Efficacy of probiotic supplementation in preventing Clostridioides difficile infection: an umbrella review of systematic reviews and meta-analysis
Wenci Chen, Xianjuan Pan, Jing Ji, Zhenhua Wu, Xinxin Lin

TL;DR
This study reviews evidence that probiotics can reduce the risk of Clostridioides difficile infection, but the quality of evidence varies.
Contribution
This umbrella review synthesizes multiple meta-analyses to evaluate the overall efficacy of probiotics in preventing CDI.
Findings
Probiotics significantly reduced CDI risk with a pooled relative risk of 0.37.
Multi-strain probiotics and those containing Saccharomyces boulardii showed significant benefits.
The quality of evidence ranged from moderate to low, with minimal overlap among primary studies.
Abstract
Clostridioides difficile infection (CDI) is a significant healthcare-associated infection. Probiotics have been proposed as a preventive strategy. This umbrella review synthesizes evidence from meta-analyses on the efficacy of probiotics in preventing CDI. A comprehensive systematic search was conducted in PubMed, Scopus, Web of Science, Embase, and the Cochrane Library up to December 2025. To manage overlap, a single primary systematic review was selected per outcome. The methodological quality of included reviews was assessed using AMSTAR-2, and the certainty of evidence was graded. Pooled effect sizes were calculated using a random-effects model. Sixteen systematic reviews and meta-analyses were included. The pooled relative risk (RR) from primary reviews indicated that probiotics significantly reduced CDI risk (RR = 0.37; 95% CI: 0.32 to 0.42; I2 = 0%). Multi-strain probiotics and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
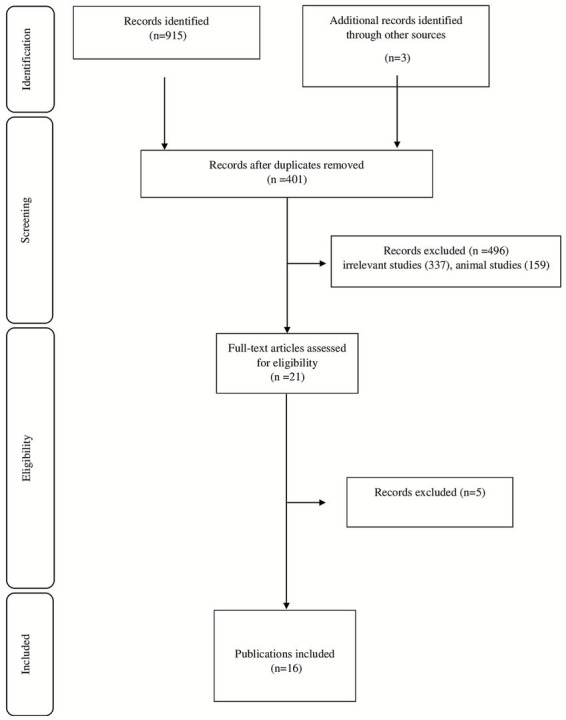 Figure 1
Figure 1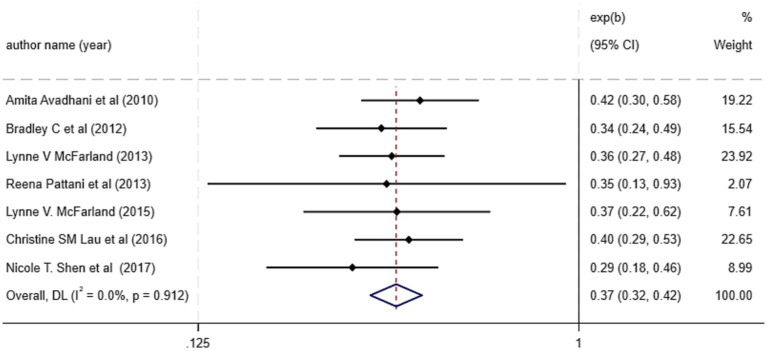 Figure 2
Figure 2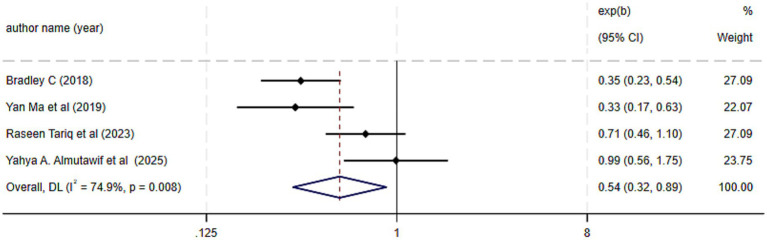 Figure 3
Figure 3| Citation (First author et al., year) | No. of studies in meta-analysis | Location | No. of participants in meta-analysis | Intervention | Quality assessment scale and outcome |
|---|---|---|---|---|---|
| Avadhani A et al. 2010 | 4 | Australia | 471 | Yes (JBI’s assessment) | |
| Johnston BC et al. 2012 | 20 | Canada | 3,818 |
| Yes (Cochrane) 5/20 low quality |
| Salari P et al. 2012 | 19 | Iran | 3,867 |
| Yes (Jadad score) 3/19 low quality |
| Pattani R et al. 2013 | 9 | Canada | 1,107 |
| Yes (Cochrane) 4/9 low quality |
| McFarland VL et al. 2013 | 5 | US | 1,211 |
| Yes (Cochrane) 4/5 low quality |
| McFarland VL et al. 2015 | 23 | US | 4,476 |
| Yes (Cochrane) 3/24 low quality |
| Lau CSM et al. 2016 | 26 | US | 7,957 |
| Yes (Cochrane) 2/26 low quality |
| Shen NT et al. 2017 | 18 | US | 6,139 |
| Yes (Cochrane) 10/18 low quality |
| Vernaya M et al. 2017 | 5 | US | 3,461 |
| Yes (Cochrane) 0/5 low quality |
| Johnston BC et al. 2018 | 13 | Canada | 5,074 | Saccharomyces. Lactobacillus. Bifid bacterium. Streptococcus | Yes (Cochrane) 7/13 low quality |
| Ma Y et al. 2019 | 11 | China | 4,523 | Saccharomyces. Lactobacillus. Bifid bacterium. Streptococcus | Yes (Cochrane) 2/11 low quality |
| Goodman C et al. 2021 | 42 | Australia | 11,305 | Saccharomyces. Lactobacillus. Bifid bacterium. Streptococcus | Yes (Cochrane) 5/42 high quality |
| Raseen Tariq et al. 2023 | 6 | US | 1,049 |
| Yes (Cochrane) 2/6 high |
| Dabrowski V et al. 2023 | 10 | Ireland | 5,146 |
| Not included in meta-analysis |
| Almutawif YA et al. 2025 | 4 | Saudi Arabia | 9,226 |
| Yes (Cochrane) 1/4 low quality |
| Wanyama H et al. 2025 | 15 | United Kingdom | 7,427 |
| Yes (Cochrane) 3/15 low quality |
| Study (Author, Year) | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 | Overall confidence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Almutawif YA et al. 0.2025 | Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | No | Yes | Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Yes | Critically low |
| Avadhani A et al. 2010 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | Partial Yes | No | Partial Yes | No | No | No | Partial Yes | No | Critically low |
| Dabrowski V et al. 2023 | Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | No | Yes | Yes | No | Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Yes | Critically low |
| Goodman C et al. 2021 | Yes | Partial Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Moderate |
| Johnston BC et al. 2018 | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Critically low |
| Johnston BC et al. 2012 | Yes | No | Yes | Yes | Partial Yes | Partial Yes | No | Yes | Yes | No | Yes | Partial Yes | Partial Yes | Yes | Partial Yes | Yes | Critically low |
| Lau CSM et al. 2016 | Yes | No | Partial Yes | Partial Yes | No | No | No | Partial Yes | Partial Yes | No | Partial Yes | No | No | Partial Yes | Partial Yes | No | Critically low |
| Ma Y et al. 2019 | Yes | Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| McFarland VL et al. 2015 | Yes | No | Yes | Partial Yes | Partial Yes | Partial Yes | No | Yes | Partial Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Yes | Critically low |
| McFarland VL et al. 2013 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | No | No | No | No | No | No | No | No | Critically low |
| Pattani R et al. 2013 | Yes | No | Partial Yes | Partial Yes | No | No | No | Partial Yes | Partial Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | No | Critically low |
| Salari P et al. 2012 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | No | No | No | No | No | No | No | No | Critically low |
| Shen NT et al. 2017 | Yes | No | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Tariq R et al. 2023 | Yes | Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Vernaya M et al. 2017 | Yes | No | Partial Yes | Partial Yes | No | No | No | Partial Yes | Partial Yes | No | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | No | Critically low |
| Wanyama H et al. 2025 | Yes | Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Outcomes | Subgroups | Studies | Test of effect | Test of heterogeneity | |
|---|---|---|---|---|---|
| ES (95%CI) | I2 (%) |
| |||
| CDI prevention | Overall | 7 | 0.37 (0.32, 0.42) | 0.0 | 0.912 |
| Type of strains | S, L, B, St | 3 | 0.35 (0.29, 0.44) | 0.0 | 0.679 |
| S, L, B | 3 | 0.38 (0.31, 0.47) | 0.0 | 0.774 | |
| S, L, St | 1 | 0.35 (0.13, 0.93) | - | - | |
| Sample size | ≥ 5,000 participants | 2 | 0.36 (0.27, 0.47) | 16.2 | 0.275 |
| <5,000 participants | 5 | 0.37 (0.31, 0.44) | 0.0 | 0.930 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Probiotics and Fermented Foods · Gastrointestinal motility and disorders
Introduction
1
Clostridioides difficile infection (CDI) is a common healthcare-associated challenge, primarily linked to antibiotic use (1, 2). It frequently manifests as diarrhea in hospitalized patients (3). Antibiotic treatment disrupts the gut microbiota, facilitating the development of CDI (4). Evidence indicates that CDI is associated with a wide range of health consequences, including severe diarrhea and systemic infection (5). It is a multifaceted disorder with broad clinical and socio-economic impacts (6), posing an economic burden through prolonged hospitalization, reduced quality of life, and increased healthcare costs (6). The rising incidence of CDI highlights the urgent need for effective preventive strategies to reduce infection rates and improve patient outcomes.
Probiotics have gained attention for their role in regulating gut microbiota (7, 8). The World Health Organization (WHO) defines probiotics as live microorganisms that confer health benefits when administered in adequate amounts (9, 10). Probiotics are thought to compete with pathogens, helping to maintain gut microbiota balance, promote gut barrier function, preserve intestinal integrity, and modulate immune responses (11, 12). Consequently, several meta-analyses have investigated the effectiveness of probiotics in preventing CDI.
Despite promising findings, some studies have reported no significant effect of probiotics on CDI prevention. These inconsistencies may stem from variations in probiotic strain, dosage, and patient population, which can influence the risk of diarrhea and CDI. Therefore, evaluating the effect of probiotics on CDI prevention using both risk ratios (RR) and odds ratios (OR) in a strain-specific manner is crucial. This underscores the importance of synthesizing the available evidence to clarify the efficacy of probiotic supplementation in preventing CDI.
Methods
2
This umbrella review of systematic reviews and meta-analyses was conducted in accordance with the PRISMA 2020 guidelines (13). The study protocol was registered in PROSPERO (ID CRD420251062730).
Search strategy
2.1
A comprehensive systematic search was conducted in PubMed, Scopus, Web of Science, Embase, and the Cochrane Library from database inception through December 2025. Reference lists of relevant studies were also screened to identify additional articles. The search strategy was developed using a combination of MeSH terms and keywords (Supplementary Table 1). Moreover, the search was restricted to articles published in the English language.
Inclusion and exclusion criteria
2.2
This study integrated the systematics reviews and meta-analyses investigating the impact of probiotics in prevention of CDI, specifically those that provided effect sizes (ESs) along with their respective confidence intervals (CIs). The PICO criteria for this umbrella meta-analysis were defined as follows: population: individuals of all ages, both below and above 18 years receiving probiotic treatment; intervention: administration of probiotics; comparison: a control or placebo group; and outcome: prevention of CDI. The CDI outcome definition and diagnostic timeframe (e.g., during antibiotic therapy or within 4–8 weeks’ post-therapy) were accepted as defined by each included systematic review. In vitro, in vivo, ex vivo studies, case reports, observational studies, and quasi-experimental studies were excluded.
Methodological quality assessment, overlap, and grading of the evidence
2.3
The Measurement Tool to Assess Systematic Reviews (AMSTAR)2 questionnaire was used to qualify the included studies by two independent researchers (14), which consists of 16 items rated as “yes,” “no,” or “not applicable.” Any disagreement was resolved via discussing with third investigator. To address overlap of primary studies across included systematic reviews, the Corrected Covered Area (CCA) was calculated. For outcomes reported by multiple reviews, a single primary systematic review was selected for synthesis based on pre-specified criteria: 1) highest AMSTAR-2 confidence rating, 2) most recent publication date, and 3) largest number of included primary trials. Sensitivity analyses were conducted by sequentially excluding non-primary reviews to assess the robustness of the umbrella review estimates. The overall certainty of evidence for the main outcome (CDI prevention) was evaluated using the GRADE approach, considering the quality of the included reviews and the underlying primary studies. The quality of evidence was categorized into four categories based on evaluation criteria, i.e., high, moderate, low, and very low (15).
Study selection and data extraction
2.4
The screening process was completed by two independent reviewers in accordance with the predefined eligibility criteria. Initially, the titles and abstracts of the articles were evaluated. Subsequently, the full-texts of the eligible articles were evaluated to determine their eligibility for inclusion in the current umbrella meta-analysis. The extracted data included the name of the first author, year of publication, the geographical location, number of included studies in each meta-analysis, total sample sizes and ESs and CIs of outcomes.
Data synthesis and statistical analysis
2.5
The pooled ES and its associated 95% CI were estimated using random-effects models performed using restricted maximum likelihood (REML) model (16). ESs are reported as RR or OR with 95% CI. The I^2^ index was used to evaluate the heterogeneity within the meta-analysis and a significant level of heterogeneity in the data was established when I^2^ exceeded 50% (16). Pre-planned subgroup analyses were conducted for clinically relevant strata: probiotic type (e.g., Saccharomyces boulardii, Lactobacillus-based, multi-strain), sample size, and age group (adult, pediatric). Where sufficient data were available, pooled estimates were calculated for each subgroup using a random-effects model, and tests for subgroup differences were performed. A sensitivity analysis was performed to evaluate the impact of excluding a specific study on the overall ES. All statistical analyses were conducted using STATA version 16.0 (Stata Corporation, College Station, TX, US). A p-value of less than 0.05 was considered significant.
Results
3
Study selection and study characteristics
3.1
There were 918 records found in the database search. 401 duplicate studies were eliminated, leaving 517 distinct studies for screening. After 496 of these were disqualified on the basis of abstract and title review, 21 articles remained for full-text assessment. A thorough evaluation led to the exclusion of five studies. 16 studies ultimately met the predetermined inclusion criteria. Figure 1 shows the selection procedure for the study. In the present review, a total of 16 systematic reviews were included (Table 1) (17–32). The CCA score was 15%, indicating “slight” overlap. For the primary outcome of CDI prevention based on RR, the review by Johnston et al. (2012) was selected as the primary synthesis due to its comprehensive scope and methodological rigor. All these studies were published between 2005 up to 2025. The most used probiotics were Saccharomyces, Lactobacillus, Bifid bacterium, Streptococcus Clostridium and mix of probiotics.
PRISMA flow diagram.
Quality assessment and certainty of evidence
3.2
The methodological quality of the included reviews, assessed using AMSTAR-2, is detailed in Table 2. Eleven of the 16 reviews were rated as having “critically low” overall confidence, primarily due to shortcomings in protocol registration, risk of bias assessment, and reporting of excluded studies (17–19, 21–23, 25–28, 31). Using the GRADE framework, the overall certainty of evidence for the efficacy of probiotics in preventing CDI was assessed as low, downgraded due to the methodological limitations of the included reviews and the indirectness introduced by pooling diverse probiotic strains and populations.
Probiotics supplementation in prevention of CDI based on relative risk analysis
3.3
The primary pooled estimate, derived from seven meta-analyses reporting RR, indicated that probiotic supplementation significantly reduced the risk of CDI by 63% (RR = 0.37; 95% CI: 0.32 to 0.42; p < 0.001) with no statistical heterogeneity (I^2^ = 0%) (Figure 2). Our subgroup analysis showed that, probiotics are effective in preventing CDI in studies less than 5,000 participants. Significant reductions in CDI risk were observed for Saccharomyces boulardii (RR = 0.38; 95% CI: 0.27 to 0.53; 3 reviews) and multi-strain formulations (RR = 0.34; 95% CI: 0.24 to 0.49; 4 reviews). The test for subgroup differences between single-strain and multi-strain probiotics was not significant (Table 3). Moreover, sensitivity analysis indicated that exclusion of any single study did not affect the overall pooled effect size (Supplementary Figure 1). Furthermore, Bag’s test revealed no evidence of publication bias (p = 0.999).
Effect size and 95% CIs presented in forest plot of the studies on the probiotics supplementation in CDI prevention based on RR analysis. Weights are from random-effects model.
Probiotics supplementation in prevention of CDI based on odds ratio analysis
3.4
The pooled effect size of four meta-analyses, revealed that probiotic intervention significantly reduced the odds of CDI prevention by 46% compared to the control group (OR = 0.54; 95% CI: 0.32 to 0.89, p = 0.001), with substantial heterogeneity (I^2^ = 74.9%, P-heterogeneity = 0.008) (Figure 3). This finding complements the RR analysis but must be interpreted within the context of this heterogeneity. Sensitivity analysis indicated that the overall effect size was robust, with no single study exerting influence (Supplementary Figure 2). Furthermore, no evidence for publication bias was seen based on Bag’s tests (p = 0.343).
Effect size and 95% CIs presented in forest plot of the studies on the probiotics supplementation in CDI prevention based on OR analysis. Weights are from random-effects model.
Probiotic supplementation on CDI-associated diarrhea
3.5
The evidence for CDI-associated diarrhea was mixed. One meta-analysis found no significant effect of Bifid bacterium, Lactobacillus, and Saccharomyces supplementation in elderly patients (OR = 0.66; 95% CI: 0.26 to 1.66) (31). However, another meta-analysis reported that mixed probiotic formulations reduced the incidence of CDI-associated diarrhea by approximately 40% in adult patients (RR = 0.60; 95% CI: 0.43 to 0.83) (32). A meta-analysis similarly demonstrated a significant reduction in acute diarrhea following probiotic supplementation (WMD = −0.65; 95% CI: −0.94 to −0.38) (28). The probiotic Lactobacillus was associated with a 75% reduction in the risk of CDI-associated diarrhea compared with placebo (RR = 0.25; 95% CI: 0.08 to 0.47) (33).
Safety and adverse events
3.6
Twelve of the sixteen included reviews reported on safety. The most commonly reported adverse events were mild gastrointestinal symptoms (e.g., bloating, flatulence). None of the reviews found a statistically significant increase in serious adverse events attributable to probiotic supplementation compared to placebo or control.
Discussion
4
This umbrella review synthesizes evidence from systematic reviews and meta-analyses on the efficacy of probiotics in preventing CDI. Our primary analysis demonstrates a significant reduction in CDI risk following probiotic supplementation (RR = 0.37). The absence of statistical heterogeneity (I^2^ = 0%) suggests a consistent effect across the included reviews and diverse populations. These findings suggest that probiotics may be considered as effective strategy to prevent the risk of CDI specifically in high-risk population such as hospitalized patients. Probiotics are more potent to restore the gut microbiota balance which may contribute to the CDI (34, 35). Also, they are effective in strengthening intestinal barrier integrity (12), and modulating immune responses (36–38). While most previous meta-analyses align with our pooled result, one review by Dabrowski et al. reported no significant benefit for patients exposed to antibiotics (19, 39, 40).
Subgroup analyses provided further insight. Strain-specific analyses indicated that multi-strain probiotics and those containing Saccharomyces boulardii had pronounced effects. This highlights the importance of probiotic composition. Synergistic effects may arise from the combined actions of different strains: Saccharomyces is noted for immunomodulation, Lactobacillus for restoring microbial balance (41, 42), and Bifid bacterium for supporting barrier function (43). Furthermore, the beneficial effect was consistent across studies of varying sample sizes, supporting the generalizability of the findings. Similarly, our meta-review demonstrated probiotics reduce the odds of CDI as evidenced by OR. This finding complements the abovementioned RR results and can be recommended in clinical setting for CDI prevention reliably.
This umbrella review has several strengths, including a comprehensive search, formal assessment of overlap, and dual appraisal of methodological quality (AMSTAR-2) and evidence certainty (GRADE). The consistent effect across metrics (RR and OR) and low heterogeneity for the primary RR analysis suggest a robust signal. Furthermore, the beneficial effects of probiotics were observed across studies of varying sample sizes, which may support the generalizability of the findings. However, significant limitations must be acknowledged. The majority of included systematic reviews were of critically low methodological quality, which indirectly lowers confidence in our umbrella review estimates. The low GRADE certainty rating further tempers the strength of any conclusions. We were unable to perform robust quantitative analyses for all pre-specified clinical strata (e.g., specific dosage, patient sub-populations) due to inconsistent reporting in the source reviews. Therefore, the findings should be interpreted with caution.
Conclusion
5
This umbrella review of systematic reviews and meta-analyses suggests that probiotic supplementation may be associated with a reduced risk of CDI, as indicated by both RR and OR estimates. The most consistent evidence supports the use of Saccharomyces boulardii and multi-strain formulations. However, due to the predominantly low methodological quality of the underlying systematic reviews, these conclusions should be interpreted with caution. High-quality, sufficiently powered primary trials and subsequent rigorous systematic reviews are needed to establish reliable, strain-specific, and dose-specific recommendations for clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Finn E Andersson FL Madin-Warburton M. Burden of Clostridioides difficile infection (CDI)-a systematic review of the epidemiology of primary and recurrent CDI. BMC Infect Dis. (2021) 21:456. doi: 10.1186/s 12879-021-06147-y, 34016040 PMC 8135979 · doi ↗ · pubmed ↗
- 2Webb BJ Subramanian A Lopansri B Goodman B Jones PB Ferraro J . Antibiotic exposure and risk for hospital-associated Clostridioides difficile infection. Antimicrob Agents Chemother. (2020) 64:19. doi: 10.1128/AAC.02169-19PMC 717931431964789 · doi ↗ · pubmed ↗
- 3Zhou F Wu S Klena JD Huang HH. Clinical characteristics of Clostridium difficile infection in hospitalized patients with antibiotic-associated diarrhea in a university hospital in China. Eur J Clin Microbiol Infect Dis. (2014) 33:1773–9. doi: 10.1007/s 10096-014-2132-9, 24820293 PMC 4674785 · doi ↗ · pubmed ↗
- 4Kim B Kim J Pai H. Association between antibiotic consumption and incidence of Clostridioides difficile infection in a hospital. J Korean Med Sci. (2020) 35:e 407. doi: 10.3346/jkms.2020.35.e 407, 33289370 PMC 7721558 · doi ↗ · pubmed ↗
- 5Feuerstadt P Theriault N Tillotson G. The burden of CDI in the United States: a multifactorial challenge. BMC Infect Dis. (2023) 23:132. doi: 10.1186/s 12879-023-08096-0, 36882700 PMC 9990004 · doi ↗ · pubmed ↗
- 6Song X Song W Cui L Duong TQ Pandy R Liu H . A comprehensive review of the global epidemiology, clinical management, socio-economic impacts, and national responses to long COVID with future research directions. Diagnostics. (2024) 14:1168. doi: 10.3390/diagnostics 14111168, 38893693 PMC 11171614 · doi ↗ · pubmed ↗
- 7Sánchez B Delgado S Blanco-Míguez A Lourenço A Gueimonde M Margolles A. Probiotics, gut microbiota, and their influence on host health and disease. Mol Nutr Food Res. (2017) 61:1600240. doi: 10.1002/mnfr.20160024027500859 · doi ↗ · pubmed ↗
- 8Musazadeh V Mohammadi Anilou M Vajdi M Karimi A Sedgh Ahrabi S Dehghan P. Effects of synbiotics supplementation on anthropometric and lipid profile parameters: finding from an umbrella meta-analysis. Frontiers in nutrition, (2023) 10:1121541. doi: 10.3389/fnut.2023.112154136908920 PMC 9995782 · doi ↗ · pubmed ↗