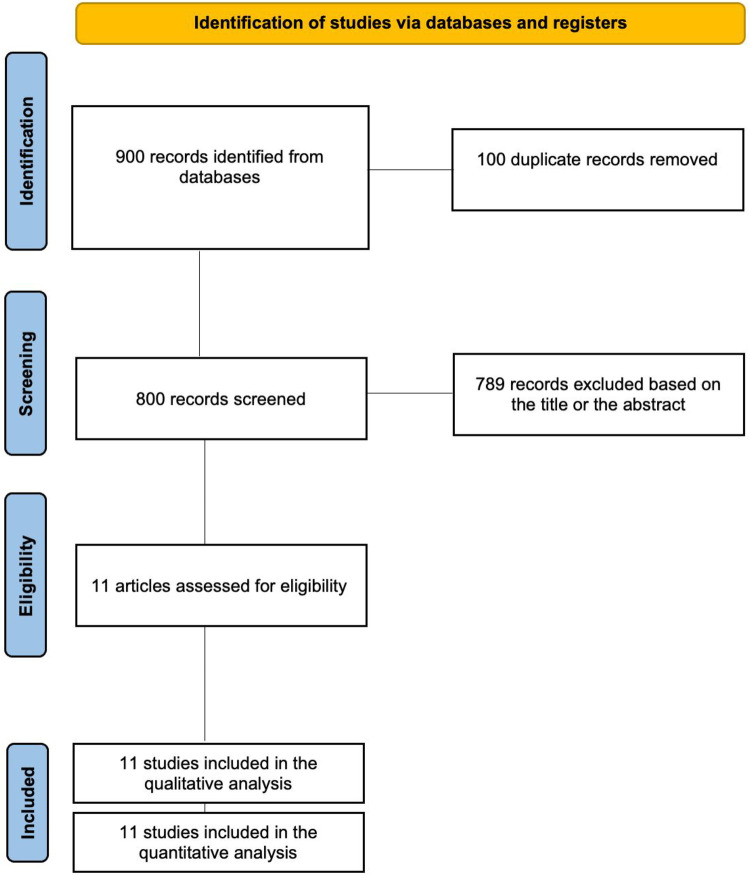 Figure 1
Figure 1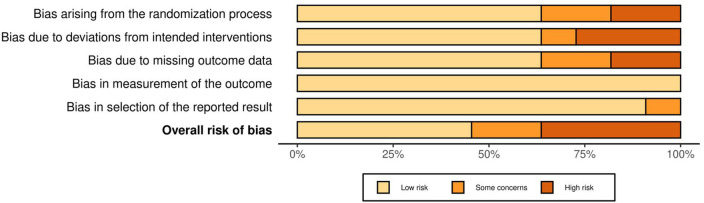 Figure 2
Figure 2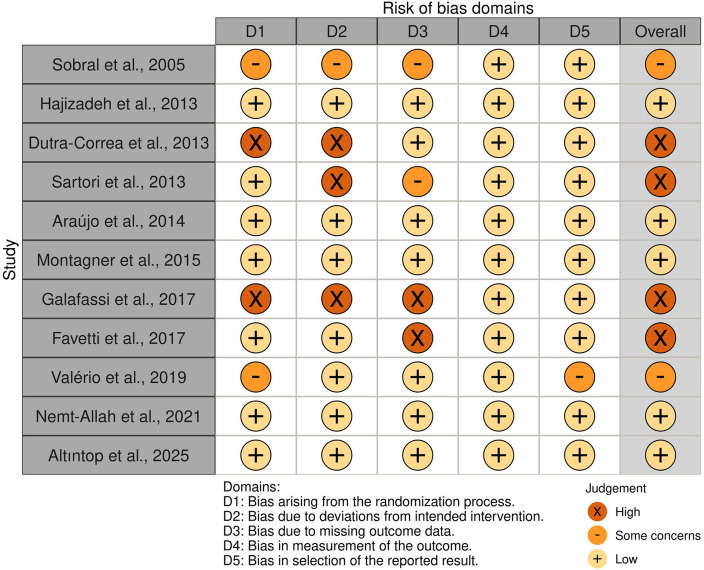 Figure 3
Figure 3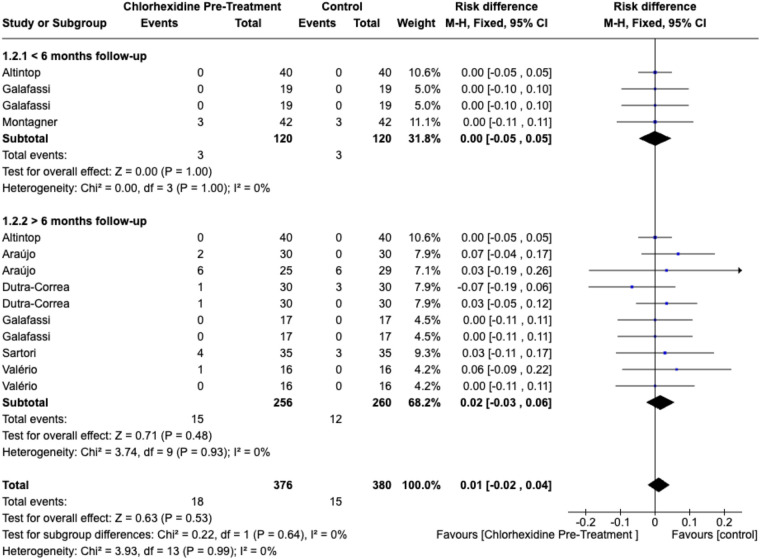 Figure 4
Figure 4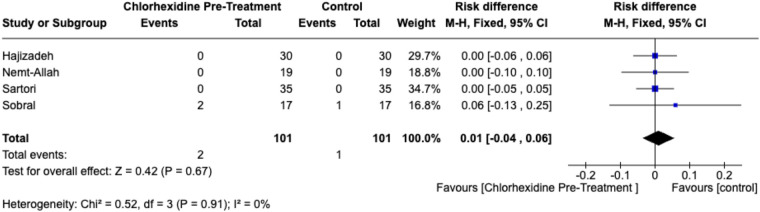 Figure 5
Figure 5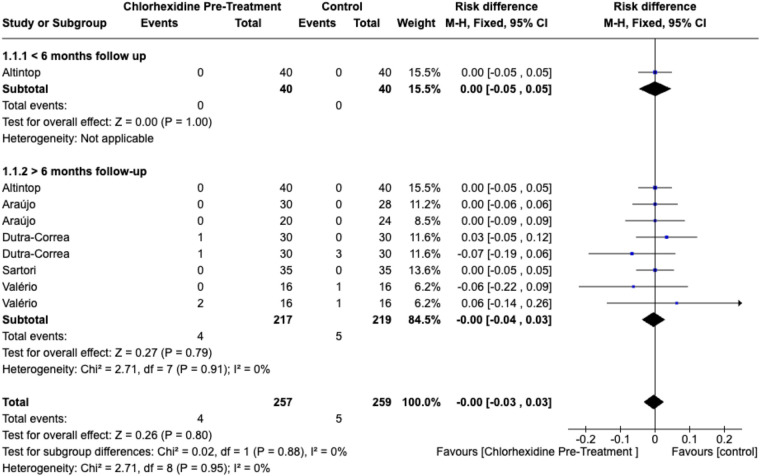 Figure 6
Figure 6| Search | Terms |
|---|---|
| # 1 (Chlorhexidine) | "Chlorhexidine” OR “chlorhexidine digluconate” OR CHX OR digluconate chlorhexidine* |
| #2 (Adhesive restorations) | "Dentin bonding” OR “resin–dentin bond” OR “bond strength” OR “dental bonding” OR “resin restoration” OR “adhesive restoration” OR “composite restoration” |
| #3 (Clinical outcomes) | "Clinical performance” OR “restoration retention” OR “restorative survival” OR “marginal adaptation” OR “marginal integrity” OR “secondary caries” OR “postoperative sensitivity" |
| # 4 | #1 AND #2 AND #3 |
| Author and year | Type of clinical trial | Clinical trial registration | Number (age) of restorations | Type of teeth (temporary/permanent) | Class of cavity | Restoration procedures (Adhesive and resin composite used) | Chlorhexidine application parameters | Evaluation criteria | Follow-up | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Sobral et al., 2005 ( | RCT, split mouth | Not reported | 51 restorations, 17 patients (20–48 y) | Permanent premolars | Class II | Control ( | Cav-Clean (CHX): applied to cavity walls with cotton roll for 1 min; excess removed with dry cotton pellets | Patient-reported postoperative sensitivity (cold, heat, sweet, floss), 4-point scale | Day 1, Day 4, Day 7 | Gluma desensitizer and CHX showed no significant benefit in reducing postoperative sensitivity compared with adhesive alone. |
| Hajizadeh et al., 2013 ( | RCT, crossover, double-blind | IRCT201104236267N1 | 60 restorations, 30 patients (20–35 y) | Permanent premolars | OM Class II | Control ( | 2% CHX solution applied to etched dentin for 60 s; air-dried; applied as separate cavity disinfectant | Patient-reported postoperative sensitivity (VAS 11-point), categorized | Baseline, Day 1, 1 week, 1 month, 6 months* | CHX significantly reduced immediate postoperative sensitivity at 1 day, with no differences at later follow-ups. |
| Dutra-Correa et al., 2013 ( | RCT | Not reported | 120 restorations, 37 patients (27–79 y) | Permanent premolars, molars | Class V | Group 1 – XP Bond (XPB, | 2% CHX aqueous solution applied to dentin surface after etching (for XPB) or prior to self-etch adhesive (XEN) for 60 s; air-dried; applied separately | Modified UNC-USPHS: retention, color match, marginal staining, wear, adaptation, texture, pre-/post-op sensitivity | Baseline, 1 week, 6 month*, 18 month§ | CHX pretreatment did not affect 6- or 18-month clinical performance or retention of either adhesive system. |
| Sartori et al., 2013 ( | RCT, crossover | Not reported | 70 restorations, 20 patients (33–64 y) | Permanent incisors, canines, premolars, molars | Class V | Control Group – Adper Single Bond 2 (SB, | 2% CHX digluconate applied to dentin after etching under scrubbing action for 30 s; excess removed with cotton pellets | Modified USPHS: retention, marginal discoloration/integrity, post-op sensitivity, caries, pulp vitality | Baseline, 6 months*, 12 months, and 36 months§ | CHX pretreatment did not improve long-term clinical performance or durability of Class V adhesive restorations. |
| Araújo MS. Et al., 2015 ( | Double-blind, RCT | Local Ethics Committee (protocol 95/10) | 88 restorations, 22 patients (45 ± 8 y) | Permanent anterior and posterior teeth | Class V | Control groups: CSE (Clearfil SE Bond) or ADS (AdheSE) applied per manufacturer instructions; composite: Filtek Z-250 in 2–3 increments of 2 mm, light-cured 20 s each, | 50 μL of 20% CHX digluconate added to 950 μL primer to yield 1.0 wt% CHX; applied as primer before adhesive | Modified USPHS: retention, marginal staining/adaptation, post-op sensitivity, caries recurrence | Baseline and 24 months§ | Incorporation of CHX did not improve 2-year clinical performance; Clearfil SE Bond showed higher retention than AdheSE regardless of chlorhexidine. |
| Montagner et al., 2015 ( | Prospective RCT, split-mouth, triple-blind | 169 restorations, 42 patients (21–76 y) | Permanent incisors, canines, premolars | Class V | Group1: 35% phosphoric acid etching (dentin 20 s, enamel 15 s) + Adper Single Bond 2 adhesive, followed by Filtek Z350 nanocomposite resin in ≥2 increments (≤2 mm thick), each light-cured 20 s at 800 mW/cm2. | 2% CHX applied 60 s post-etch, excess removed | FDI: retention, marginal adaptation/staining, surface staining, post-op sensitivity, aesthetics, fracture, anatomy, vitality | 6 months* | CHX application did not affect 6-month retention of Class V restorations; cavity geometry, not CHX, influenced failure. | |
| Galafassi et al., 2017 ( | Prospective RCT, split mouth | FORP/USP—Case No 02937212.5.0000.5419 | 80 restorations, 20 children (8–12 y) | Permanent molars | Class I (occlusal) | Group1: 37% phosphoric acid (enamel 30 s, dentin 15 s) + Adper Single Bond 2, light-cured 10 s. Restoration: Filtek Z350 XT incremental composite). | 2% CHX applied to dentin for 60 s after acid etching; excess removed. s. | Modified USPHS criteria (retention, marginal adaptation, marginal discoloration, other failures); | Baseline, 6 months*, 12 months§ | Laser-prepared cavities showed superior clinical performance regardless of re-wetting agent; CHX did not significantly influence outcomes. |
| Favetti et al., 2017 ( | RCT, crossover | 105 restorations, 42 patients (49.7 y) | Permanent incisors, canines, premolars | Class V | Group1: Two-step etch-and-rinse adhesive (Single Bond 2, 3M ESPE) applied after 35% phosphoric acid etching (enamel 20 s, dentin 15 s), light-cured 10 s; restored with Filtek Z350 nanocomposite resin in 2 increments ≤2 mm thick, light-cured 20 s per increment. | 2% CHX applied to etched dentin for 60 s with scrubbing, excess removed | FDI: retention, marginal adaptation/staining, post-op sensitivity, surface properties, fracture, anatomy, vitality | Baseline (1 wk), 6 months*, 12 months, 24 months, and 36 months§ | CHX pretreatment did not improve long-term retention or survival of NCCL restorations over 36 months. | |
| Valério RA et al. 2020 ( | RCT, split-mouth | ReBEC RBR-8n5n3v | 64 restorations, 16 patients (8–12 y) | Permanent first molars | Class I | Control ( | 2% CHX applied after caries removal, before adhesive; excess removed | Modified USPHS: retention, marginal adaptation/discoloration, secondary caries, pulp vitality | Baseline, 6 months*, 12 months, 48 months§ | Er:YAG laser or bur preparation produced similar 4-year restoration survival; CHX biomodification did not influence outcomes. |
| Nemt-Allah AA 2022 ( | RCT | 57 restorations, 19 patients (17–50 y) | Permanent posterior teeth | Class II | Control ( | 2% CHX: Consepsis applied 1 min, excess removed; separate step | FDI criteria for marginal adaptation, marginal staining, and postoperative sensitivity | Immediate, 6 months*, 12 months*, and 24 months§ | No significant differences were observed among groups; CHX did not affect marginal adaptation, staining, or postoperative sensitivity for up to 2 years. | |
| Altıntop H., et al. 2025 ( | Prospective, single-blind, RCT | 80 restorations, 40 patients (5–9 y) | Primary molars | Class II | Control ( | CHX incorporated within Peak Universal Bond (0.2%), no separate application step | FDI: esthetic, functional, biological properties, post-op sensitivity, secondary caries, retention, marginal adaptation | 3 months, 6 months*, 9 months, and 12 months§ | CHX-containing adhesive showed similar 12-month clinical success to standard adhesive and higher microtensile bond strength, without compromising performance. |
| Clinical outcome | No. of studies (restorations) | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Overall certainty of evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|
| Restoration retention (≥6 months) | 9 (∼833) | RCTs | Not serious | Not serious | Not serious | Serious | Not serious | ⊕⊕⊕⊝ Moderate |
| Postoperative sensitivity | 10 (∼880) | RCTs | Not serious | Not serious | Not serious | Serious | Not serious | ⊕⊕⊕⊝ Moderate |
| Secondary caries incidence | 4 (∼302) | RCTs | Not serious | Not serious | Not serious | Very serious | Not serious | ⊕⊕⊝⊝ Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental materials and restorations · Dental Erosion and Treatment · Endodontics and Root Canal Treatments
Introduction
1
The long-term clinical success of adhesive restorations depends on the stability of the resin–dentin interface. Composite resins provide esthetic and conservative treatment options, but their durability is limited by hydrolytic and enzymatic degradation of the hybrid layer (HL), resulting in loss of retention, marginal discoloration, secondary caries, and postoperative sensitivity (1–3).
In recent years, research has increasingly focused on strategies to enhance the long-term durability of the bond between dental adhesive systems and dentin, as the HL gradually deteriorates due to collagen fiber hydrolysis, even in the absence of bacterial challenge (3, 4).
Matrix metalloproteinases (MMPs) and cysteine cathepsins within dentin are activated during acid etching or by acidic monomers in self-etch adhesives, leading to collagen breakdown within the HL (4, 5). Inhibiting these endogenous enzymes has been proposed as a strategy to enhance long-term bond stability (6).
Chlorhexidine digluconate (CHX) is a well-established cationic bisbiguanide with strong antimicrobial and protease-inhibiting properties (7–10). Due to its substantivity and affinity for dentin phosphate groups, CHX can suppress MMP-mediated collagen degradation and help preserve HL integrity. In vitro studies have shown that low CHX concentrations (0.1%–2%) effectively inhibit MMP activity and maintain resin–dentin bond strength for extended aging periods (11, 12).
In 2010, Breschi et al. (5) reported that the application of 0.2% CHX suppressed MMP activity in demineralized dentin aged for two years and extended the durability of adhesive bonds. Similarly, Loguercio et al. (10) found that CHX treatment maintained higher bond strengths after five years of aging, representing the longest follow-up period reported in the literature regarding CHX-mediated MMP inhibition. More recently, Breschi et al. confirmed that CHX retained anti-proteolytic activity within the hybrid layer even after 10 years of accelerated aging, further supporting its role in hybrid layer protection (11).
Nevertheless, the clinical effectiveness of CHX in preserving restoration longevity remains inconclusive. It was reported that CHX pretreatment did not improve the retention and marginal integrity of dental restorations (13).
Such discrepancies may result from variations in CHX concentration, application time, adhesive system, or follow-up duration. Therefore, this systematic review and meta-analysis aimed to synthesize the available clinical evidence regarding the influence of CHX pretreatment on the longevity and performance of resin-based restorations. The null hypothesis was that CHX pretreatment, regardless of concentration or application protocol, does not significantly affect the clinical outcomes of resin–dentin restorations.
Materials and methods
2
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (14) and was prospectively registered in the International Prospective Register of Systematic Reviews [PROSPERO; registration number (CRD420251165239)]. Studies were selected based on the population, intervention, comparison, outcome, and study design (PICOS) framework: population (patients receiving adhesive restorations in vital teeth); intervention (dentin pretreatment with CHX applied either as a solution or incorporated into the adhesive protocol); comparison (no CHX pretreatment or conventional adhesive procedure); outcome (clinical performance measures, including restoration retention, marginal adaptation, marginal discoloration, postoperative sensitivity, and secondary caries); and study design [randomized controlled trials (RCTs) or controlled clinical trials]. Only English full-text publications were included, while duplicates and studies without accessible full text were excluded.
Comprehensive electronic searches were conducted in PubMed, Scopus, Web of Science, and the Cochrane Library from database inception to September 2025. Structured search strategies were tailored for each database using combinations of keywords and Medical Subject Headings (MeSH) related to “chlorhexidine,” “dentin,” “adhesion,” “bond strength,” “resin composite,” and “clinical trial” (Table 1). Reference lists of eligible studies and relevant reviews were also screened to identify additional publications. All retrieved records were imported into a reference manager software program (EndNote 20; Clarivate Analytics) for duplicate removal. Two reviewers independently screened titles and abstracts, followed by full-text assessments; disagreements were resolved through discussion or by consulting a third reviewer.
Studies were included if they met the following criteria: (1) randomized controlled trials or controlled clinical trials; (2) human clinical studies involving vital teeth restored with adhesive restorations; (3) use of chlorhexidine as a dentin pretreatment, either as a solution or incorporated into the adhesive protocol; (4) presence of a control group without chlorhexidine pretreatment; (5) reporting at least one clinical outcome of interest, including restoration retention, marginal adaptation, marginal discoloration, postoperative sensitivity, or secondary caries; (6) a minimum follow-up period of one week; and (7) availability of full-text articles published in English. Studies were excluded if they were: (1) in vitro, in situ, animal, or laboratory-based studies; (2) observational studies, case reports, case series, reviews, or conference abstracts; (3) studies evaluating non-adhesive restorations or non-vital teeth; (4) studies lacking a comparator group; or (5) publications with inaccessible full texts or insufficient clinical outcome data.
Data were independently extracted by two reviewers (MAF-B and EP) for each study, including author, year, country, study design, CHX type and concentration, adhesive system, restoration procedure, control protocol, follow-up period, clinical evaluation criteria, and reported outcomes. Any discrepancies were resolved by consensus. The methodological quality of RCTs was appraised using the Cochrane Risk-of-Bias 2.0 tool, whereas controlled clinical trials were evaluated using the Joanna Briggs Institute (JBI) checklist for quasi-experimental studies (15). Conflicts were resolved through consensus with a third reviewer (TR and NK). The certainty of evidence for each clinical outcome was evaluated using the GRADE approach (16), considering factors such as study risk of bias, consistency of effect, im-precision, indirectness, and publication bias. Certainty ratings were classified as high, moderate, low, or very low, and detailed justifications for downgrading were reported.
When two or more studies reported comparable outcomes, quantitative synthesis was performed using a software program (Review Manager 5.4.1; The Cochrane Collaboration, Copenhagen, Denmark). Effect sizes were expressed as risk ratios (RRs) with 95% confidence intervals (CIs) for dichotomous variables. To account for the time-dependent nature of clinical outcomes and to explore whether the effect of CHX pretreatment varies with observation length, separate meta-analyses were planned according to follow-up duration. Studies were categorized into short-term (<6 months) and long-term (≥6 months) follow-up periods. For studies reporting multiple follow-up assessments, data from the longest available time point within each category were extracted. When a study contributed data to both short- and long-term analyses (e.g., reporting outcomes at 3 and 12 months), the corresponding time points were included separately in each respective pooled analysis. All analyses were conducted using a random-effects model, and heterogeneity was quantified using the I^2^ statistic. A fixed-effect model was used when heterogeneity was low (I^2^ < 50%); otherwise, a random-effects model was applied.
Although the included studies varied in terms of CHX concentration, application time, adhesive system, and cavity class, meta-analytic pooling was considered appropriate for the following reasons: (1) all studies addressed the same PICOS question and shared a common intervention–comparator framework; (2) the outcome measures (retention, postoperative sensitivity, secondary caries) were defined using standardized and comparable clinical criteria; and (3) preliminary assessment of statistical heterogeneity using the I^2^ statistic revealed no significant heterogeneity (I^2^ = 0%) for any of the pooled outcomes, supporting the combinability of effect estimates. These considerations align with current methodological guidance, which permits pooling in the presence of clinical diversity when statistical heterogeneity is low and the body of evidence is coherent.
Results
3
The electronic search retrieved 900 records from the different databases. After removal of 100 duplicates, 800 titles and abstracts were screened for eligibility. Of these, 789 records were excluded based on the predefined inclusion and exclusion criteria. Following full-text assessment, 11 randomized or controlled clinical trials fulfilled the eligibility criteria and were included in the qualitative synthesis and quantitative analysis (meta-analysis). The study selection process is summarized in the PRISMA flow diagram (Figure 1).
PRISMA flow diagram of study selection.
The clinical trials, published between 2005 and 2025, were conducted across diverse populations and settings. Sample sizes ranged from 14 to 60 participants, covering age groups from young children to older adults. Both primary and permanent teeth were included, with cavity classes ranging from non-carious cervical lesions (NCCLs) and Class V restorations to Class I and II carious lesions. CHX was most tested at concentrations of 0.2% and 2%, with application times of 15–30 s in most protocols. Adhesive systems included etch-and-rinse, self-etch, and universal adhesives. Resin composites were the predominant restorative material, placed using either incremental or bulk-fill techniques. Control groups generally followed adhesive protocols without CHX pretreatment. Follow-up durations ranged from 1 week to 4 years. Outcomes were assessed according to standardized clinical criteria, such as the modified United States Public Health Service (USPHS) and Fédération Dentaire Internationale (FDI) evaluation systems, and in some studies supplemented by radiographic examinations, pulp vitality testing, or patient-reported sensitivity assessments. Follow-up durations ranged from 1 week to 4 years, with most studies reporting outcomes at ≥6 months. For meta-analysis, outcomes were grouped into short-term (<6 months) and long-term (≥6 months) follow-up where applicable. The study by Altıntop et al. (25), while reporting up to 12-month data, contributed to the short-term analysis based on its 3-month evaluations. All studies reported at least one of the prespecified clinical outcomes, including restoration retention, postoperative sensitivity, or secondary caries. A summary of the study characteristics is presented in Table 2.
The risk of bias assessment indicated that most studies presented low to moderate risk across the five domains of the Cochrane RoB 2.0 tool. Some studies had unclear allocation concealment, incomplete outcome data, or potential deviations from intended interventions; however, overall confidence in the results was considered acceptable (Figures 2, 3).
Risk of bias graph: review of authors’ judgments about each risk of bias item presented as percentages across all included studies. Domains: D1: Bias arising from the randomization process; D2: Bias due to deviations from intended interventions; D3: Bias due to missing outcome data; D4: Bias in measurement of the outcome; D5: Bias in selection of the reported result.
Risk of bias summary: review of authors’ judgments about each risk of bias item for each included study. Symbols: “+” Low risk; “-” Some concerns; “X” High risk.”.
The certainty of evidence for the clinical outcomes associated with dentin pretreatment with chlorhexidine (CHX) was evaluated using the GRADE approach. Evidence derived from 11 randomized and controlled clinical trials provides moderate-certainty evidence that CHX pretreatment does not improve the clinical performance of adhesive restorations compared with conventional adhesive protocols without CHX, with respect to restoration retention, postoperative sensitivity, and secondary caries incidence (Table 3). Downgrading of the evidence was primarily driven by imprecision, related to modest sample sizes and the limited number of clinical events, as well as some concerns regarding risk of bias in individual studies, including incomplete reporting of allocation concealment, blinding, or outcome data. Across outcomes, the direction and magnitude of effects were consistent, and statistical heterogeneity was negligible, indicating no serious concerns regarding inconsistency. Indirectness was not considered serious, as the populations, interventions, comparators, and outcomes were directly relevant to contemporary clinical adhesive dentistry. For secondary caries incidence, the certainty of evidence was rated as low, owing to very few reported events and relatively short follow-up periods, resulting in substantial uncertainty around the effect estimates. Overall, the available evidence indicates that CHX dentin pretreatment results in short- to medium-term clinical performance comparable to standard adhesive procedures, without conferring a measurable advantage in restoration longevity or biological outcomes.
For restoration retention, pooled analysis showed no statistically significant difference between CHX-treated and control groups at either short-term (< 6 months) or long-term (>6 months) follow-up (p > .05). The combined estimate indicated comparable retention rates (risk difference = 0.01; 95% CI, −0.02 to 0.04; p = .53) with no heterogeneity (I^2^ = 0%) (Figure 4).
Forest plot of restoration retention comparing CHX pretreatment vs. control groups. Data for ≥6 months follow-up represent the longest available follow-up for each study. Comparator groups are placebo (water) controls where available; otherwise, standard adhesive-only controls were used.
Similarly, no significant difference was found in postoperative sensitivity (RD = 0.01; 95% CI, −0.04 to 0.06; p = .67; I^2^ = 0%) (Figure 5) or in secondary caries incidence (RD = 0.00; 95% CI, −0.03 to 0.03; p = .80; I^2^ = 0%) (Figure 6).
Forest plot of postoperative sensitivity comparing CHX pretreatment vs. control groups. Data for ≥6 months follow-up represent the longest available follow-up for each study. Comparator groups are placebo (water) controls where available; otherwise, standard adhesive-only controls were used.
Forest plot of secondary caries comparing CHX pretreatment vs. control groups. Data for ≥6 months follow-up represent the longest available follow-up for each study. Comparator groups are placebo (water) controls where available; otherwise, standard adhesive-only controls were used.
Discussion
4
This systematic review and meta-analysis critically examined the clinical effects of CHX pretreatment on adhesive restorations, focusing on restoration retention, postoperative sensitivity, and secondary caries. Across 11 randomized clinical trials, CHX application, whether used as a cavity disinfectant or after acid etching, did not significantly affect clinical performance compared with conventional adhesive protocols. These findings support the null hypothesis and indicate that CHX pretreatment offers no additional long-term clinical advantage in routine adhesive dentistry.
Mechanistically, CHX exhibits high affinity for demineralized dentin due to its cationic nature and capacity to bind phosphate groups, resulting in durable substantivity and inhibition of MMPs responsible for hybrid layer degradation (26). Although laboratory studies demonstrate sustained bond strength preservation through MMP inhibition (27–29), the clinical evidence remains inconsistent. This discrepancy may be partly explained by the fact that the beneficial effect of CHX is markedly diminished when applied to mineralized dentin prior to etching, due to its limited penetration and binding capacity. This may explain the poor translation of in vitro benefits into clinical performance, as highlighted by Frassetto et al. (30).
Clinically, most included trials used etch-and-rinse adhesives (e.g., AdheSE, XP Bond, Single Bond Universal, Bond, Peak Universal Bond), which establish durable hybrid layers and chemically interact with hydroxyapatite through functional monomers such as 10-methacryloxydecyl dihydrogen phosphate (10-MDP) (31, 32). The inherent chemical stability and micromechanical retention of these systems likely overshadow any incremental benefit from CHX-mediated MMP inhibition, consistent with the stable retention outcomes observed across follow-ups of up to four years (22, 24).
It should be noted that one included study evaluated primary teeth (25), while the others focused on permanent dentition. Although the dentin structure and mineralization differ, the consistent findings (with no statistical heterogeneity) across both populations in our analysis suggest that, within the observed follow-up periods, the clinical effect of CHX pretreatment may not be significantly influenced by dentition type. However, this observation is based on a single pediatric study and warrants confirmation in future research.
The reviewed studies varied in CHX concentration and application protocols, typically using 0.2% to 2% for 15–60 s after etching (13, 18, 20, 25). Shorter application times or lower concentrations may limit CHX diffusion into demineralized dentin, reducing its inhibitory potential. Additionally, universal adhesives contain hydrophilic solvents and acidic monomers that could partially remove or dilute CHX residues, altering its interaction with collagen fibrils (25). Despite these variations, meta-analytic results revealed no significant heterogeneity (I^2^ = 0%), reinforcing the robustness and reproducibility of the overall clinical trend.
Several clinical and material-related factors may further explain the limited effect of CHX in vivo. Continuous mechanical stresses from occlusal loading, polymerization shrinkage, and thermal and pH fluctuations induce fatigue and degradation of the resin–dentin interface, diminishing the influence of enzymatic inhibition over time (31). Differences in cavity configuration, restoration type, oral environment, and patient-specific factors such as hygiene and dietary habits also contribute to interstudy variability. These complex clinical dynamics, absent in controlled laboratory conditions, likely explain the discrepancy between the biochemical efficacy of CHX and its limited clinical impact.
It is worth noting that other enzymatic inhibitors, such as benzalkonium chloride (BAC), quaternary ammonium methacrylates (QAMs), or natural extracts (e.g., proanthocyanidins), have also been investigated for their potential to stabilize the resin–dentin interface (33–35). These agents may offer different mechanisms of action or substantivity profiles compared to CHX. Future clinical research could benefit from direct comparisons between CHX and these alternative inhibitors to identify the most effective strategy for enhancing bond durability in specific clinical scenarios.
The methodological quality of the included studies was generally acceptable, with most trials demonstrating low to moderate risk of bias. While allocation concealment and examiner blinding were adequately reported, some studies lacked detailed descriptions of randomization or dropout management. Variations in restoration class, adhesive type, and evaluation criteria could also introduce subtle clinical heterogeneity not fully captured by statistical models. Standardized protocols and long-term randomized clinical trials are needed to determine whether CHX pretreatment may offer measurable benefits with self-etch or universal adhesives, which are more prone to hydrolytic and enzymatic degradation. In addition, Embase and gray literature were not systematically searched due to access limitations and the review's focus on peer-reviewed clinical trials; however, manual reference screening was performed to minimize the risk of missing relevant studies. Despite these limitations, CHX application remains a safe adjunctive procedure that does not compromise bonding effectiveness. The consistency of clinical outcomes across adhesive systems and CHX concentrations indicates that current adhesives provide reliable long-term performance, even in the absence of MMP inhibition strategies. Therefore, based on current evidence, CHX pretreatment should not be considered a mandatory step in routine adhesive protocols. However, clinicians may still consider it for its antimicrobial and disinfectant properties, especially in patients with high caries risk or in cases requiring additional dentin decontamination for selective preventive purposes.
Conclusions
5
Based on the available clinical evidence dentin pretreatment with CHX did not show a significant effect on the clinical performance of resin-based restorations in terms of retention, postoperative sensitivity, or secondary caries. While CHX is an effective MMP inhibitor in vitro, this benefit was not translated into a measurable clinical advantage in the reviewed trials. Broad conclusions regarding CHX's clinical inefficacy should be avoided due to the constrained evidence base. Further long-term, standardized RCTs are warranted to clarify its potential role, particularly with modern adhesive systems.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Carvalho RM Manso AP Geraldeli S Tay FR Pashley DH. Durability of bonds and clinical success of adhesive restorations. Dent Mater. (2012) 28:72–86. 10.1016/j.dental.2011.09.01122192252 PMC 3863938 · doi ↗ · pubmed ↗
- 2Hashimoto M Ohno H Kaga M Endo K Sano H Oguchi H. In vivo degradation of resin–dentin bonds in humans over 1 to 3 years. J Dent Res. (2000) 79:1385–91. 10.1177/0022034500079006060110890717 · doi ↗ · pubmed ↗
- 3Pashley DH Tay FR Yiu C Hashimoto M Breschi L Carvalho RM Collagen degradation by host-derived enzymes during aging. J Dent Res. (2004) 83:216–21. 10.1177/15440591040830030614981122 · doi ↗ · pubmed ↗
- 4Mazzoni A Pashley DH Nishitani Y Breschi L Mannello F Tjäderhane L Reactivation of inactivated endogenous proteolytic activities in phosphoric acid–etched dentine by etch-and-rinse adhesives. Biomaterials. (2006) 27:4470–6. 10.1016/j.biomaterials.2006.01.04016687171 · doi ↗ · pubmed ↗
- 5Breschi L Mazzoni A Nato F Carrilho M Visintini E Tjäderhane L Chlorhexidine stabilizes the adhesive interface: a 2-year in vitro study. Dent Mater. (2010) 26:320–5. 10.1016/j.dental.2009.11.15320045177 PMC 3819099 · doi ↗ · pubmed ↗
- 6Carrilho MR Geraldeli S Tay FR de Goes MF Carvalho RM Tjäderhane L In vivo preservation of the hybrid layer by chlorhexidine. J Dent Res. (2007) 86:529–33. 10.1177/15440591070860060817525352 · doi ↗ · pubmed ↗
- 7Zhou W Liu S Zhou X Hannig M Rupf S Feng J Modifying adhesive materials to improve the longevity of resinous restorations. Int J Mol Sci. (2019) 20:723. 10.3390/ijms 2003072330744026 PMC 6387348 · doi ↗ · pubmed ↗
- 8Carrilho MR Carvalho RM de Goes MF Di Hipólito V Geraldeli S Tay FR Chlorhexidine preserves dentin bond in vitro. J Dent Res. (2007) 86:90–4. 10.1177/15440591070860011517189470 PMC 2248723 · doi ↗ · pubmed ↗