Novel use of anifrolumab in a young patient with Jo-1-positive juvenile dermatomyositis
Daniel Windschall, Tanja Hinze, Sven Hardt, Duygu Aydin, Faekah Gohar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
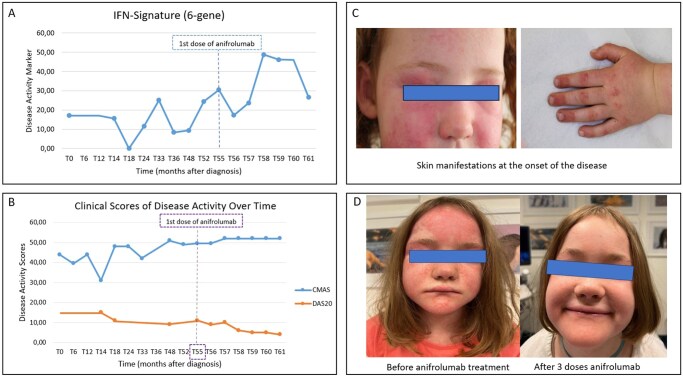 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Myopathies and Dermatomyositis · Spondyloarthritis Studies and Treatments · Infectious Diseases and Tuberculosis
Dear Editor, Anifrolumab is a monoclonal antibody targeting subunit 1 of the type 1 interferon (IFN) receptor. Experience with anifrolumab in patients with JDM is limited to predominantly adult or adolescent patients treated with a higher dose (300 mg/month) for skin and muscle disease, without calcinosis cutis and without longitudinal IFN signature assessments reported [1–3]. Two patients with anti-transcription intermediary factor 1γ–positive JDM and rapid response to anifrolumab were published in June 2025 [4]. Anifrolumab is currently approved for the treatment of SLE in adults and a study of anifrolumab in paediatric SLE is currently under way.
This case report describes the changes in disease activity and expression of type 1 IFN-stimulated genes in whole blood over 7 months with off-label use of anifrolumab (150 mg/month) in an 8-year-old girl with refractory skin involvement combined with severe calcinosis cutis.
Jo-1-positive JDM was first diagnosed at the age of 4 years, with Gottron’s papules, skin erythema (Fig. 1C) and MRI-confirmed myositis present. The initial treatment included methylprednisolone pulse therapy, oral prednisolone and methotrexate. Six months later, hydroxychloroquine was added. The treatment was ineffective, leading to an increased oral prednisolone dose after 12 months of therapy. Off-label tofacitinib, initiated 16 months after diagnosis, with a starting dose of 3.75 mg twice daily, followed by an increase to 4 mg twice daily after 14 months of treatment, significantly improved myositis [Childhood Myositis Assessment Scale (CMAS): 37–51 (maximum 52)] and the 20-item DAS [DAS20: 15 to 9 (worst 20)]. Minimal change in the IFN signature (median of the whole blood expression of six type 1 IFN-stimulated genes measured by real-time PCR: IFI27, IFI44L, IFIT1, ISG15, RSAD2, SIGLEC1; normal <6.0, moderate activity 20.1—50.0) occurred (15.6 to 9.4). Skin involvement remained refractory and calcinosis cutis developed 3.5 years after first presentation. The addition of immunoglobulin therapy and switching from tofacitinib to baricitinib, administered at a dose of 2 mg once daily, and increased to 3 mg once daily 2 months later, resulted in a worsening of disease activity (DAS20 = 11) and increasing of the IFN signature to 30.5, measured 4 months after the start of baricitinib treatment. For this reason, treatment with baricitinib was ended.
Off-label anifrolumab (150 mg/month) was started 4.5 years after the initial diagnosis. Methotrexate (12.5 mg once weekly) and oral prednisolone (3 mg once daily during the first 2 months of treatment and reduced gradually over the following months with a dose of 1 mg every second day after 6 months of treatment with anifrolumab) were continued. All the medications used throughout the course of the disease, including the oral prednisolone dose, are shown in Supplementary Fig. S1. Disease activity improved after a single dose of anifrolumab (DAS20 = 9) and the IFN signature decreased to 17.3 (Fig. 1A, 1B and Supplementary Table S1). The IFN signature values and the values of the individual IFN-regulated genes throughout the course of the disease are shown in Supplementary Table S1. Before the fifth dose, DAS20 improved further to 5 (Fig. 1B). At this time, the vasculitic skin lesions, Gottron’s papules and skin erythema were no longer present and only minimal nailfold erythema remained (Fig. 1D). Furthermore, there were no signs of ongoing myositis and the CMAS remained stable at the highest possible value of 52. No new calcinosis cutis lesions developed, while existing lesions appeared to be healing after spontaneous draining. The IFN signature remained moderately elevated (25.7) after the sixth dose of anifrolumab (Fig. 1A and Supplementary Table S1).
No safety or adverse events were reported and no infections occurred over 7 months of treatment.
In conclusion, skin involvement of JDM rapidly improved in this young patient with refractory disease after just two doses of anifrolumab (150 mg/dose). The IFN signature remained moderately elevated after six doses despite clinical improvement. Calcinosis cutis remained stable. No safety or adverse events occurred.
This case illustrates the potential for anifrolumab to provide additive value to existing treatment strategies, including the use of newer Janus kinase inhibitors, to improve the future treatment of refractory JDM.
Larger prospective studies are required to confirm efficacy and safety in the paediatric population. In addition, longer-term follow-up is required for this promising therapy for JDM to determine the effect of anifrolumab on the course of calcinosis cutis lesions and association with IFN signature.
Supplementary Material
rkag017_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shayegan LH , Shaw KS, Wieschhoff GG et al Improvement in dermatomyositis-associated muscle disease with anifrolumab. Br J Dermatol 2025;192:1126–8. doi: 10.1093/bjd/ljaf 06440036364 PMC 12107708 · doi ↗ · pubmed ↗
- 2Barrutia-Etxebarria A , Escribano De La Torre RM, Lopez Martinez J et al Anifrolumab in refractory juvenile dermatomyositis. Pediatr Dermatol 2026;43:116–20. doi: 10.1111/pde.1601240671636 · doi ↗ · pubmed ↗
- 3Shaw KS , Reusch DB, Castillo RL et al Rapid improvement in recalcitrant cutaneous juvenile dermatomyositis with anifrolumab treatment. JAMA Dermatol 2024;160:237–8. doi: 10.1001/jamadermatol.2023.474437950917 · doi ↗ · pubmed ↗
- 4Triaille C , Piram M, Ellezam B et al Rapid clinical and transcriptomic response to anifrolumab in refractory anti-TIF 1γ-positive juvenile dermatomyositis. Ann Rheum Dis 2025;84:1052–4. doi: 10.1016/j.ard.2025.02.00240221262 · doi ↗ · pubmed ↗