Effect of co-occurring mutations in TP53 gene and TERT promoter on the survival of bladder cancer patients
Maria Lina Tornesello, Maria Carmela Piccirillo, Rosa Tambaro, Vittorio Simeon

TL;DR
Bladder cancer patients with mutations in both TP53 and TERT promoter have significantly worse survival, suggesting these mutations act together to worsen outcomes.
Contribution
This study identifies a strong prognostic link between co-occurring TP53 and TERTp mutations in bladder cancer patients.
Findings
Patients with both TP53 and TERTp mutations had the worst overall survival compared to other mutation groups.
Co-occurring TP53 and TERTp mutations were associated with higher tumor mutational burden and microsatellite instability.
The association was validated in an independent cohort, supporting the biological relevance of these mutations.
Abstract
Mutations in the TP53 gene and telomerase reverse transcriptase promoter (TERTp) are among the most frequent genetic alterations in bladder cancer, but the clinical impact of their co-occurrence has not been fully explored. In this study, we assessed the mutational landscape as well as the prognostic significance of concurrent TERTp and TP53 mutations in a cohort of bladder urothelial carcinoma patients. Using data from the cBioPortal database, we retrospectively analysed primary bladder urothelial carcinoma cases profiled with the Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) assays. We investigated the relationships between tumour mutational burden (TMB), microsatellite instability (MSI), and somatic mutations. The Kaplan-Meier method was used to calculate patient overall survival. Log-rank testing and multivariable Cox proportional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
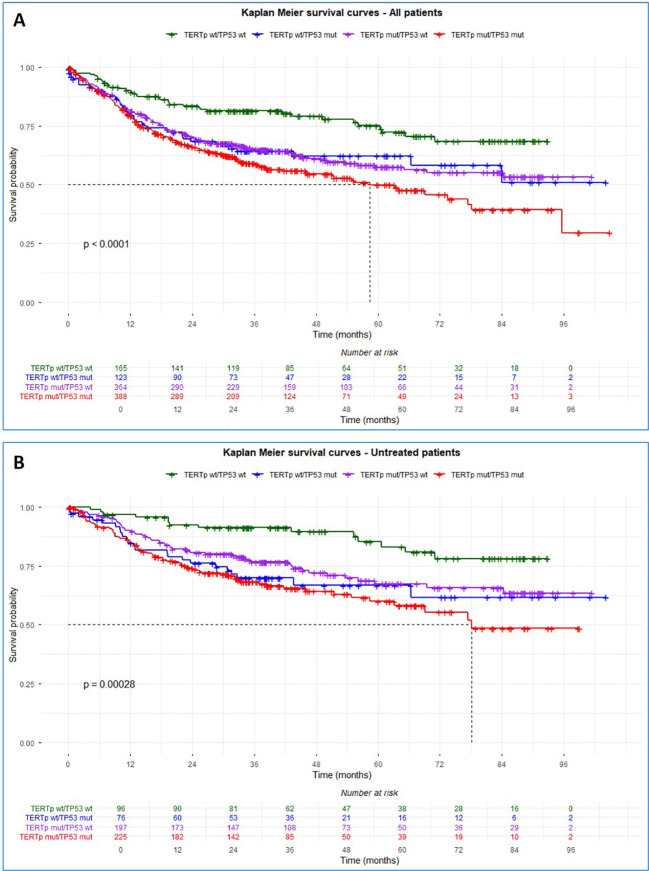 Figure 1
Figure 1| Variables | Total (N = 1,111) |
|---|---|
| Age | |
| Median (IQR) | 66 (58 - 73) |
| Missing | 106 (9.5%) |
| Sex (%) | |
| Female | 261 (23%) |
| Male | 849 (76%) |
| Missing | 1 (0.1%) |
| Smoking (%) | |
| Never | 363 (33%) |
| Active, former | 654 (59%) |
| Missing | 94 (8%) |
| Tumour grade (%) | |
| G1-2 | 247 (22%) |
| G3 | 796 (72%) |
| Missing | 68 (6.1%) |
| Intravesical treatment | |
| Naive | 748 (67%) |
| Treated | 266 (24%) |
| Missing | 97 (8.7%) |
| Systemic treatment | |
| Naive | 828 (75%) |
| Treated | 172 (15%) |
| Missing | 111 (10%) |
| MSI status (%) | |
| Instable H | 9 (1%) |
| Instable L | 16 (1%) |
| Stable | 1082 (97%) |
| Missing | 4 (0.4%) |
| MSI score | |
| Median (IQR) | 0.2 (0 - 0.66) |
| Missing | 4 (0.4%) |
| TMB (mutations/Mb) | |
| Median (IQR) | 9.5 (5.9 - 17) |
| N. Mutations per sample | |
| Median (IQR) | 11 (7.0 - 18) |
| Missing | 24 (3%) |
| Gene name | Gene type | p-value | q-value | ||
|---|---|---|---|---|---|
|
| Oncosuppressor | 58 (33%) | 52 (12%) | <0.001 |
|
|
| Oncosuppressor | 12 (6.8%) | 158 (36%) | <0.001 |
|
|
| Oncogene | 22 (13%) | 107 (24%) | 0.001 |
|
|
| Oncosuppressor | 41 (23%) | 151 (34%) | 0.008 |
|
|
| Oncogene | 13 (7.4%) | 65 (15%) | 0.013 |
|
|
| Oncogene | 22 (13%) | 88 (20%) | 0.029 | 0.076 |
|
| Oncogene | 28 (16%) | 46 (10%) | 0.059 | 0.14 |
|
| Oncosuppressor | 12 (6.8%) | 50 (11%) | 0.092 | 0.2 |
|
| Oncogene | 15 (8.5%) | 58 (13%) | 0.11 | 0.2 |
|
| Oncosuppressor | 30 (17%) | 58 (13%) | 0.2 | 0.4 |
|
| Oncogene | 18 (10%) | 61 (14%) | 0.2 | 0.4 |
|
| Oncosuppressor | 12 (6.8%) | 43 (9.8%) | 0.2 | 0.4 |
|
| Oncogene | 21 (12%) | 66 (15%) | 0.3 | 0.5 |
|
| Oncosuppressor | 60 (34%) | 134 (30%) | 0.4 | 0.5 |
|
| Oncosuppressor | 21 (12%) | 59 (13%) | 0.6 | 0.8 |
|
| Oncogene | 46 (26%) | 119 (27%) | 0.8 | 0.9 |
|
| Oncosuppressor | 17 (9.7%) | 46 (10%) | 0.8 | 0.9 |
|
| Oncosuppressor | 29 (16%) | 69 (16%) | 0.8 | 0.9 |
|
| Oncosuppressor | 22 (13%) | 54 (12%) | >0.9 | >0.9 |
| Characteristic | N | wt/wt, | TERTp wt/ | p-value2 | ||
|---|---|---|---|---|---|---|
| Median age, y | 1,004 | 65 (18–87) | 66 (30–91) | 66 (31–92) | 67 (34–89) | 0.3 |
| Sex | 1,110 | 0.8 | ||||
| Female | 44 (25%) | 90 (23%) | 34 (26%) | 93 (22%) | ||
| Male | 131 (75%) | 297 (77%) | 98 (74%) | 323 (78%) | ||
| Smoking history | 1,017 | 0.5 | ||||
| Never | 66 (41%) | 124 (34%) | 44 (35%) | 129 (35%) | ||
| Former/active | 96 (59%) | 236 (66%) | 82 (65%) | 240 (65%) | ||
| Tumour grade | 1,043 |
| ||||
| G1-2 | 74 (46%) | 120 (32%) | 24 (18%) | 29 (8%) | ||
| G3 | 87 (54%) | 253 (68%) | 107 (82%) | 349 (92%) | ||
| MSI type | 1,105 |
| ||||
| Instable H | 5 (2.9%) | 1 (0.3%) | 2 (1.5%) | 12 (0.2%) | ||
| Instable L | 1 (0.6%) | 6 (1.6%) | 3 (2.3%) | 6 (1.4%) | ||
| Stable | 168 (97%) | 378 (98%) | 127 (96%) | 409 (98%) | ||
| MSI score | 1,107 | 0.09 (0, 0.40) | 0.17 (0, 0.56) | 0.26 (0, 0.93) | 0.27 (0.05, 0.83) |
|
| TMB (n. mut/Mb) | 1,087 | 8 (4, 14) | 10 (6, 16) | 8 (5, 13) | 13 (9, 21) |
|
| Variables | All patients | Untreated patients | Treated patients** | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | P value* | HR | 95%CI | P value* | HR | 95%CI | P value* | ||
| Age | 1.02 | 1.01 - 1.03 |
| 1.04 | 1.02 - 1.05 |
| 0.98 | 0.97 - 1.00 | 0.11 | |
| Sex male | 1.05 | 0.83 - 1.34 | 0.7 | 1.05 | 0.74 - 1.50 | 0.8 | 0.88 | 0.52 - 1.49 | 0.6 | |
| Smoking*** | 1.60 | 1.26- 2.01 |
| 1.69 | 1.20- 2.38 |
| 1.36 | 0.86 – 2.14 | 0.2 | |
| Grade G3 | 3.55 | 2.56-4.93 |
| 3.41 | 2.15 – 5.41 |
| 1.64 | 0.72 – 3.75 | 0.2 | |
| MSI score | 0.96 | 0.90- 1.02 | 0.2 | 0.95 | 0.86 - 1.06 | 0.4 | 0.94 | 0.85 - 1.04 | 0.2 | |
| TMB | 0.99 | 0.99 - 1.00 | 0.1 | 1.00 | 0.99 - 1.01 | 0.7 | 0.99 | 0.97 - 1.00 | 0.12 | |
| 1.83 | 1.27 - 2.62 |
| 2.17 | 1.20 – 3.90 |
| 0.86 | 0.40 - 1.85 | 0.7 | ||
| TERTpwt/ | 1.84 | 1.19 – 2.85 |
| 2.69 | 1.38 – 5.23 |
| 0.97 | 0.41 - 2.32 | >0.9 | |
| 2.32 | 1.63 – 3.31 |
| 3.21 | 1.81 – 5.70 |
| 0.77 | 0.35 – 1.66 | 0.5 | ||
| Variables | Multivariate - Untreated patients | ||
|---|---|---|---|
| HR | 95%CI | P value*** | |
| Age | 1.03 | 1.02- 1.05 |
|
| Smoking* | 1.56 | 1.10 - 2.21 |
|
| Tumour grade G3 | 2.97 | 1.83 -4.82 |
|
| 1.88 | 1.05 -3.40 |
| |
| 1.95 | 1.0 – 3.83 | 0.051 | |
| 2.06 | 1.15 – 3.70 |
| |
- —Ministero della Salute10.13039/501100003196
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Telomeres, Telomerase, and Senescence · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
Bladder cancer is one of the most common malignancies in the world, with approximately 613,791 cases and 220,349 deaths in 2022 (1). Several risk factors are involved in the development of bladder cancer, such as cigarette smoking, exposure to occupational and environmental contaminants, and advanced age (2, 3). Its incidence is about four times higher in men than in women, a disparity largely attributed to higher rates of smoking habit and occupational exposures among men, in addition to other biological and epidemiological factors (3–6).
Most bladder cancers are urothelial carcinomas, representing about 90% of cases in Western countries, with approximately 75% classified as non-muscle-invasive (NMIBC) and 25% as muscle-invasive (MIBC) or metastatic disease (7–9). The NMIBC are commonly low grade with favourable prognosis but with frequent recurrences, whereas MIBC are almost always high grade, aggressive, and often lethal (10, 11). A subset of NMIBC progresses to MIBC, underscoring the need for improved prediction of high-risk patients (12–16). A main characteristic of bladder urothelial cancer is the high frequency of multifocal synchronous and metachronous tumours (17). These lesions often share early trunk mutations and genomic aberrations, but also harbour distinct private alterations, reflecting both clonal relatedness and tumour heterogeneity (18–20).
Urothelial bladder cancer is among the most highly mutated cancers, with an average tumour mutation burden (TMB) of 7.7 per megabase and above 300 exonic mutations per tumour (21–23). The prevalent cancer driver mutations are localized in the telomerase reverse transcriptase (TERT) gene promoter (76%) and TP53 (59%) followed by RB1 (22%), ERBB2 (14%), and CDKN1A (8.3%) (23–27).
Telomerase activity, generally undetectable in normal somatic cells, significantly increases in the majority of tumours causing elongation of telomeres at chromosomes ends and limitless replication of neoplastic cells (28). Multiple molecular mechanisms are involved in telomerase overexpression, including structural chromosomal alterations, copy number gains of the TERT locus, and activating mutations within the TERT promoter region (29). Recurrent activating mutations in TERTp, primarily hot spot mutations C228T and C250T, first identified in melanoma by Horn et al. (2013) and Huang et al. (2013), are among the most prevalent genetic alterations across various cancers, including bladder urothelial carcinoma (30–34). These mutations lead to the permanent activation of telomerase expression, by creating de novo consensus binding sites preferentially bound by the multimeric ETS factor GABPA/B1 (35–37). In bladder cancer, TERT expression from mutant (C228T) promoter alleles is selectively activated through binding of the transcription factor TRIM28, which undergoes mTORC1-mediated phosphorylation, leading to its dissociation from TRIM24 (38).
Mutations in the promoter region of the TERT gene (TERTp), besides being very frequent in urothelial carcinoma, represent early events in the transformation process since they are detected in the urinary exfoliated cells decades before the diagnosis of bladder cancer (34, 37, 39–41). In the Golestan cohort, which was monitored for up to 14 years, Hosen et al. found TERTp mutations in the urine of 47% of asymptomatic individuals who later developed primary bladder cancer, while no such mutations were detected in the matched control group that remained cancer-free (42). Accordingly, the identification of TERTp mutations in urinary exfoliated cells has emerged as a promising biomarker for early diagnosis of bladder cancer.
The tumour suppressor p53 is a central regulator of cellular homeostasis, controlling processes such as the cell cycle, DNA repair, apoptosis, autophagy, metabolism, and immune response (43). TP53 is the most frequently mutated gene across human cancers, including bladder urothelial carcinoma, with the majority of alterations being non-synonymous mutations generating defective p53 proteins (44). These mutant forms typically lose tumour-suppressive activity, exert dominant-negative effects on wild-type p53, and in many cases acquire gain-of-function properties that promote tumour progression and oncogenesis (45). Urothelial bladder cancer patients with TP53 inactivating mutations have poor overall survival but have a better response to immunotherapy due to increased tumour mutational burden and tumour associated antigens (46). Therefore, there is an urgent need for additional studies in bladder urothelial cancer clarifying how the type of TP53 mutation within a tumour can best be used as a predictive biomarker.
The specific aims of this study were to provide a detailed genomic analysis of recurring mutations in bladder urothelial carcinoma and to evaluate the impact of co-occurring mutations in TERTp and in TP53 gene on patient’s clinical outcome in order to possibly develop a bladder cancer informed molecular classification system.
Methods
Patients and data collection
The cBioPortal database was queried to identify bladder cancer datasets, resulting in 21 independent genomic studies publicly available for analyses (Supplementary Table S1). Studies were categorized according to the availability of TERTp mutation data, along with annotated somatic mutations in coding regions, and survival time. TERTp mutation status along with survival information, were available only for the Bladder Cancer (MSK, Cell Reports 2022) study, which was therefore included as the principal dataset in the analyses (47). The Bladder Urothelial Carcinoma SWOG S1314 Trial (MSK, JCO Precis Oncol 2024) cohort containing information regarding TERTp but not survival time was analysed as independent validation set to confirm the robustness of association between TP53 and TERTp (48).
The principal dataset included a total of 1,659 samples from 1,244 bladder cancer patients treated and enrolled at the Memorial Sloan Kettering Cancer Center (MSK) from 1999 to 2021 (ClinicalTrials.gov, NCT01775072) (47). All samples have been analysed with the MSK-IMPACT^®^ (Integrated Mutation Profiling of Actionable Cancer Targets), targeted sequencing assays developed at Memorial Sloan Kettering Cancer Center that detect clinically relevant genetic alterations and enable mutation profiling across a broad range of genes. Tumours were profiled using the MSK-IMPACT341 (n = 46), MSK-IMPACT410 (n = 196), MSK-IMPACT468 (n = 825), and MSK-IMPACT505 (n = 44) panels, all of which included the genes selected for this study.
Applying the selection criteria “cancer type = bladder cancer” and “cancer type detailed = bladder urothelial carcinoma” yielded a cohort of 1,111 patients whose samples derived from primary tumour (n=960), local recurrence (n=1) and metastasis (n=150). Demographic, clinical, pathologic and treatment information, along with the somatic mutation types and mutation sites, were retrieved through the search options in cBioPortal and downloaded as.tsv files. Patients’ information included sex, age at bladder cancer diagnosis, smoking habit (active, former, never), treatment history, survival time (months). Tumour features included the histological classification, TMB, microsatellite instability (MSI) score and prevalent gene mutations (47). The primary objective of the study was to identify differences in the overall survival between four groups of patients according to TERTp and TP53 mutation status: TERTp and TP53 wild type tumours (wt/wt), TERTp mutant and TP53 wild type tumours (TERTp), TERTp wild type and TP53 mutant tumours, TERTp and TP53 double mutant tumours (TERTp/TP53).
The Bladder Urothelial Carcinoma SWOG S1314 Trial (MSK, JCO Precis Oncol 2024) cohort including 184 cases of bladder urothelial carcinoma that were analysed with the MSK-IMPACT assay, was used to validate the significance of TERTp and TP53 co-occurrence (Supplementary Figure S2) (48).
Mutation annotation and co-mutations definition
Complete datasets of genes harbouring somatic mutations with a frequency ≥10% were queried using the search function in cBioPortal, and the corresponding files were downloaded for further analysis. For TERTp, only tumour cases harbouring recurrent mutations at positions C228T and C250T, which have been shown to activate TERT expression, were classified as TERTp mutant, all other cases were assigned to the TERTp wild-type group. In addition, we assessed the co-occurrence of cancer driver mutations in TERTp and TP53 genes as well as their impact on the overall survival of bladder cancer patients. Other frequently mutated genes included KDM6A, ARID1A, KMT2D, FGFR3, PIK3CA, RB1, ELF3, KMT2C, CREBBP, ERBB2, CDKN1A, ATM, FAT1, STAG2, KMT2A, EP300, TSC1, ERBB3 and ERCC2, and their relationship with TERTp and TP53 mutations was evaluated. Co-mutations were classified at the gene level: two genes were considered to be co-mutated if they each had at least one mutation, the actual number of mutations in each gene were not taken into consideration. For example, if one sample harboured two mutations in gene A and three mutations in gene B, only one co-mutation was considered. Each gene was assigned a binary value 0 or 1 for wild type and mutated status, respectively.
Statistical analysis
Categorical variables were expressed as numbers and percentages, continuous variables as medians and interquartile ranges (IQRs). The presence of missing data has been reported in Table 1. Differences between groups organized by tumour mutation status (wt/wt, TERTp, TP53, and TERTp/TP53) and clinical covariates were assessed using the Kruskal–Wallis test or the Fisher exact test. Co-mutations analyses were performed using the Chi-square test and the results were adjusted for the false discovery rate with q-value <0.05 considered as statistically significant. The mutations in TP53 gene and TERTp as well as in other cancer driver genes and their association with survival probability in bladder cancer patients have been evaluated. The survival time was calculated from the date of diagnosis to the date of death from bladder cancer or the last follow-up visit. A log-rank test was performed to identify the significance of differences between the survival curves. Univariate analyses or multivariate Cox regression models were used to assess the hazard ratio (HR) with 95% confidence intervals (CI) to assess the prognostic effect of TERTp and/or TP53 status, age at diagnosis, smoking history, MSI score and TMB. Multivariable Cox regression analyses were performed using a complete-case approach, including only patients with full documentation for all variables entered the model. The proportional hazards assumption for the Cox models was formally evaluated and confirmed by evaluating the independence between Schoenfeld residuals and time. P values <0.05 were considered statistically significant. All analyses were performed using RStudio (R version 4.3.2) with R packages “tidyverse”, “janitor”, “dplyr”, “gtsummary”, “table1”, “survival” and “survminer”.
Results
Patients’ characteristics
We performed a retrospective study of 1,111 bladder urothelial cancer cases. All demographic, pathologic and genomic data were collected for patients with localized or metastatic bladder urothelial carcinoma referring to Memorial Sloan Kettering Cancer Center (MSK) from 1999 to 2021, and publicly available through the https://www.cbioportal.org/. Molecular data were available for 960 primary tumours, 150 metastasis and one local recurrence samples. The clinical characteristics of the patients are reported in Table 1. The median age at cancer diagnosis was 66 years (IQR range, 58–73 years). The patient group included 261 females and 849 males (sex ratio 1:3). The majority of patients were former smokers (n=538), followed by never smokers (n=363), and active smokers (n=116). Overall, 64% of the patients were active or former smokers and 36% never smoked. Most bladder urothelial carcinomas were poorly differentiated grade 3 (G3, 72%). A group of patients (24%) received intravesical therapy, including BCG, chemotherapy or both. A second group received systemic therapy (15%), including chemotherapy, immunotherapy or both therapies. Patients who received intravesical or systemic treatments were grouped in “intravesical treated” and in “systemic treated”, respectively, without further distinction by type of therapy. A total of 748 patients were naïve to any treatment.
Gene mutations in bladder cancer
The median MSI score was 0.2 (IQR, 0 - 0.66), with most tumours classified as MS stable (97%) having a score below 3.5 (Table 1). Few cases (1%) had low MS instability (MS Instable L, score equal or higher than 3.5 and lower than 10) or (1%) high MS instability (MS Instable H, score equal or higher than 10). The median TMB score for the 1,111 patients was 9.5 (IQR, 5.9 – 17). Genetic alterations, including gene amplification and copy number variations, were rare, occurring in less than 5% of cases at both the TERT locus and TP53 (Supplementary Figure 1). The most frequent mutations were single nucleotide changes in TERTp, with the hotspot mutations C228T and C250T observed in 62.3% (692/1,111) and 10% (111/1,111) of cases, respectively. Mutations other than C228T and C250T, whose impact on TERT expression has not been characterized, accounted for 5.2% (58/1,111). In the analyses, only tumours harbouring C228T or C250T mutations, which are known to activate TERT expression, were classified as TERTp mutant, while all remaining tumours were assigned to the wild-type group. Among genes with mutation rates above 10%, eleven are classified as oncosuppressors (TP53, KDM6A, ARID1A, CREPPB, KMT2C, RB1, CDKN1A, FAT1, ATM, ELF3, TSC1) and nine as oncogenes (FGFR3, KMT2D, PIK3CA, ERBB2, ERCC2, STAG2, EP300, KMT2A and ERBB3), according to https://bioinfo.uth.edu/TSGene/. The TP53 mutations were the most frequent, occurring in 49% of cases (548/1,111). In addition, a high mutation rate was observed in genes involved in chromatin remodelling, such as histone methyl transferases KMT2D, KMT2C and KMT2A, the histone demethylase KDM6A, histone acetyltransferases EP300 and CREBBP, as well as ARID1A, which is a part of chromatin SWI/SNF nucleosome-remodelling complex.
We compared the mutation frequencies of mutant genes between TERTp wild type and TERTp-mutant bladder cancer samples (Supplementary Table S2). Overall, nine genes exhibited significantly higher mutation frequencies, after multiple testing correction (q < 0.05), in TERTp-mutant compared with wild-type bladder cancer cases. Such genes included CDKN1A, RB1, ERBB2, ARID1A, PIK3CA, TSC1, TP53, ELF3, KMT2A. Functionally, these co-mutations involve both tumour suppressors (e.g., CDKN1A, RB1, ARID1A, TSC1, TP53, ELF3) and oncogenes (e.g., ERBB2, PIK3CA, KMT2A), suggesting that TERTp mutations often coexist with other driver alterations that promote tumour proliferation, genomic instability, and telomerase activation. Notably, these mutant genes are functionally involved in cell cycle regulation (CDKN1A, RB1, TP53), chromatin remodelling (ARID1A, KMT2A), and activation of oncogenic signalling pathways (ERBB2, PIK3CA).
Moreover, distinct mutational patterns were observed between TP53 mutant and TP53 wild type bladder cancers (Supplementary Table S3). Four genes showed significant higher mutation frequencies in TP53-mutant cases (q<0.05), including RB1, ERBB2, TERTp, TSC1, suggesting cooperative effect in tumour progression (Supplementary Table S3). Of note, in TP53-wild-type tumours the most frequent mutations (q<0.05) were identified in FGFR3, CDKN1A, and STAG2, while typically absent in TP53-mutant cases, indicating that alterations in these genes and TP53 are mostly mutually exclusive.
The TERTp/TP53 double-mutant subgroup displayed high frequency of driver mutations in several genes, such as RB1, ERBB2, ARID1A and KMT2A, with ERBB2 exhibiting the most marked shift (13% versus 24%), (Table 2). Among tumour suppressors, RB1 displays a striking increase in mutations (6.8% versus 36%), underscoring extensive genomic instability associated with TERTp/TP53 co-mutations. Conversely, other tumour suppressor genes, such as FGFR3 (33% in wild type versus 12% in mutants) are significantly more mutated in the wild-type group. This suggests the existence of distinct oncogenic pathways in tumours that retain wild type TERTp/TP53, characterized by an alternative mutation spectrum, particularly involving FGFR3. Other genes, such as ARID1A, KMT2A and PIK3CA also show statistically significant differences, though with more moderate effect sizes. After false-discovery-rate correction, these associations remain robust (q < 0.05 for all significant genes), reinforcing their biological relevance.
Mutation analysis in the validation cohort, which included 184 bladder urothelial carcinoma cases, confirmed that TERTp and TP53 mutations were the most frequent genetic alterations, occurring in 80.4% (148/184) and 65.2% (120/184) of cases, respectively. A significant co-occurrence between TERTp and TP53 mutations was also observed (Supplementary Figure S1).
TERTp and TP53 mutations in urothelial bladder cancer and overall survival analyses
Among the 1,111 urothelial bladder cancer patients, 176 had tumours with wild-type TERTp and TP53 (wt/wt), 387 had TERTp-mutated tumours (TERTp mut/TP53 wt), 132 had TP53-mutated tumours (TP53 mut/TERTp wt), and 416 were TERTp and TP53 double mutant tumours (TERTp mut/TP53 mut) (Table 3). There were no significant differences between groups in the median age (P = 0.3), sex (P = 0.8), or smoking history (P = 0.5). The percentage of tumours classified as grade G3 was higher in the TERTp/TP53 co-mutated tumours (92%) than in other groups (68% of TERTp mut/TP53 wt and 82% of TERTp wt/TP53 mut tumours compared to 54% of wt/wt, P<0.001). Furthermore, patients with double mutant tumours had higher mutation burden (13 mutations/Mb) versus the other groups (8 mutations/Mb for wt/wt, 10 for TERTp wt/TP53 mut wt, and 8 for TERTp wt/TP53 mut, P< 0.001).
Univariate Cox regression analysis showed that several clinical and molecular factors were associated with overall survival (Table 4). In the entire cohort, older age, smoking history, higher tumour grade (G3), and the presence of TERTp or TP53 mutations, individually or combined, were significantly associated with poorer survival. These associations were primarily observed in the untreated patients subgroup, where age, smoking, high-grade tumours, and TERTp and TP53 alterations remained strong predictors of unfavourable outcomes. In contrast, among patients with systemic treatments, no variables were significantly associated with survival, suggesting that therapy may attenuate their negative prognostic effects. Interestingly, co-occurring mutations in TERTp and TP53 were linked to improved survival in systemic treated patients, although this did not reach statistical significance (HR = 0.77, 95% CI: 0.35–1.66, p = 0.5), highlighting a potential predictive effect on treatment response.
A multivariate Cox proportional hazards regression analysis was performed to assess the independent prognostic impact of clinical and molecular variables on overall survival in untreated patients (Table 5). Increasing age (HR = 1.03, 95% CI 1.02–1.05, p < 0.001), smoking history, including both current and former smokers (HR = 1.56, 95% CI 1.10–2.21, p = 0.012), higher tumour grade (G3, HR = 2.97, 95% CI 1.83–4.82, p < 0.001) were significantly associated with higher mortality risk. With respect to pathogenic variants, TERTp mutations (TERTp mut/TP53 wt) were independently associated with increased risk of death (HR = 1.88, 95% CI 1.05–3.40, p = 0.035). TERTp mutations (TERTp wt/TP53 mut) showed a borderline association with poorer survival (HR = 1.95, 95% CI 1.00–3.83, p = 0.051). Notably, the presence of concurrent TERTp and TP53 mutations (TERTp mut/TP53 mut) conferred the highest risk and remained a significant independent predictor of poor outcome (HR = 2.06, 95% CI 1.15–3.70, p = 0.015), suggesting an additive or synergistic negative prognostic effect in untreated patients.
The Schoenfeld residual-based test of the proportional-hazards assumption for overall survival is reported in Supplementary Table S4. For all variables (age, smoking status, and mutant groups), p-values are > 0.05 and rho values are small, indicating no evidence of violation of the proportional-hazards assumption and supporting the validity of the Cox model.
To investigate the prognostic impact of concurrent TERTp and TP53 mutations, we performed Kaplan–Meier survival analyses stratifying patients according to their mutational status. As shown in Figure 1, in the analysis including all patients, survival outcomes differed significantly among the four groups (wt/wt, TERTp wt/TP53 mut, TERTp mut/TP53 wt, and TERTp mut/TP53 mut; log-rank p <0.001), (Figure 1A). Patients harbouring concurrent TERTp and TP53 mutations exhibited the poorest survival, with a marked decline in survival probability beginning around 24–30 months. Whereas patients with TERTp wt/TP53 wt demonstrate the most favourable prognosis, with the median not reached within the observed follow-up. Single-mutant subgroups (TERTp mut/TP53 wt and TERTp wt/TP53 mut) showed intermediate outcomes. To exclude potential confounding effects of therapy, we next examined survival in the subset of untreated patients. The same pattern was observed, with significantly worse outcomes for the TERTp mut/TP53 mut group (log-rank p < 0.001), (Figure 1B). Additionally, Kaplan–Meier analyses in the untreated cohort demonstrated that older age (≥65 years), former or active smoking, and high-grade (G3) tumours were associated with lower overall survival probability (log-rank p = 0.0088, 0.0024, and <0.0001, Supplementary Figure S3). Median survival was not reached in any group, consistent with the observation that co-occurring mutations in TERTp and TP53 reduced survival probability.
Kaplan-Meier survival analysis according to TERTp and TP53 mutation status. (A) Kaplan-Meier survival curves for all patients stratified by combined TERTp and TP53 mutation status. (B) Kaplan-Meier survival curves for untreated patients only.
In patients who received systemic treatment (Supplementary Figure S2), Kaplan–Meier survival analysis stratified by TERTp and TP53 mutations showed no significant differences in overall survival among the four groups (log rank p = 0.84). Survival curves largely overlapped and median survival times were comparable across groups. Conversely, among patients treated with intravesical therapy, overall survival differed significantly according to TERTp and TP53 mutational status (log rank p = 0.029). Patients harbouring concurrent TERTp and TP53 mutations exhibited the earliest decline in survival and reached median survival earlier than other groups. Patients with either TERTp or TP53 mutations alone showed intermediate outcomes, whereas patients with wild-type TERTp and TP53 demonstrated the most favourable survival.
Discussion
For many years, studies on cancer molecular profiling have primarily been based on whole-exome sequencing, which largely excludes non-coding regions (49). Consequently, nucleotide alterations in regulatory elements such as TERTp C228T and C250T mutations and their coexistence with other cancer driver genes have not been systematically investigated (50). More recently, the use of whole-genome sequencing and targeted sequencing panels such as MSK-IMPACT has enabled the inclusion of these non-coding regions, allowing for the detection of TERTp mutations together with other clinically relevant genetic alterations (32, 41).
In the present study, we assessed the presence of concomitant TERTp mutations in bladder urothelial cancer, and we observed a cooperative association between co-occurring mutations in TERTp and TP53, which are shown to influence the clinical outcome. The results showed that 72% and 49% of urothelial bladder carcinoma harboured mutations in TERTp (C228T and C250T) and in TP53 gene, respectively. Notably, 37% of tumours carried concurrent TERTp and TP53 mutations, reflecting a statistically significant tendency toward co-mutation. The significant co-occurrence of TERT promoter and TP53 mutations was validated in the Bladder Urothelial Carcinoma SWOG S1314 trial cohort, confirming the robustness of this association (48). Nevertheless, the molecular pathways connecting these alterations and their potential cooperative effects remain to be determined. Mutational profiles of TERTp and TP53 did not differ significantly by sex, age, or smoking history. However, the marked sex imbalance (849 males versus 261 females) is consistent with epidemiological data that bladder cancer incidence is approximately four times higher in men than in women (51).
Emerging evidence suggests that sex disparity may arise from biological differences in how oncogenic mutations are subjected to selection and accumulation in the bladder urothelium (52). A recent study demonstrated that the type of genetic alterations identified in mutant clones of normal urothelium differs markedly by sex, age and smoking history (53). Mutational analyses, performed by ultradeep sequencing across 16 genes, have shown that normal urothelium in males exhibits a significant higher burden of truncating mutations in RBM10, CDKN1A, and ARID1A genes compared to females. This sex-specific clonal selection may contribute to the higher incidence of bladder cancer in men by expanding premalignant fields long before tumour development. TERTp mutations have also been shown to drive clonal cell expansions in normal urothelium in both males and females, but they are detected almost exclusively in individuals over 55 years of age and are more prevalent among those with a history of smoking (53).
Mutations in TERTp showed significant enrichment of mutations in oncosuppressors (ARID1A, CDKN1A, RB1, TP53) and in oncogenes (ERBB2, PIK3CA, KMT2A), indicating that telomerase activation frequently co-occurs with additional genetic events that enhance proliferative capacity and genomic instability. Conversely, cancers harbouring TP53 mutations showed higher frequencies of RB1 nucleotide changes, whereas TP53 wild-type tumours were enriched for alterations in FGFR3, ELF3, CDKN1A, and STAG2. Tumours carrying TERTp/TP53 mutations were characterized by a sharp increase in RB1 mutations (6.8% to 36%). On the other end, TERTp/TP53 wild-type tumours carry a significant high number of mutations in FGFR3 gene (33%).
Similar patterns of co-mutations were observed in the AACR Project GENIE, with TP53 mutations mutually exclusive with FGFR3 and KDM6A, while TP53 and RB1 mutations co-occurred, indicating potential mutual exclusive and cooperative roles in tumorigenesis, respectively (54, 55). In addition, TP53 and TERT mutations were enriched in metastatic tumours, whereas RB1, KDM6A, and KMT2D were more common in primary tumours. No significant differences were observed for ARID1A, FGFR3, or CDKN2A between metastatic and primary tumours in such cohort.
These divergent mutation patterns support the existence of specific tumour molecular subtypes. Previous studies showed that bladder cancers harbouring concurrent RB1 and TP53 alterations consistently exhibit multiple features linked to better immunotherapy response, including stronger immune infiltration, enhanced interferon signalling, and reduced TGF-β activity (56). They also exhibit higher proliferation, higher TMB and increased tumour-infiltrating lymphocytes. Together, these characteristics suggest that dual RB1/TP53 loss defines a more immunogenic bladder cancer subtype with elevated sensitivity to immune-checkpoint inhibition.
The identification of TERTp and TP53 mutations in urothelial bladder carcinoma has been reported to have important clinical implications (57). TERTp mutations have been shown to consistently predict improved immunotherapy outcomes independently from the TP53 status, suggesting that enhanced TERT activity may increase responsiveness to PD-1/PD-L1 blockade. In addition, TERTp mutations or TERT overexpression have been described to define a biologically aggressive, stage-specific subset of urothelial carcinoma, linked to poor survival and platinum resistance in advanced disease but better responses to PD-1/PD-L1 blockade, highlighting the potential of telomerase activation as context-specific biomarker (57).
On the other hand, patients with TP53-mutant bladder carcinoma might benefit from emerging therapeutic approaches aimed at restoring wild-type p53 function, such as small molecules, gene therapy and other strategies (45). Similarly, patients with TERTp-mutant tumours may be candidates for therapeutic approaches that directly inhibit telomerase or target signalling pathways linked to telomerase activation (58). Integrating TERTp/TP53 mutation status into clinical decision-making could refine prognostic models and guide the development of combination therapies that target telomerase and/or mutant TP53 in conjunction with immunotherapy approaches.
The association of TERTp and TP53 mutations has been studied in other types of cancer such as hepatocellular carcinoma, brain cancer and melanoma (59, 60). In hepatocellular carcinoma, TERTp and TP53 co-mutations were more frequently identified in male patients, in moderately differentiated tumours and associated with a significant higher risk of tumour relapse and shorter progression-free survival (59). The frequent coexistence of TERTp and TP53 mutations in bladder cancer with high tumour grade and poor outcomes supports their association with an aggressive tumour phenotype. However, it remains unclear whether these mutations directly drive tumour aggressiveness or they represent markers of later disease stages.
In our analyses, TERTp and TP53 mutation status in bladder cancer patients who did not received intravesical or systemic therapy was significantly associated with poorer overall survival in univariate analyses and retained independent prognostic significance in the multivariate model when adjusted for age, smoking status, and tumour grade. These results suggests that TERTp and TP53 mutations have a robust, independent association with adverse outcomes and supports their role as biologically distinct cancer drivers in urothelial carcinoma.
Our study has several limitations. First, its retrospective design and reliance on publicly available datasets may introduce selection bias. Second, while our analysis provides detailed analysis on the associations between TERTp and TP53 mutations, experimental validation of their cooperative role is needed to clarify the underlying biological mechanisms. Third, we attempted to identify independent validation cohorts with comprehensive TERTp and TP53 mutation data linked to clinical outcomes, however, publicly available datasets covering non-coding regions of human cancer genomes are currently limited, including urothelial carcinoma. Finally, our study does not address potential therapeutic implications, and prospective studies integrating mechanistic experiments and treatment response data are required to confirm these associations and evaluate the feasibility of targeting TERTp and/or TP53 co-mutations in clinical interventions. Nevertheless, the findings might provide valuable clinical observations to guide future research to identify predictive biomarkers of clinical outcome and therapeutic response.
Conclusions
Further research, including large-scale genomic analyses and prospective clinical studies, is needed to better understand the interplay between TERTp mutations, variations in cancer driver genes, environmental risk factors, and clinical outcomes in bladder cancer. Clarifying these relationships could potentially lead to the development of more personalized prognostic markers and therapeutic strategies for this disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 2Halaseh SA Halaseh S Alali Y Ashour ME Alharayzah MJ . A review of the etiology and epidemiology of bladder cancer: all you need to know. Cureus. (2022) 14:e 27330. doi: 10.7759/cureus.27330, PMID: 36042998 PMC 9411696 · doi ↗ · pubmed ↗
- 3Freedman ND Silverman DT Hollenbeck AR Schatzkin A Abnet CC . Association between smoking and risk of bladder cancer among men and women. JAMA. (2011) 306:737–45. doi: 10.1001/jama.2011.1142, PMID: 21846855 PMC 3441175 · doi ↗ · pubmed ↗
- 4van Osch FH Jochems SH van Schooten FJ Bryan RT Zeegers MP . Quantified relations between exposure to tobacco smoking and bladder cancer risk: a meta-analysis of 89 observational studies. Int J Epidemiol. (2016) 45:857–70. doi: 10.1093/ije/dyw 044, PMID: 27097748 · doi ↗ · pubmed ↗
- 5Cumberbatch MG Cox A Teare D Catto JW . Contemporary occupational carcinogen exposure and bladder cancer: A systematic review and meta-analysis. JAMA Oncol. (2015) 1:1282–90. doi: 10.1001/jamaoncol.2015.3209, PMID: 26448641 · doi ↗ · pubmed ↗
- 6Zhang Y . Understanding the gender disparity in bladder cancer risk: the impact of sex hormones and liver on bladder susceptibility to carcinogens. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. (2013) 31:287–304. doi: 10.1080/10590501.2013.844755, PMID: 24171436 PMC 3852434 · doi ↗ · pubmed ↗
- 7Sanli O Dobruch J Knowles MA Burger M Alemozaffar M Nielsen ME . Bladder cancer. Nat Rev Dis Primers. (2017) 3:17022. doi: 10.1038/nrdp.2017.22, PMID: 28406148 · doi ↗ · pubmed ↗
- 8Burger M Catto JW Dalbagni G Grossman HB Herr H Karakiewicz P . Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. (2013) 63:234–41. doi: 10.1016/j.eururo.2012.07.033, PMID: 22877502 · doi ↗ · pubmed ↗