Trends in emotional distress among childhood, adolescent, and young adult (CAYA) cancer survivors: A decade-long study
Pranali G. Patel, Chaitali S. Dagli, Abdulghafoor Alani, Mrudula Nair, Nada Al-Antary, Oluwole A. Babatunde, Dina K. Abouelella, Nosayaba Osazuwa-Peters, Eric Adjei Boakye

TL;DR
This study looked at emotional distress trends among childhood, adolescent, and young adult cancer survivors over a decade and found no significant changes.
Contribution
The study provides a decade-long analysis of emotional distress trends in CAYA cancer survivors using U.S. national survey data.
Findings
The proportion of individuals with mild/no distress increased until 2014 then decreased, but not significantly.
Severe distress decreased by 7.36% annually after 2014, but also not statistically significant.
No significant trends in emotional distress were found when stratified by demographics or mental health access.
Abstract
We examined trends in emotional distress among survivors of childhood and adolescent and young adult (CAYA) cancers. We analyzed the 2008–2018 National Health Interview Survey (NHIS) data among individuals (n = 6451) who were diagnosed with cancer between 0 and 39 years of age. Emotional distress was assessed using the validated Kessler 6-item scale. Respondents rated how often they felt nervous, hopeless, restless, or fidgety, so sad that nothing could cheer them up, that everything was an effort, and worthless in the past 30 days. Responses were scored and added to produce a range of 0–24. We classified emotional distress as mild/no (score of less <5), moderate (score between 5 and 12), or severe distress (≥ 13). Joinpoint regression estimated yearly increases/decreases in psychological distress using annual percent changes. Overall, the proportion of individuals experiencing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
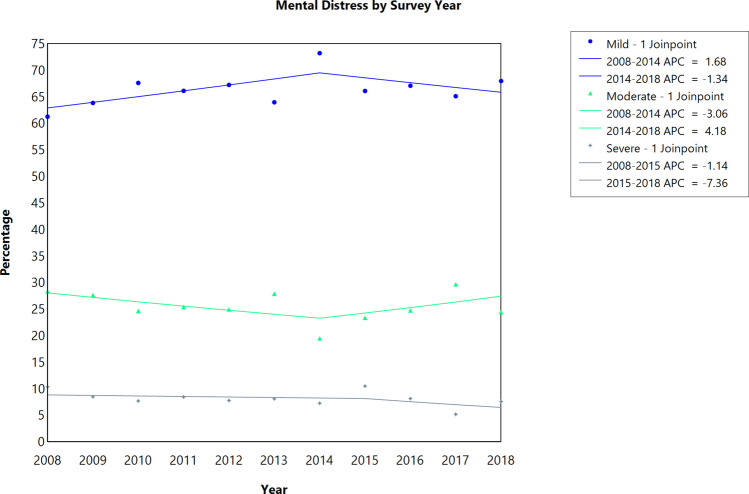 Figure 1
Figure 1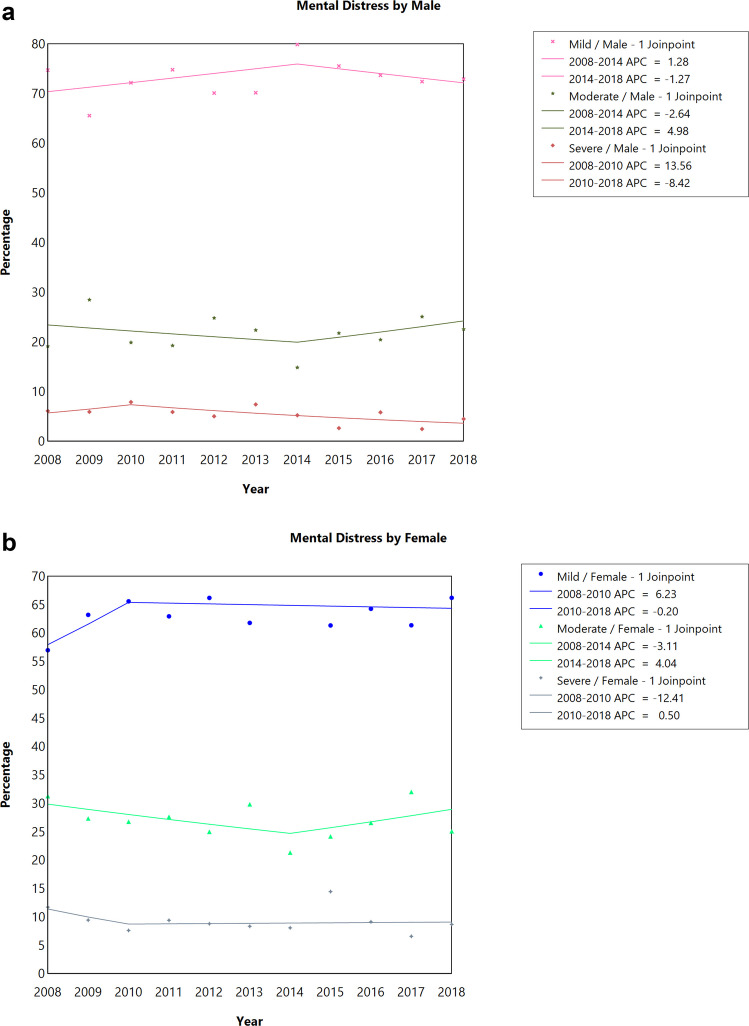 Figure 2
Figure 2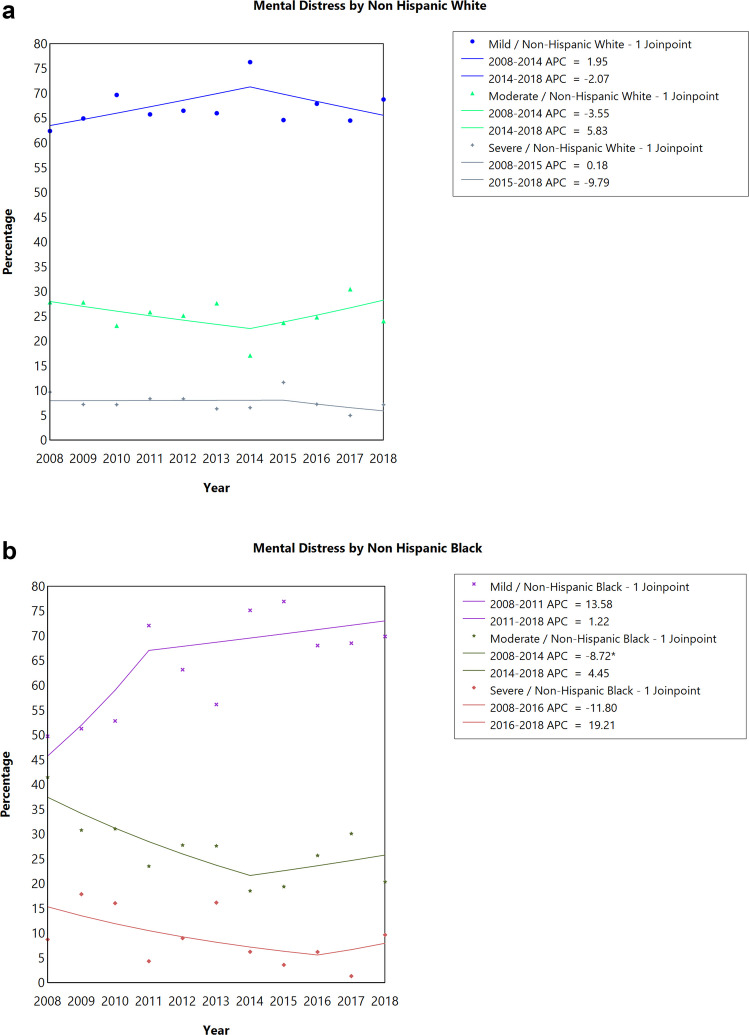 Figure 3
Figure 3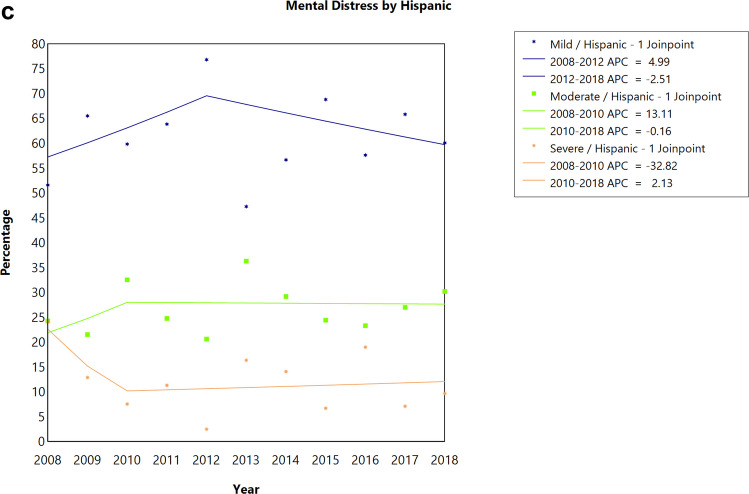 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildhood Cancer Survivors' Quality of Life · Cancer survivorship and care · Family Support in Illness
Introduction
There were approximately 18.1 million cancer survivors in the United States (U.S.) as of January 2022 [1], representing 5.4% of the total U.S. population. By 2040, the number of cancer survivors is projected to reach 26 million [2]. The population of cancer survivors diagnosed at childhood or adolescent and young adult (CAYA) age is currently estimated at 400,000 in the U.S., and it is steadily increasing [2–5]. In addition, with financial burden of an estimated 279,648 per childhood cancer survivor [[6](#CR6)] and 259,324 per adolescent and young adult survivor [7], survivors of CAYA cancer encounter unique challenges.
Navigating the critical transition from adolescence to young adulthood is already psychologically demanding [8]. However, for individuals diagnosed with cancer during this stage, the journey becomes even more complex due to the added physical and emotional challenges of the disease and its treatment. Cancer survivors often experience chronic pain, which is linked to worsened mental health, functionality, and employment outcomes [9]. Recent studies have shown that childhood cancer survivors have more frequent mental health visits [10], a higher prevalence of emotional distress symptoms [11, 12], cognitive impairment, physical disability, and chronic health issues [13]. Adolescent and young adult (AYA) cancer survivors also face a wide range of physical and psychological late effects that significantly impact their quality of life [14]. Compared to survivors diagnosed in middle or older adulthood, survivors diagnosed as AYAs experience a greater prevalence of emotional distress [12]. Another study found that 15.1% of childhood cancer survivors reported experiencing elevated levels of overall emotional distress [13].
However, these studies, being cross-sectional, cannot capture changes in emotional distress over the course of survivorship. Longitudinal studies on childhood cancer survivors indicate that most survivors report minimal to no distress, with elevated symptoms affecting only a specific group, aligning with the concept of post-traumatic growth [15, 16]. Limited research has explored the changes in emotional distress over time among survivors of CAYA cancers. This study aims to examine trends in emotional distress experienced by adult survivors of CAYA cancers between 2008 and 2018 in the U.S. By employing trend analysis, we will identify factors that have changed over time with respect to emotional distress. Understanding these patterns is crucial for optimizing the timing of screening measures and interventions; ultimately helping CAYA survivors manage their distress during critical post-treatment phases, and addressing overlapping challenges and improving quality of life.
Methods
Data source
We examined data from 2008 to 2018 National Health Interview Survey (NHIS), which is conducted annually by the National Center for Health Statistics, Centers for Disease Control and Prevention [17]. NHIS is a cross-sectional household interview survey of the civilian noninstitutionalized population residing in the United States at the time of the interview. NHIS is used to monitor the health of the United States population through the collection and analysis of data on a broad range of health topics. NHIS interviews are completed in person in participants’ homes. The sample design is a probability design that permits the representative sampling of households and noninstitutional group quarters and oversamples Hispanic and Black populations. The sample adult survey component, which includes information on health conditions for adults 18 years old or older, was used in this study. Because these data are publicly available, our study did not require an IRB approval and informed consent.
Study cohort
Our study sample was restricted to participants who were diagnosed with cancer when they were 0 to 39 years old. Cancer survivors were identified using the NHIS question that asked about ever being told by a physician or health professional that she/he had cancer or a malignancy of any kind. Nonmelanoma skin cancer or skin cancer with unknown type were excluded from the analytical sample.
Outcome variable
The outcome variable was psychological distress, measured by the validated Kessler 6 (K6) nonspecific distress scale of six symptoms [18]. Respondents were asked how often they felt the following in the past 30 days: 1) “So sad nothing cheers them up”, 2) “nervous”, 3) “restless/fidgety”, 4) “hopeless”, 5) “everything was an effort”, and 6) “worthless”. The responses were on a 5-point Likert scale which were scored as 0 — “None of the time”, 1 — “A little of the time”, 2 — “Some of the time”, 3 — “Most of the time”, 4 — “All of the time”. Responses were scored and added to produce a range of 0–24. We further categorized the score into three levels based on previous literature with values of 0–4 being classified as mild distress, 5–12 as moderate distress, and ≥ 13 as severe psychological distress [12].
Covariates
Trend analyses were stratified by gender, race/ethnicity, marital status, and visit to mental health professional within past year. Marital status was categorized as “currently married/living with partner”, “widowed/divorced/separated”, and “never married”. Race/Ethnicity was categorized as “non-Hispanic White”, “non-Hispanic Black”, and “Hispanic”. Visit to a mental health professional within past 12 months was classified as “yes” or “no”.
Statistical analyses
Analyses were weighted to account for the complex survey design of the NHIS that reduced bias owing to nonresponse and noncoverage and allowed the results to be generalized to the U.S. adult population. Descriptive statistics using Chi square test were performed to describe the cohort characteristics and stratified by psychological distress. We reported frequency and percentages for all categorical variables. Trends in psychological distress were calculated using joinpoint regression, a variant of log-linear regression [19]. Joinpoint regression models determined the starting and ending years of increases/decreases and then estimated the annual percentage change (APC) and 95% confidence intervals (CI) on the basis of regression model between the 2 joinpoint years [20]. The final joinpoint models were based on log-transformed percentages to better ensure the normality of residuals. The permutation test method determined the model with the fewest number of joinpoints necessary to effectively characterize trends with a maximum of 2 joinpoints selected in this study. Tests for the model selection and significant increases/decreases in APCs were set at alpha = 0.05 and all tests were two-tailed. Joinpoint regression was performed in Joinpoint 4.9.0.1 (National Cancer Institute Statistical Research Applications Branch, Bethesda, MD). Descriptive statistics were conducted by using SAS, version 9.4 (SAS Institute, Inc).
Results
There were 6451 survey respondents in our study between years 2008 and 2018. Overall, 8% of respondents reported experiencing severe distress, and 26% reported moderate distress. Respondents were 43.9% aged 18–44, 71.5% female, 82.3% non-Hispanic White, and 62.5% married or living as married. Approximately 30.9% had a college degree or more, and 85.3% had not seen a mental health professional. Finally, 38.2% resided in the South region of the U.S. (Table 1). Table 1. Sample characteristics overall and stratified by emotional distress, 2008–2018 National Health Interview Survey (n = 6451)**Frequency (weighted percent)P-value****Total (100%)Emotional distressLow/None (66.3%)****Moderate (25.6%)*Severe (8.1%)Age at time of survey <0.0001 18–442634 (43.9)1575 (62.2)761 (28.4)251 (9.4) 45–642441 (38.8)1524 (66.5)637 (25.3)238 (8.2) 65+ 1340 (17.3)993 (76.3)258 (19.0)60 (4.7)Sex <0.0001 Male1677 (28.5)1197 (73.0)354 (21.7)95 (5.3) Female4738 (71.5)2895 (63.7)1302 (27.1)454 (9.3)Race/ethnicity0.1066 Non-Hispanic White5058 (82.3)3295 (67.0)1274 (25.3)400 (7.7) Non-Hispanic Black520 (6.5)299 (63.6)149 (27.0)57 (9.4) Hispanic619 (8.4)363 (61.3)171 (27.1)75 (11.7) Missing218 (2.9)135 (67.9)62 (25.2)17 (6.9)Marital status <0.0001 Married/Living as Married3213 (62.5)2226 (70.7)741 (23.4)199 (5.9) Divorced/Widowed/Separated2151 (23.6)1252 (58.6)596 (28.7)259 (12.7) Never Married1051 (13.9)614 (59.6)319 (29.9)91 (10.6)Education level Less than High School810 (11.6)377 (48.7)258 (32.0)153 (19.3) <0.0001 High School Graduate1463 (23.4)867 (59.8)420 (30.1)150 (10.1) College Graduate or More1850 (30.9)1415 (78.0)354 (18.9)50 (3.1) Some College2274 (33.7)1425 (66.4)615 (26.0)195 (7.6) Missing18 (0.4)8 (34.9)9 (57.4)1 (7.7)Visit mental health professional past 12 months Yes943 (13.5)316 (35.0)403 (43.2)210 (21.9) <0.0001 No5393 (85.3)3753 (71.2)1246 (22.8)336 (6.0) Missing79 (1.2)23 (78.3)7 (16.0)3 (5.6)Geographic region Northeast896 (14.6)589 (68.4)220 (23.8)74 (7.8)0.6971 Midwest1539 (24.4)964 (64.1)402 (26.8)137 (9.1) South2303 (38.2)1471 (66.7)589 (25.5)201 (7.8) West1677 (22.8)1068 (66.6)445 (25.5)137 (7.9)Survey year0.1602 2008444 (9.5)258 (61.3)131 (28.4)48 (10.4) 2009519 (8.6)328 (63.9)141 (27.7)49 (8.5) 2010504 (9.1)329 (67.6)133 (24.7)37 (7.7) 2011591 (8.6)381 (66.1)156 (25.4)52 (8.5) 2012646 (9.0)425 (67.2)165 (25.0)55 (7.8) 2013649 (9.2)392 (64.0)180 (27.9)59 (8.1) 2014715 (9.2)474 (73.2)160 (19.5)62 (7.3) 2015636 (8.8)392 (66.1)152 (23.4)61 (10.5) 2016650 (9.1)422 (67.1)155 (24.8)58 (8.2) 2017562 (9.8)358 (65.1)160 (29.7)32 (5.2) 2018499 (9.1)333 (68.0)123 (24.4)36 (7.6)*p-value <0.05 as test of significance
Overall, the proportion of individuals experiencing mild/no psychological distress increased by 1.68% annually between 2008 and 2014 (APC = 1.68; 95% CI: −0.35 to 3.75) and then decreased by 1.34% annually between 2014 and 2018 (APC = −1.34; 95% CI: −4.77 to 2.21); however, the trends were not statistically significant (Fig. 1, Table 2). In contrast, the proportion of individuals experiencing moderate distress decreased by 3.06% annually between 2008 and 2014 (APC = −3.06; 95% CI: −8.12 to 2.29) and then increased by 4.18% annually between 2014 and 2018 (APC = 4.18; 95% CI: −6.53 to 16.12), and these trends were not statistically significant (Fig. 1, Table 2). The proportion of individuals experiencing severe distress decreased by 1.14% annually between 2008 and 2014 (APC = −1.14; 95% CI: −7.48 to 5.63) and then decreased by 7.36% annually between 2014 and 2018 (APC = −7.36; 95% CI: −28.56 to 20.15); a non-significant trend remained (Fig. 1, Table 2).Fig. 1. Joinpoint analysis of the prevalence of emotional distress among cancer survivors diagnosed at childhood or adolescent and young adult, 2008–2018 National Health Interview Survey. APC, annual percentage change; ^^P-value < 0.05 as test of significance. Data: 2008–2018 National Health Interview SurveyTable 2Annual percentage change (APC) over time in emotional distress, 2008–2018 National Health Interview Survey**YearsAPC**Lower CIUpper CIP***-valueOverall trend** Mild2008–20141.68−0.353.750.090 Mild2014–2018−1.34−4.772.210.386 Moderate2008–2014−3.06−8.122.290.206 Moderate2014–20184.18−6.5316.120.391 Severe2008–2015−1.14−7.485.630.687 Severe2015–2018−7.36−28.5620.150.499SexFemale Mild2008–20106.23−14.8032.460.528 Mild2010–2018−0.20−2.251.890.820 Moderate2008–2014−3.11−9.033.200.267 Moderate2014–20184.04−9.1319.100.501 Severe2008–2010−12.41−58.9887.050.684 Severe2010–20180.50−8.179.980.897Male Mild2008–20141.28−1.353.970.281 Mild2014–2018−1.27−5.202.820.469 Moderate2008–2014−2.64−12.147.890.548 Moderate2014–20184.98−11.4524.470.511 Severe2008–201013.56−68.04303.490.814 Severe2010–2018−8.42−19.434.110.144Race/EthnicityNon-Hispanic White Mild2008–20141.95−0.394.350.088 Mild2014–2018−2.07−6.082.100.265 Moderate2008–2014−3.55−9.582.890.220 Moderate2014–20185.83−7.0320.460.326 Severe2008–20150.18−7.238.170.957 Severe2015–2018−9.79−32.6020.740.420Non-Hispanic Black Mild2008–201113.58−12.3747.220.275 Mild2011–20181.22−3.766.470.577 Moderate2008–2014−8.72−15.83−1.010.033^^ Moderate2014–20184.45−17.4632.180.667 Severe2008–2016−11.80−29.4610.280.218 Severe2016–201819.21−96.043489.780.904Hispanic* Mild2008–20124.99−7.6319.340.388 Mild2012–2018−2.51−9.675.230.447 Moderate2008–201013.11−44.57130.780.687 Moderate2010–2018−0.16−7.497.760.961 Severe2008–2010−32.82−88.68298.770.604 Severe2010–20182.13−17.9827.170.822Marital statusMarried Mild2008–20142.26−0.4717.380.058 Mild2014–2018−3.26−15.280.780.068 Moderate2008–2014−4.19−10.122.140.153 Moderate2014–20187.34−5.8322.340.234 Severe2008–2014−4.12−17.1410.950.507 Severe2014–20184.60−20.0736.880.697Divorced/Separated Mild2008–20150.48−4.675.910.831 Mild2015–20182.43−12.7720.270.727 Moderate2008–20130.30−15.2718.730.967 Moderate2013–2018−4.65−19.4912.910.516 Severe2008–20162.14−8.7214.290.661 Severe2016–2018−18.30−75.14168.540.692Never Married Mild2008–201012.56−25.4069.830.508 Mild2010–20180.57−2.733.980.691 Moderate2008–2010−15.51−54.5457.020.530 Moderate2010–20182.83−3.839.950.347 Severe2008–2014−2.50−24.1025.250.813 Severe2014–2018−29.76−63.9136.720.242Visit mental health professional past 12 months**Yes Mild2008–2016−1.06−9.287.900.774 Mild2016–201815.68−41.23127.720.618 Moderate2008–2010−3.84−44.6266.990.868 Moderate2010–20181.32−4.207.170.588 Severe2008–20150.47−10.5012.780.925 Severe2015–2018−10.58−42.1738.250.553No Mild2008–20141.780.777.000.013* Mild2014–2018−1.52−6.430.280.108 Moderate2008–2015−3.26−8.041.760.160 Moderate2015–20187.52−10.3829.000.367 Severe2008–2010−12.92−58.3882.180.663 Severe2010–2018−1.27−9.297.470.726
When stratified by sex, there was no statistically significant difference in trends in the proportion of individuals experiencing severe, moderate, or mild/no distress among both females and males CAYA survivors (Fig. 2A, B, Table 2). There was no statistically significant difference in trends in the proportion of individuals experiencing severe, moderate, or mild/no distress for non-Hispanic Whites and Hispanics over the 10-year period (Fig. 3A, C, Table 2). However, for non-Hispanic Blacks, the proportion of individuals experiencing moderate distress significantly decreased by 8.72% annually between 2008 and 2014 (APC = −8.72; 95% CI: −15.83 to −1.01, P = 0.033) and then increased by 4.45% annually between 2014 and 2018, although not statistically significant (Fig. 3B, Table 2). There was no statistically significant difference in trends in the proportion of individuals experiencing severe, moderate, or mild/no distress irrespective of the marital status of the respondent (Supplemental Fig. 1A-C, Table 2). There was no statistically significant difference in trends in the proportion of individuals experiencing severe, moderate, or mild/no distress among respondents who visited or did not visit a mental health professional in the past 12 months (Supplemental Fig. 2A-B, Table 2).Fig. 2. Joinpoint analysis of the prevalence of emotional distress among a) male and b) female cancer survivors diagnosed at childhood or adolescent and young adult, 2008–2018 National Health Interview Survey. APC, annual percentage change; ^^P-value < 0.05 as test of significance. Data: 2008–2018 National Health Interview SurveyFig. 3Joinpoint analysis of the prevalence of emotional distress among a) Non-Hispanic White, b) Non-Hispanic Black, and c) Hispanic cancer survivors diagnosed at childhood or adolescent and young adult, 2008–2018 National Health Interview Survey. APC, annual percentage change; ^^P-value < 0.05 as test of significance. Data: 2008–2018 National Health Interview Survey
Discussion
Our study aimed to assess trends in emotional distress among the CAYA cancer survivors. To our knowledge, this is the first study investigating trends in emotional distress over time among survivors of CAYA cancers. Our results reported that overall trends in emotional distress have not changed significantly over the 2008–2018 decade. When stratified by gender, race/ethnicity, marital status, and visit to mental health professional within the past year, we did not observe any significant changes in the trend of emotional distress except in non-Hispanic Blacks. Non-Hispanic Blacks experiencing moderate distress had a significantly decreased trend between 2008 and 2014. Though traditionally, non-Hispanic Blacks report lower mental health due to protective factors like strong social support, religious hope, and unique cultural coping mechanisms; it is difficult to explain this finding as we could not access changes in those factors in the same timeframe. Future studies should examine trends in protective factors and mental health to help explain this relationship. If distress levels remain unchanged, there may be serious long-term implications on the quality of life and healthcare outcomes of survivors. Persistent emotional distress is associated with poor adherence to treatment, worse overall outcomes, and significant financial burdens [21], all of which highlight the need for support for this population.
Although not statistically significant, our analyses revealed a slight increase in moderate emotional distress but a slight decrease in mild emotional distress from 2014 to 2018. The proportion of CAYA cancer survivors with severe distress was relatively stable through the study period. While our findings did not report a significant increase in distress over time, the consistency of moderate and severe distress levels over the years suggests that emotional/psychological distress remains an unresolved issue for many CAYA survivors, consistent with literature suggesting that higher levels of emotional distress among cancer survivors compared to the general population [12, 22]. Evidence indicates that a history of mental illness is associated with poorer outcomes [21], which could explain some of the persistent distress observed in our data. Other potential explanations could be the long-term psychosocial impacts of cancer treatment or the growing stigma of mental health challenges in recent years and navigating adult responsibilities while coping with the long-term effects of cancer may also contribute to sustained distress among survivors [23, 24]. The challenges of employment, education, and relationships are further complicated for survivors diagnosed as AYAs, underscoring the importance of specialized support services [25]. This situation is compounded by the lack of treatment protocols specifically designed for survivors diagnosed as children or AYAs and the limited availability of clinical trials focused on this age group [26]. Our findings highlight the persistent psychological burden faced by cancer survivors, emphasizing the need for continued screening and support, regardless of emotional distress severity.
Our analysis of emotional distress trends stratified by gender, race/ethnicity, marital status, and visit to mental health professionals was not statistically significant. This finding indicates that psychological distress is a universal challenge among cancer survivors, transcending gender, race/ethnicity, and even access to mental health professionals. The trend among these groups has not changed significantly over the years, suggesting that emotional distress remains a consistent issue across all demographics. This finding diverges from prior cross-sectional studies that have consistently shown greater emotional distress among female survivors, as well as elevated distress among ethnic minorities and individuals with limited access to mental health services [27–29]. For example, cross-sectional studies have shown that women, particularly adolescent females, tend to experience higher rates of depression and anxiety compared to their male counterparts, which reemphasizes the complexity of CAYA cancer survivor subgroup needs [30, 31]. Social and psychological stressors such as infertility and the long-term sequelae of cancer treatment may exacerbate these issues among female survivors [32, 33]. This could indicate that current interventions are not sufficiently tailored to address the complex needs of CAYA survivor subgroups [30].
Interestingly, despite an increase in visits to mental health professionals, trends in emotional distress levels among CAYA survivors remained stable. A possible explanation for this could be the persistent stigma surrounding mental health, particularly in the previous two decades. Research indicates that while attitudes toward mental health have improved over the years, stigma still lingers, especially in certain populations, which might prevent survivors from fully benefiting from mental health services [24, 34]. This finding suggests that even though mental health services are being accessed, current approaches may not be sufficient to address emotional distress in CAYA survivors. These unmet needs may contribute to persistently heightened emotional distress, as suggested by previous literature [31]. Pre-existing mental health conditions, which were not captured in our data, may also play a role.
Limitations
Our findings should be interpreted in the context of several limitations. First, the use of self-reported data regarding emotional distress introduces the potential for recall and social desirability biases. Additionally, a small sample size limited the examination of trends in emotional distress by cancer type to assess if distress differed by cancer a survivor was diagnosed with. Lastly, due to the cross-sectional design, we fail to comment on the causal association of the study.
Conclusion
Our study provides a novel examination of emotional distress trends among CAYA cancer survivors over a decade. While overall distress levels have remained relatively stable, the consistent presence of moderate and severe distress underscores the need for continued mental health support and tailored interventions. Understanding the nuanced needs of this survivor population and its subgroups is critical in improving their quality of life and long-term outcomes.
Supplementary Information
Below is the link to the electronic supplementary material. ESM 1Supplementary Material 1 (PNG 99.4 KB)High Resolution Image (TIFF 94.4 KB)ESM 2Supplementary Material 2 (PNG 111 KB)High Resolution Image (TIFF 100 KB)ESM 3Supplementary Material 3 (PNG 109 KB)High Resolution Image (TIFF 103 KB)ESM 4Supplementary Material 4 (PNG 99.1 KB)High Resolution Image (TIFF 95.4 KB)ESM 5Supplementary Material 5 (PNG 100 KB)High Resolution Image (TIFF 95.0 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1U.S. Centers for Disease Control and Prevention. National Health Interview Survey. Accessed January 11, 2024. https://www.cdc.gov/nchs/nhis/index.html
- 2Surveillance Research Program , National Cancer Institute (2024) Joinpoint Regression Software. Version 5.0.2. 2024. https://surveillance.cancer.gov/joinpoint