Effects of Cash Transfer and Incentive Programs on Service Utilization and Treatment Outcomes Related to Neglected Tropical Diseases and Their Impact on Health and Nutrition in Low- and Middle-Income Countries: Protocol for a Systematic Review
S M Tafsir Hasan, Radhika Dayal, Amena Al Nishan, Sunetra Ghatak, Puja Chakraborty, Sudeshna Maitra, Sumaiya Tasneem Raisa, Nizamuddin Khan, Dinesh Mondal, Tahmeed Ahmed, Avishek Hazra

TL;DR
This study reviews how cash transfer and incentive programs affect neglected tropical disease treatment and health outcomes in low- and middle-income countries.
Contribution
The study introduces a systematic review protocol to assess the impact of financial incentive programs on NTD service utilization and health outcomes in LMICs.
Findings
The review will examine how financial incentives influence NTD-related service use and treatment outcomes.
It will explore how program design and covariates affect these outcomes and their impact on health and nutrition.
Findings will guide policymakers in developing strategies for NTD control in low- and middle-income countries.
Abstract
Despite a global decreasing trend in neglected tropical diseases (NTDs), progress is not on track to meet the Sustainable Development Goals by 2030. Evidence suggests a positive effect of conditional cash transfer programs on controlling NTDs. However, it remains to be evaluated whether other financial incentive programs exert similar effects on NTD-related service utilization and treatment outcomes in low- and middle-income countries (LMICs). This systematic review aims to evaluate the effects of cash transfer and incentive programs on NTD-related service utilization and treatment outcomes in LMICs; to examine how covariates, program design, and implementation plan influence these outcomes; and to examine how NTD-related service utilization and treatment outcomes influence nutritional status and health in LMICs. This review will follow the PICOS (Population, Interventions,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
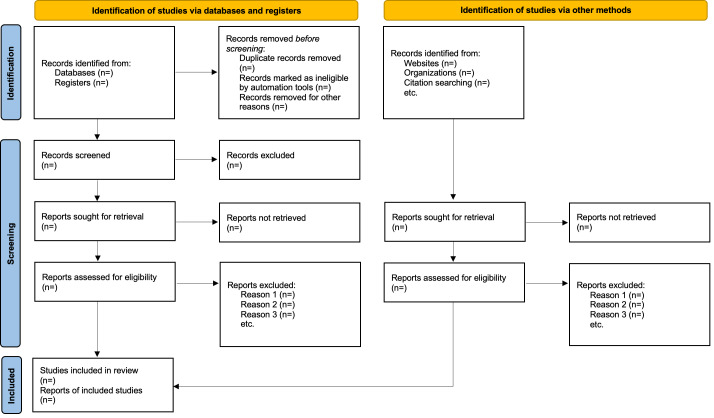 Figure 1
Figure 1| Serial | NTD name | Core strategic interventions | Treatment outcomes | ||||
|---|---|---|---|---|---|---|---|
| Innovative and intensified disease management | Preventive chemotherapy | Vector control | Veterinary public health measures | Provision of safe WASH | |||
| 1 | Buruli ulcer | Early detection, case management (provision of antibiotics: rifampicin, clarithromycin, moxifloxacin, streptomycin, and hygienic wound care) | Bacillus Calmette–Guérin (BCG) vaccination | Aquatic insects, adult mosquitoes, possums, and biting arthropods | Not applicable | Safe water storage practices | Disability, morbidity management including surgery, wound, and lymphedema |
| 2 | Chagas disease | Case management (benznidazole and nifurtimox), MDA | Blood screening before blood transfusion and organ transplantation | Spraying with residual insecticides to remove triatomine bugs, home cleanliness, and housing improvements (eg, crack-free walls, bed nets), wear protective clothing | Not applicable | Good hygiene practices | Prevalence, incidence, detection rate, cure rate, surgery rate, disability rate, death rate |
| 3 | Dengue and chikungunya | Case management (fluid management, proactive treatment of hemorrhage, such as platelet transfusion or whole blood transfusion, paracetamol) | Vaccination (dengue) | Reducing mosquito habitats (eg, environmental | Not applicable | Safe water storage practices, safe water disposal, waste management | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 4 | Dracunculiasis | Surveillance, early detection of cases, case containment, cash reward scheme for voluntary reporting, metronidazole or thiabendazole, health education | Not applicable | Temephos to control water fleas/cyclops | Proactive tethering of dogs | Safe drinking water supply and sanitation, water filtration, preventing water contamination | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 5 | Echinococcosis | Albendazole prophylaxis, surgery, early detection by ultrasound | Not applicable | Not applicable | Deworming of dogs, foxes, vaccination of sheep, safe slaughtering and disposal | Handwash, avoiding contaminated food and water | Prevalence, incidence, detection rate, cure rate, disability rate, surgery rate, total or partial cystopericystectomy, liver damage, death rate |
| 6 | Foodborne trematodiases | Anthelminthic medicines (praziquantel, triclabendazole), PAIR (puncture, aspiration, instillation, and respiration) methods, surgery (partial hepatectomy), Provision of care and rehabilitative services | MDA with triclabendazole ( | Not applicable | Livestock and domestic animal treatment, safe fish farming, one health intervention | Safe disposal of fecal waste, safe water, safe food practices, safe WASH practices | Prevalence, incidence, detection rate, cure rate, disability rate, surgery rate, liver damage, death rate |
| 7 | Human African trypanosomiasis | Screening clinic attendance, active case detection, treatment of gHAT | Not applicable | Baits and traps, impregnated screens, insecticide spraying, reducing the disease reservoir, controlling the tsetse fly vector | Treatment of animals (cattle, pigs) | Safe water, safe WASH practices | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 8 | Leishmaniasis | Early diagnosis, cryotherapy, thermotherapy, medication (liposomal amphotericin B, pentavalent antimonials, miltefosine), rapid diagnostic test rk-39 | Not applicable | Insecticide spraying, insecticide-treated nets, environmental management, protection from sandfly bites | Rodent control, vaccination for dogs | Safe WASH practices | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 9 | Leprosy | Early detection, MDA, physical therapy, multidrug therapy (rifampicin, clofazimine, dapsone, ofloxacin, and minocycline) | Postexposure prophylaxis of rifampicin, vaccination with BCG, Mycobacterium w (Mw) | Not applicable | Not applicable | WASH in health facility | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 10 | Lymphatic filariasis | Essential package of care (skincare and hygiene, exercises for | MDA, annual MDA with diethylcarbamazine citrate and albendazole, home-based disability alleviation and prevention | Vector control to reduce transmission, avoid mosquito bites | Not applicable | Hygiene, sanitation improvement, personal hygiene and self-care of the affected limbs to avoid secondary | Prevalence, incidence, detection rate, cure rate, disability rate, hydrocele management, surgery rate, mental health, death rate |
| 11 | Mycetoma, chromoblastomycosis and other deep mycoses (paracoccidioidomycosis [PCM], caused by | Long-term itraconazole+ antibiotic administration, physical therapy, wound care, surgery (excision, debridement, amputation) | Self-protection by wearing long clothes, closed-toed shoes | Not applicable | Pet control for sporotrichosis, feral cat management | Personal hygiene and self-care of the affected limbs to avoid secondary infections | Prevalence, incidence, detection rate, cure rate, disability rate, local excision, debridement, amputation, surgery rate, death rate |
| 12 | Noma | Case management with antibiotics, mouthwash, health education | Nutrition supplements | Not applicable | Not applicable | Personal hygiene | Prevalence, incidence, detection rate, cure rate, disability rate (disfiguration), mental health, death rate |
| 13 | Onchocerciasis | Ivermectin, doxycycline, eye care, MDA | MDA of ivermectin for community-based prevention | Insecticides at black fly habitats and larval breeding sites, avoid blackfly bites | Not applicable | Not applicable | Prevalence, incidence, detection rate, cure rate, disability rate (ocular morbidity rate), death rate |
| 14 | Rabies | Postexposure prophylaxis (PEP) with rabies vaccine and rabies immunoglobulin | Pre-exposure vaccination for people at high risk (eg, laboratory staff working with rabies virus, veterinarians and animal handlers) | Wild mammals (dogs, bats) control | Mass vaccination of dogs, mammal pet vaccination, agriculture, livestock, wildlife, environment (One Health) | Not applicable | Prevalence, incidence, detection rate, death rate |
| 15 | Scabies and other ectoparasitoses | Topical scabicides, permethrin, benzyl benzoate, malathion, and sulfur ointment, oral ivermectin | MDA using oral ivermectin | Not applicable | Not applicable | WASH practices, hygiene practices | Prevalence, incidence, detection rate, cure rate, co-morbidities (kidney disease, rheumatic heart disease, systemic infection) |
| 16 | Schistosomiasis | Case management and surgery, education | MDA with praziquantel | Snail control | Keeping animals away from transmission sites | Safe water, improved sanitation, excreta management, hygiene | Prevalence, incidence, detection rate, cure rate, disability rate, surgery rate, death rate |
| 17 | Soil-transmitted helminthiases | Case management (with albendazole/mebendazole/ivermectin), education of hygiene | MDA with albendazole/mebendazole/ivermectin, antenatal care preventive treatment | Not applicable | Not applicable | WASH practices, safe water, improved sanitation, excreta management, hygiene | Prevalence, incidence, detection rate, cure rate, disability rate, death rate |
| 18 | Snakebite envenoming | High-quality, safe, and effective snake antivenoms; wound care; ventilation; surgery; WHO | Protective footwear, sealing house wall, roof and door gaps, bed nets, household rodent controls to keep away the snakes | Not applicable | Not applicable | Not applicable | Prevalence, incidence, detection rate, cure rate, disability rate, surgery rate, intensive care unit (ICU) admission rate, death rate |
| 19 | Taeniasis/cysticercosis | Case management (praziquantel, niclosamide, albendazole), neurological treatment, surgery | MDA with niclosamide/ praziquantel/ albendazole, community awareness | Not applicable | Improved pig husbandry, pig vaccination | WASH practices, proper cooking | Prevalence, incidence, detection rate, cure rate, disability rate (neurological symptoms), surgery rate, death rate |
| 20 | Trachoma | Eye surgery to treat trachomatous trichiasis, TT (the S of the SAFE strategy) Azithromycin | MDA of azithromycin and tetracycline eye ointment (WHO-recommended SAFE strategy) | Reducing breeding sites for muscid flies | Not applicable | Access to water and improved sanitation | Prevalence, incidence, detection rate, cure rate, disability rate (blindness), surgery rate |
| 21 | Yaws | Case management (azithromycin medication, intramuscular benzathine benzylpenicillin), Morges strategy, health education | Mass treatment, also known as total community treatment (TCT), involves giving oral azithromycin (single dose) | Not applicable | Not applicable | Personal hygiene | Prevalence, incidence, detection rate, cure rate, disability rate (disfiguration) |
| Domain | Description | Search terms or keywords |
|---|---|---|
| Population | Participants |
Adults and children living in LMICs Adults, young adults, young women, young men, child, infant, adolescents, teen |
| Interventions | Programs |
Money, monetary, cash, financial transfer, cash transfer, payment, conditional cash transfer (CCT), unconditional cash transfer (UCT), incentive. Financial, nonfinancial incentive programs, eg, social protection, social program, scholarship programs, family allowance, in-kind transfer, food/medicine voucher, and microfinance/microcredit. |
| Outcomes | Neglected tropical diseases and disease groups; core strategic interventions; NTD |
Neglected disease, neglected tropical disease, tropical medicine, tropical disease, Buruli, buruli ulcer, Bairnsdale ulcer, Daintree ulcer, Mossman ulcer, mycobacterium, Early detection, antibiotic, Rifampicin, Clarithromycin, hygiene, wound care, BCG Attendance at screening clinics, treatment adherence, health-seeking behavior, NTD campaign coverage, etc Prevalence, incidence, detection rate, cure rate, disability, disability rate, morbidity, morbidity rate, death rate, lymphedema management, wound management, total cystopericystectomy, partial cystopericystectomy, surgery rate, liver damage, mental health, disfiguration, ocular morbidity, comorbidities, kidney disease, rheumatic heart disease, systemic infection, ICU |
| Study | Design |
RCTs Difference-in-difference, pre-post design, time series, regression discontinuity, instrumental variable estimation, propensity score matching, and qualitative study. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Parasitic Diseases Research and Treatment · Global Maternal and Child Health
Introduction
Background
Neglected tropical diseases (NTDs) remain a major global public health concern, affecting an estimated 1.62 billion people in tropical and subtropical climatic zones [12] and accounting for approximately 200,000 deaths and 14.5 million disability-adjusted life years annually [23]. Although there has been a general decline in the global burden of NTDs [2], the progress is not yet on track to meet the ambitious Sustainable Development Goals 2030 target of a 90% reduction in the number of people requiring interventions for NTDs [3]. NTDs continue to pose a big challenge for low- and middle-income countries (LMICs) due to their intricate links with poverty, inadequate hygiene, poor sanitation, and limited health care access [45].
Poverty is a key factor exacerbating the burden of NTDs in LMICs. Financial deprivation and disease are closely intertwined, which influence the social and environmental determinants of NTDs, including water, sanitation, and hygiene, education, housing, and health care accessibility [5-7]. Poverty highly modulates the accessibility and utilization of the services related to the 5 important NTD control strategies recommended by the World Health Organization (WHO): innovative and intensified disease management; preventive chemotherapy; vector control; veterinary public health measures; and provision of safe water, sanitation, and hygiene practices [89]. NTDs disproportionately affect impoverished and marginalized communities, resulting in increased catastrophic health spending and out-of-pocket expenses [10]. Already living in poverty before the onset of these diseases, affected households often face deeper financial hardship as rising out-of-pocket costs push them further below the poverty line [11-13]. To manage these expenses, they often resort to coping strategies such as borrowing money or selling assets, which further exacerbates their poverty. This cycle undermines access to health care services and negatively affects treatment outcomes [13]. Physical disabilities due to NTDs, such as blindness, lesions, and swelling, may also contribute to decreased income ability [14]. This financial burden perpetuates a cycle of poverty and NTD burden, hindering service uptake and treatment [15]. Consequently, the detrimental effects of NTDs are amplified, including poor NTD-related service utilization and adherence, treatment failure, disability, and deterioration of general health and well-being [15].
Moreover, infection with NTDs increases the nutritional burden of the hosts and impedes overall health. NTDs have been reported to be associated with stunting, anemia, iron deficiency, micronutrient deficiencies, and malnutrition [16-19]. Simultaneously, nutrient deficiency may also increase the susceptibility and vulnerability of NTD-affected individuals and lead to NTD treatment failure [182021]. Actions taken to control NTDs may eventually improve nutritional outcomes, which, in turn, will also influence overall health and well-being, particularly in resource-limited settings.
Despite various programs and policies implementing innovative strategies to improve NTD campaign coverage, multiple layers of poverty-associated and financial obstacles continue to hinder appropriate health-seeking behaviors in affected populations. These barriers include attending screening clinics, receiving adequate care, and treatment adherence [22-25]. Cash transfer programs have demonstrated potential for improving NTD outcomes [26-29]. These programs aim to provide small-scale monetary assistance to individuals or households to break the intergenerational cycle of poverty. Conditional cash transfers (CCTs) impart benefits through a 2-way strategy: direct cash assistance and enforced conditionalities [30]. It is also possible that conditionalities related to the control of NTDs may also impart positive effects on nutrition and overall health outcomes in LMICs. Large-scale, national-level cash transfer programs in Latin America have not only proven effective in improving social protection, economic stability, and sustained developmental outcomes [31] but have also generated interest in using cash transfers to target context-specific health outcomes, including NTD treatment outcomes, maternal health, child health, cognitive development, nutrition, and health care utilization [2632-34undefinedundefined].
A recent systematic review highlighted the positive impact of CCT programs in controlling NTDs. It indicated that the targeted benefits of these programs for vulnerable populations can help reduce health inequalities associated with NTDs. For example, cash transfers have been shown to reduce leprosy incidence and increase the uptake of deworming treatments in certain contexts [35]. However, the review had a major limitation in that it included and synthesized evidence for only 3 of the 21 NTDs and disease groups prioritized by WHO [2335]. While other incentive programs, such as in-kind transfers, microcredits, vouchers for transport, medicines, or food, have shown the potential to promote health knowledge, reduce health inequalities, and improve health-seeking behaviors, their direct or indirect effects on NTD-related indicators have not been comprehensively studied in LMICs [3637].
Given this context, there is a need for an evidence synthesis on the effects of cash transfers and other incentive programs on NTD-related service utilization and treatment outcomes in LMICs. This proposed systematic review and meta-analysis (depending on information availability) will conduct a comprehensive synthesis and unbiased assessment of the existing studies in this area, critically assessing the strengths and limitations of existing evidence.
Objectives
The systematic review aims to answer the following three questions: (1) What are the effects of cash transfer and incentive programs on NTD-related service utilization and treatment outcomes in LMICs? (2) How do incentive program design (type, amount, and frequency), implementation plan, and other covariates influence NTD-related service utilization and treatment outcomes in LMICs? and (3) How do NTD-related service utilization and treatment outcomes influence nutritional status, overall health, and well-being in LMICs?
Methods
Overview
This protocol was developed in accordance with the guidelines of the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) [38]. A PRISMA-P checklist for this protocol is provided in Checklist 1. The protocol has been registered in PROSPERO (CRD42024627804).
Eligibility Criteria
The eligibility criteria for studies to be included in this review are adapted based on the PICOS (Population, Interventions, Comparators, Outcomes, Study Design) framework [39], as described below.
Population
The population of interest in this review will be adults and children of all ages residing in LMICs.
Interventions
For intervention, this review will include programs or policies addressing socioeconomic disadvantages through the provision of cash transfers or financial incentive programs, including but not limited to in-kind transfers, food vouchers, free medicine vouchers, discount coupons, and microcredit to households or individuals.
CCT programs require beneficiaries to comply with certain conditionalities (eg, regular health check-ups) [31], while unconditional cash transfer programs do not set such requirements [40]. Microcredit is the extension of very small loans (microloans) to impoverished borrowers who typically lack collateral, steady employment, and a verifiable credit history [41]. It is designed to support entrepreneurship and alleviate poverty [41]. An in-kind transfer is a transfer of goods or services rather than cash [42]. Other incentive programs may also include giving free medicine vouchers, food vouchers, discount coupons, social protection, social programs, scholarship programs, family allowances, and microfinance.
Comparators
This review will include studies with suitable comparators; studies without comparators will be excluded. Comparators will include individuals or households who did not receive any cash transfers or incentive programs, recipients of cash transfers or incentive programs from the preintervention period, and populations or areas with varying levels of intervention coverage.
Outcomes
The primary outcomes of interest will be service utilization and treatment outcomes related to any of the 21 NTDs and disease groups prioritized by WHO [2]. These include Buruli ulcer; Chagas disease; dengue and chikungunya; dracunculiasis; echinococcosis; foodborne trematodiases; human African trypanosomiasis; leishmaniasis; leprosy; lymphatic filariasis; mycetoma, chromoblastomycosis, and other deep mycoses; noma; onchocerciasis; rabies; scabies and other ectoparasitoses; schistosomiasis; soil-transmitted helminthiases; snakebite envenoming; taeniasis/cysticercosis; trachoma; and yaws.
Service utilization related to WHO-recommended core strategic interventions for each of the 21 NTDs and disease groups will be evaluated. The aspects of service utilization evaluated will include, but not be limited to, health-seeking behavior, attendance at screening clinics, treatment adherence, and NTD campaign coverage. Treatment outcomes related to WHO-recommended core strategic interventions for each of the 21 NTDs will include, but not be limited to, prevalence, incidence, detection rate, cure rate, disability rate, death rate, and components of morbidity management, including surgery, wound management, physiotherapy, and long-term rehabilitation. A comprehensive list of core strategic interventions and treatment outcomes for each of the 21 NTDs and disease groups is provided in Table 1 [1343-48undefinedundefinedundefinedundefinedundefined].
The review will include only studies reporting primary outcomes. However, in the included studies, exploratory outcomes related to the nutrition, health, and well-being of adults and children will be analyzed to examine how NTD-related service utilization and treatment outcomes may influence these outcomes in LMICs. Exploratory outcomes will include, but not be limited to, nutritional status, various types of malnutrition, micro- and macronutrient deficiency, anemia, cognitive development, school attendance and performance, mortality, and morbidity.
Study Design
The review will include randomized controlled trials, as well as nonrandomized studies with comparator groups, such as cohort, case-control, longitudinal, cross-sectional, ecological, and quasi-experimental studies. Additionally, impact evaluation results, program reports, qualitative studies, and studies employing methodologies like difference-in-difference, pre-post design, interrupted time series, regression discontinuity, instrumental variable estimation, and propensity score matching will be considered. Studies reported in the English language will be considered for inclusion.
Search Strategy
A scoping search will be conducted to identify key Medical Subject Headings terms and other relevant search terms, which will then be combined to develop a comprehensive search strategy. Boolean operators (AND, OR, and NOT), truncation/stemming (*), and phrase searching (“”) will be used. The search will focus on NTDs, using genus names along with key terms, such as cash transfer, unconditional cash transfer, CCT, microcredit, food voucher, and incentive. A preliminary search strategy is provided in Table 2.
Article Screening Process
The following databases will be searched: MEDLINE, PubMed, Scopus, Embase, Web of Science, POPLINE, Google Scholar, Cochrane Collection, PsycINFO, Global Health, EconLit, Social Sciences Citation Index, International Bibliography of the Social Sciences, Knowledge Commons of Population Council, and 3ie database. Gray literature databases, including WHO websites, AlignMNH, World Bank, and UNICEF websites, will also be searched for relevant reports. Websites and online resources of universities and research centers in LMICs will be reviewed to identify working papers, dissertations, and theses. Reference lists or bibliographies of included studies will also be hand-searched to include any additional relevant studies. For those studies not available in the public domain, a librarian will be contacted. Studies in English, published or available from 2000 to 2024, will be included. A search log will be maintained throughout the search process to document the database platforms or search interface used, the date the search was conducted, the search strings used, and the number of records or counts identified. The log will be updated as necessary to ensure transparency, robustness, and ease of updating during the study period.
Preliminary search documents will be stored in reference management software (EndNote or Mendeley). All the screened studies will be transferred into Microsoft Excel or Rayyan tool, a systematic review management platform [49].
Title, Abstract, and Full-Text Relevancy
Two reviewers will independently screen studies based on titles and abstracts. During the initial screening phase, decisions made by each reviewer will be blinded. After the initial screening is done, the studies screened by the two reviewers will be compared and checked for discrepancies. Any discrepancies in the categorization will be resolved through consultation between the reviewers or with another reviewer. A second-level independent review will then be conducted by a separate reviewer to perform quality checks on studies with discrepancies and those deemed ineligible. Studies deemed relevant based on titles and abstracts will undergo full-text screening for relevancy, following the same procedures used during the title and abstract screening phase. Reasons for the exclusion of papers will be documented. The studies will be equally divided among the reviewers for relevancy screening. Data will be extracted individually by each reviewer. Any questions arising during the process will be addressed through consultation among the reviewers to reach a consensus. Eligible studies from the full-text review will be entered directly into a master data extraction spreadsheet.
Data Extraction
After the article screening process is completed, all eligible studies will be extracted into a master data extraction spreadsheet. The data extraction sheet will include the following categories: title, author(s), date of publication, type of publication (eg, summary, synthesis, single study), number and type of included studies (if a summary or synthesis), settings and population studied, interventions implemented, outcomes measured and results, and if relevant, whether results differed among subgroups, such as gender, socioeconomic status, or ethnicity. For studies with multiple outcomes or variables, all eligible outcomes will be extracted. The data extraction form will be pilot-tested and refined based on the information extracted from a few initial studies meeting the inclusion criteria. This process will help minimize bias and improve the validity and reliability of the systematic review. Authors will be contacted through email if key information is missing or if further information or clarification is required.
Risk of Bias Assessment for Individual Studies
The quality assessment will be done by using the Revised Cochrane Risk of Bias for randomized trials (RoB 2) [50], the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) [51], the Joanna Briggs Institute (JBI) checklist for analytical cross-sectional studies, and an adapted version of the Critical Appraisal Skills Programme (CASP) [52] for qualitative studies; ecological studies will be evaluated narratively. The quality of each included study will be independently assessed by one reviewer, with the assessment results checked by a second reviewer. Any discrepancies or disagreements will be resolved through consultation with a third reviewer to reach a consensus.
Anticipated Number of Studies to Be Included in the Review
Based on the initial search to develop the protocol, about 20 to 30 studies are anticipated to be included in the review [345354]. This number might change during the actual work of the systematic review based on the search using electronic databases and gray literature.
Data Synthesis
A narrative synthesis will be produced by describing the studies. A geographical information system map will be generated to illustrate the frequency distribution of impact evaluations of cash transfer and incentive programs on NTD-related service utilization, treatment outcomes, nutritional status, and health and well-being, subject to data availability. Interventions of cash transfers and incentive programs will be classified into different categories for different types of NTDs, and their effects will be synthesized for (1) NTD-related service utilization; (2) treatment outcomes; and (3) nutritional status, health, and well-being outcomes. For this review, improvement in nutritional status and health and well-being are considered potential downstream or contextual outcomes that may occur through multiple pathways, in addition to through changes in NTD-related service utilization and treatment outcomes. These pathways may include independent effects of incentives on household resources, food security, health-seeking behavior, and overall living conditions. Given that most primary studies may not be designed to test the full causal pathway, causal inference in this review will be restricted to proximal outcomes (service utilization and treatment outcomes), while nutritional and broader health outcomes will be interpreted as associative and contextual. All the studies will be tabulated by quantitative and qualitative type, and key findings will be described. Primary and exploratory outcomes will be listed along with differences in effectiveness between different cash transfer and incentive programs for NTD control.
We will assess the certainty of evidence for quantitative outcomes using the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach. For qualitative or narrative evidence, we will use an appropriate structured approach (eg, GRADE-CERQual) to evaluate confidence in the findings.
The possibility of performing a meta-analysis will be explored depending on the availability of a sufficient number of relevant studies. The ability to undertake a meta-analysis will depend on the heterogeneity of the measures, such as similarities or differences in population, intervention, outcomes, and methodologies. If a meta-analysis is deemed appropriate, statistical heterogeneity of effects will be assessed using χ^2^ and I^2^ statistics. Efforts will be made to analyze the factors explaining heterogeneity through moderator analysis, including subgroup meta-analysis. All analyses will be contingent on sufficient study density.
For qualitative studies, the themes will be identified using a deductive approach, and the findings will be used to interpret or complement the quantitative findings as part of the narrative synthesis. We will also consider stratifying synthesis by study design strength.
The synthesis will present the factors such as program design, implementation, context, and challenges that influence the impact of cash transfer or incentive programs on NTD-related service utilization, treatment outcomes, nutrition status, and health and well-being. Absolute evidence gaps and synthesis gaps will also be identified that can inform the development of new studies or programs.
Analysis of Subgroups or Subsets
The possibility of performing subgroup analyses will be explored. It will, however, depend on the evidence strength to summarize effects in special populations, such as pregnant women and geriatric populations, or to distinguish effect differences across different levels of groups, such as female/male, child/adolescent/adult, different geographical regions, malnourished/well-nourished, and type of disease agents (viruses, bacteria, protozoa, fungi, helminths, ectoparasites, snakebites). The effects will also be examined to determine how they vary by incentive program design (type, amount, and frequency), implementation plan, study design, and relevant covariates.
Ethical Considerations
The systematic review protocol has been reviewed and approved by two independent institutional review boards: icddr,b (PR-24112) in Bangladesh and Population Council Institute (IORG0011824) in India. Although systematic reviews do not require institutional review board approvals because no human subjects were involved, these approvals were taken as an institutional requirement.
Results
This project is supported by the Children’s Investment Fund Foundation and was funded in March 2024. As of January 15, 2026, an exhaustive article search and title-abstract screening have been completed, and the full-text article screening process is expected to be completed by February 2026. Findings will then be synthesized and reported by the end of April 2026. Based on our initial search, we anticipate that 20 to 30 articles will be included, although the final number may vary. The screening process will be reported using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart (Figure 1) [55].
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Discussion
Principal Findings
We expect that this study will be completed by April 2026. This systematic review will critically examine and provide a comprehensive assessment of the effects of cash transfer and other financial incentive programs on NTD-related service utilization and treatment outcomes in LMICs. A recent systematic review of 11 studies published in The Lancet found that CCTs improve NTD outcomes through both enhanced living standards from the cash benefits and direct health effects linked to health care–related conditionalities [35]. However, this review had a major limitation in that it included and synthesized evidence for only 3 of the 21 NTD groups prioritized by WHO. In contrast, this review will seek evidence across all 21 WHO-prioritized NTDs.
The financial impact of different categories of financial aid for mitigating NTDs will be assessed to inform policymakers about more effective intervention programs and prevention or treatment strategies. Additionally, the potential link between NTD-related service utilization and health and nutrition outcomes in LMICs will be evaluated. A methodological assessment of the published literature will be performed, and the findings will be compared with those of similar reviews to examine the strength of evidence.
The proposed systematic review will synthesize evidence generated over a 25-year period and will critically assess the strengths and limitations of existing studies on NTDs. The use of rigorous methodology and a robust article screening process is expected to ensure a comprehensive, up-to-date, and unbiased synthesis of evidence on the effectiveness of cash transfer and incentive programs in improving NTD-related service utilization, treatment outcomes, and associated health and nutrition outcomes in LMICs.
One of the major anticipated limitations of this systematic review is that the available evidence may include multiple outcome measures and substantial methodological heterogeneity, potentially limiting the feasibility of meta-analysis. Additional limitations may include potential risk of bias in the included studies, possible publication bias, language bias due to the inclusion of English-language articles only, and limitations of the search strategy. We may face limited sensitivity in the electronic database searches because of the extensive NTD-related keywords and the indexing constraints of certain databases. However, supplementary strategies, including bibliographic citation searching and snowballing from the reference lists of included articles and relevant systematic reviews, are expected to help mitigate these limitations.
Conclusion
This systematic review will provide policymakers with evidence to support more effective strategic planning and targeted interventions for controlling NTDs in LMICs. The findings from this systematic review will also be valuable for researchers, funding agencies, and governmental bodies seeking to design and implement effective NTD control programs.
Dissemination Plan
The findings of this systematic review will be presented at national and international conferences and reported in a peer-reviewed journal in accordance with the PRISMA 2020 guideline for reporting systematic reviews [55]. Any amendments to this protocol during the review process will be documented in PROSPERO and reported in the final manuscript.
Supplementary material
10.2196/76450Checklist 1PRISMA-P checklist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hudu SA Jimoh AO Adeshina KA Otalike EG Tahir A Hegazy AA An insight into the success, challenges, and future perspectives of eliminating neglected tropical disease Scientific African Jun 202424 e 02165 doi 10.1016/j.sciaf.2024.e 02165 · doi ↗
- 2Global report on neglected tropical diseases 2024 World Health Organization 0552024 UR Lhttps://iris.who.int/server/api/core/bitstreams/cb 44ed 69-02bd-4273-b 599-26661646 f 5d 3/content Accessed 26-02-2026
- 3Ending the neglect to attain the sustainable development goals: a road map for neglected tropical diseases 2021–2030 World Health Organization 2020 UR Lhttps://www.who.int/publications/i/item/9789240010352 Accessed 02-03-2026
- 4Engels D Zhou XN Neglected tropical diseases: an effective global response to local poverty-related disease priorities Infect Dis Poverty 012820209110 doi 10.1186/s 40249-020-0630-9Medline 31987053 PMC 6986060 · doi ↗ · pubmed ↗
- 5Hotez PJ Fenwick A Savioli L Molyneux DH Rescuing the bottom billion through control of neglected tropical diseases Lancet 0522009373967415701575 doi 10.1016/S 0140-6736(09)60233-6Medline 19410718 · doi ↗ · pubmed ↗
- 6The Causes and Impacts of Neglected Tropical and Zoonotic Diseases: Opportunities for Integrated Intervention Strategies National Academies Press 2011 doi 10.17226/13087 Medline ISBN 978-0-309-18634-621977543 · doi ↗ · pubmed ↗
- 7Coady D Alleviating structural poverty in developing countries: the approach of PROGRESA in Mexico World Bank Group 2003 UR Lhttps://documents 1.worldbank.org/curated/en/435991468757217796/pdf/269430 Coady.pdf Accessed 26-02-2026
- 8Integrating neglected tropical diseases into global health and development: fourth WHO report on neglected tropical diseases World Health Organization 2017 UR Lhttps://iris.who.int/server/api/core/bitstreams/903594 da-27f 0-44f 1-a 1e 8-f 4261 ed 810a 5/content Accessed 26-02-2026