Premature Coronary Artery Disease and Familial Dyslipidemia in Patients Presenting With Acute Coronary Syndrome: A Tertiary Cardiac Center Registry
Mohamed Saad, Mohammad Alshehri, Amr Elgazzar, Mohamed Senara, Hesham S Taha

TL;DR
This study finds that premature coronary artery disease in patients with heart attacks is strongly linked to smoking and family history of high cholesterol, not diabetes or high blood pressure.
Contribution
The study identifies smoking and familial dyslipidemia as key predictors of premature coronary artery disease in acute coronary syndrome patients.
Findings
Premature CAD patients were younger, more likely male, and had higher cholesterol and LDL levels.
Smoking and family history of dyslipidemia were the strongest independent predictors of premature CAD.
Diabetes and hypertension were less common in premature CAD cases compared to non-premature cases.
Abstract
Background: Premature coronary artery disease (CAD) in patients presenting with acute coronary syndrome (ACS) is an increasing clinical concern driven by genetic predisposition and lifestyle factors. This study compared clinical and laboratory characteristics of premature versus non-premature CAD and identified predictors of early-onset disease. Methods: This was a cross-sectional observational study of 2,000 patients admitted with confirmed ACS. Premature CAD was defined as males <55 years and females <65 years. Clinical, laboratory, and cardiological variables were compared between groups. Results: From December 2021 to March 2025, 2,000 patients were enrolled. Premature CAD occurred in 637 patients (31.9%), who were younger (median age 49 years) and predominantly male (68.4%). Smoking (32.8% vs. 9.4%), family history of dyslipidemia (20.4% vs. 3.7%), higher total cholesterol (174.0…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
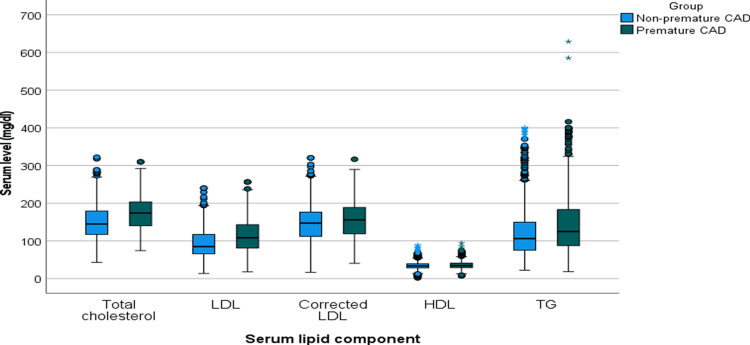 Figure 1
Figure 1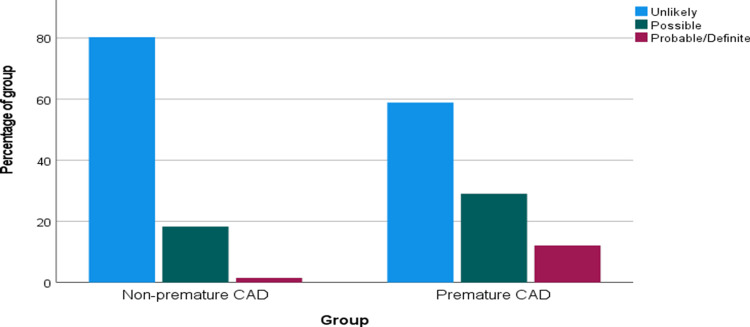 Figure 2
Figure 2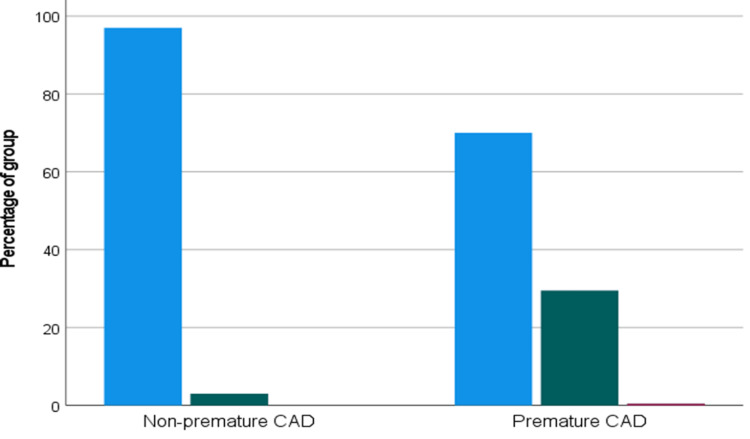 Figure 3
Figure 3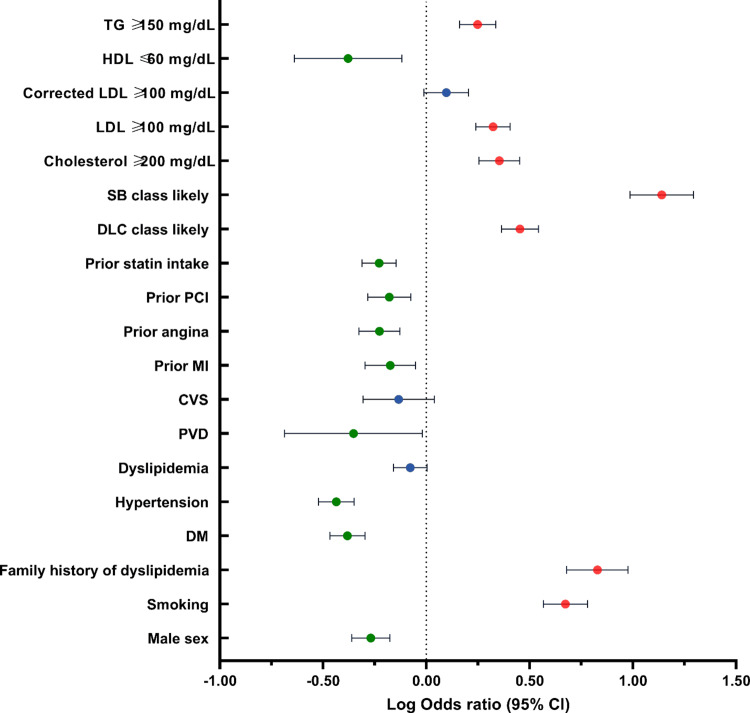 Figure 4
Figure 4| Variable | Non-premature CAD (N=1,363) | Premature CAD (N=637) | P value |
| Age (years) | 71 (65, 79) | 49 (44, 54) | <.001a |
| Male sex | 1092 (80.1%) | 436 (68.4%) | < .001> |
| Smoking | 128 (9.4%) | 209 (32.8%) | < .001> |
| Family history of dyslipidemia | 50 (3.7%) | 130 (20.4%) | < .001> |
| DM | 994 (72.9%) | 336 (52.7%) | < .001> |
| Hypertension | 1036 (76.0%) | 342 (53.7%) | < .001> |
| Dyslipidemia | 754 (55.3%) | 324 (50.9%) | .063 |
| PVD | 38 (2.8%) | 8 (1.3%) | .033 |
| CVS | 100 (7.3%) | 35 (5.5%) | .126 |
| Prior MI | 224 (16.4%) | 74 (11.6%) | .005 |
| Prior angina | 395 (29.0%) | 124 (19.5%) | < .001> |
| Prior PCI | 327 (24.0%) | 110 (17.3%) | .001 |
| Prior CABG | 96 (7.0%) | 19 (3.0%) | < .001> |
| Repeat attack | 433 (31.8%) | 139 (21.8%) | < .001> |
| Prior statin intake | 844 (61.9%) | 312 (49.0%) | < .001> |
| Variable | Non-premature CAD (N=1,363) | Premature CAD (N=637) | P value |
| Cholesterol (mg/dl) | 145.0 (117.2, 179.4) | 174.0 (140.4, 203.4) | <.001a |
| Cholesterol ≥200 mg/dl | 204 (15.0%) | 181 (28.4%) | < .001> |
| LDL (mg/dl) | 85.1 (65.7, 117.20 | 108.3 (81.2, 143.1) | <.00 a |
| LDL ≥100 mg/dl | 529 (38.8%) | 364 (57.1%) | < .001> |
| Corrected LDL (mg/dl) | 147.3 (112.1, 176.3) | 155.8 (118.7, 188.7) | <.001a |
| Corrected LDL ≥100 mg/dl | 1096 (80.4%) | 533 (83.7%) | .080 |
| HDL (mg/dl) | 33.6 (28.6, 39.4) | 34.4 (29.0, 41.0) | .004a |
| HDL <60 mg/dl | 1342 (98.5%) | 614 (96.4%) | .003 |
| TG (mg/dl) | 106.3 (75.3, 149.7) | 124.9 (87.7, 183.3) | <.001a |
| TG ≥150 mg/dl | 340 (24.9%) | 236 (37.0%) | < .001> |
| Dutch Lipid Clinic Network Criteria for FH | <.001b | ||
| Unlikely | 1094 (80.3%) | 375 (58.9%) | |
| Possible | 249 (18.3%) | 185 (29.0%) | |
| Probable/Definite | 20 (1.5%) | 77 (12.1%) | |
| Simon Broome Diagnostic Criteria for FH | <.001b | ||
| Unlikely | 1322 (97.0%) | 446 (70.0%) | |
| Possible | 41 (3.0%) | 188 (29.5%) | |
| Definite | 0 (0.0%) | 3 (0.5%) |
| Variable | Non-premature CAD (N=1,363) | Premature CAD (N=637) | P value |
| Diagnosis | .622a | ||
| Unstable angina | 339 (24.9%) | 182 (28.6%) | |
| NSTEMI | 668 (49.0%) | 254 (39.9%) | |
| STEMI | 356 (26.1%) | 201 (31.6%) | |
| In-hospital medication | |||
| Aspirin | 1363 (100.0%) | 637 (100.0%) | NA |
| P2Y12 inhibitor | 1363 (100.0%) | 637 (100.0%) | NA |
| Statin | 1363 (100.0%) | 634 (99.5%) | .032b |
| Antihypertensive | 1070 (78.5%) | 396 (62.2%) | < .001> |
| Coronary angiography done | 1140 (83.6%) | 578 (90.7%) | < .001> |
| Management | .061 | ||
| Conservative | 352 (25.8%) | 190 (29.8%) | |
| Interventional | 1011 (74.2%) | 447 (70.2%) | |
| Reason for conservative treatment | <.001c | ||
| No coronary angiography | 223/352 (63.4%) | 59/190 (31.1%) | |
| Normal coronary angiography | 45/352 (12.8%) | 71/190 (37.4%) | |
| Insignificant atherosclerotic CAD | 72/352 (20.5%) | 40/190 (21.1%) | |
| MVD | 5/352 (1.4%) | 3/190 (1.6%) | |
| Slow flow | 7/352 (2.0%) | 17/190 (8.9%) | |
| Interventions | |||
| Stent implantation | 849 (62.3%) | 390 (61.2%) | .648 |
| Balloon dilatation | 16 (1.2%) | 3 (0.5%) | .131 |
| CABG | 153 (11.2%) | 56 (8.8%) | .097 |
| Medications on discharge | |||
| Aspirin | 1322 (97.0%) | 606 (95.1%) | .038 |
| P2Y12 inhibitor | 1311 (96.2%) | 557 (87.4%) | < .001> |
| Statin | 1359 (99.7%) | 629 (98.7%) | .024 b |
| High-dose statin | 1284 (94.2%) | 584 (91.7%) | .042 |
| Ezetimibe | 84 (6.2%) | 66 (10.4%) | .001 |
| Evolocumab | 10 (0.7%) | 12 (1.9%) | .022 |
| Ezetimibe + Evolocumab | 6 (0.4%) | 3 (0.5%) | >.999 b |
| OAC | 29 (2.1%) | 22 (3.5%) | .080 |
| NOAC | 140 (10.3%) | 27 (4.2%) | < .001> |
| Antihypertensive | 1181 (86.6%) | 447 (70.2%) | < .001> |
| Variable | Non-premature CAD (N=1,363) | Premature CAD (N=637) | P value |
| Variable | Odds ratio | Lower 95% CI | Upper 95% CI | z-statistic | P value |
| Male sex | 0.54 | 0.43 | 0.67 | 5.683 | < .0001> |
| Smoking | 4.71 | 3.68 | 6.03 | 12.353 | < .0001> |
| Family history of dyslipidemia | 6.73 | 4.78 | 9.48 | 10.933 | < .0001> |
| DM | 0.41 | 0.34 | 0.50 | 8.803 | < .0001> |
| Hypertension | 0.37 | 0.30 | 0.45 | 9.888 | < .0001> |
| Dyslipidemia | 0.84 | 0.69 | 1.01 | 1.862 | .0627 |
| PVD | 0.44 | 0.21 | 0.96 | 2.074 | .0381 |
| CVD | 0.73 | 0.49 | 1.09 | 1.525 | .1273 |
| Prior MI | 0.67 | 0.50 | 0.89 | 2.805 | .005 |
| Prior angina | 0.59 | 0.47 | 0.74 | 4.494 | < .0001> |
| Prior PCI | 0.66 | 0.52 | 0.84 | 3.375 | .0007 |
| Prior statin intake | 0.59 | 0.49 | 0.71 | 5.438 | < .0001> |
| Cholesterol ≥200 mg/dl | 2.26 | 1.80 | 2.83 | 7.003 | < .0001> |
| LDL ≥100 mg/dl | 2.10 | 1.74 | 2.54 | 7.622 | < .0001> |
| Corrected LDL ≥100 mg/dl | 1.25 | 0.97 | 1.60 | 1.747 | .081 |
| HDL ≤60 mg/dl | 0.42 | 0.23 | 0.76 | 2.855 | .004 |
| TG ≥150 mg/dl | 1.77 | 1.45 | 2.17 | 5.537 | < .0001> |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Cardiovascular Disease and Adiposity · Cardiovascular Health and Risk Factors
Introduction
Premature coronary artery disease (CAD) refers to the development of CAD as acute coronary syndrome (ACS) at a younger age, typically before 55 years in men and 65 years in females [1]. One of the most prominent contributors to premature CAD is familial hypercholesterolemia (FH), a genetic condition marked by persistently elevated low-density lipoprotein cholesterol (LDL-C) levels from childhood, which significantly raises the risk of early-onset atherosclerotic cardiovascular disease (ASCVD) [2,3]. Although FH affects nearly one in every 250 individuals globally, it often goes undetected and untreated, especially in resource-limited settings [4]. The constant exposure to high LDL-C in FH accelerates endothelial damage and atherosclerotic plaque formation, frequently leading to ACS in younger individuals [5]. In many cases, an ACS event may be the first clinical indication of underlying FH, highlighting the need for timely identification and intervention [6]. In this context, it becomes crucial to define the clinical and biochemical features of premature CAD more precisely, particularly in patients presenting with ACS given that these individuals are often at heightened but underrecognized risk.
Exploring the patterns and prevalence of dyslipidemia, including FH and other hereditary or metabolic factors, is vital for improving screening protocols, enhancing risk prediction, and informing early preventive strategies. Moreover, social determinants of health such as socioeconomic status, education level, access to healthcare, and urban lifestyle also contribute significantly to the development and outcomes of premature CAD. These upstream factors can influence both the onset and management of premature CAD and should be considered when designing effective public health interventions [7].
This study aims to investigate the relationship between FH and premature CAD in patients admitted with ACS. Through the analysis of clinical profiles, lipid data, FH diagnostic scores, and procedural details, the research seeks to delineate the unique risk factors of premature CAD and reinforce the necessity of prompt diagnosis and aggressive lipid-lowering interventions in high-risk younger adults. In addition to genetic and lipid-related risk factors, unhealthy dietary habits, increased consumption of saturated fats and refined carbohydrates, and elevated body mass index (BMI) are recognized contributors to early atherosclerosis and should be considered in comprehensive preventive strategies even though these variables were not captured in our dataset.
Materials and methods
Study design
A cross-sectional observational study was conducted at the Department of Cardiology, Prince Khaled Bin Sultan Hospital, between December 2021 and March 2025. The study population consisted of 2,000 adult patients consecutively admitted with a confirmed diagnosis of ACS. Participants were classified into two groups based on age and sex: premature CAD (males under 55 years and females under 65 years) and non-premature CAD (males 55 years or older and females 65 years or older).
Study procedures
Data was obtained from electronic hospital records and included demographics, cardiovascular risk factors, laboratory test results, echocardiographic and angiographic findings, and details of in-hospital treatment. Lipid measurements were collected within 24 hours of admission. FH was identified using both the Dutch Lipid Clinic Network (DLCN) and Simon Broome criteria. Diagnosis of ACS was established based on internationally recognized guidelines [8,9]. Clinical features suggestive of dyslipidemia or FH, such as tendon xanthomas and corneal arcus, were evaluated [10]. LDL-C was assessed using a direct detect spectrometer (Abbott Alinity C system; Abbott Park, IL, USA). For patients already on lipid-lowering therapy at the time of admission, LDL-C was retrospectively estimated using correction factors derived from published medication efficacy data [11-15]. In-hospital interventions including medication use, reperfusion strategies, and discharge prescriptions were recorded. To convert lipid values into mg/dL, the multiplication factors used were 38.67 for cholesterol (total, high-density lipoprotein (HDL), LDL-C) and 88.57 for triglycerides.
Inclusion criteria
Patients aged 18 years or older were eligible if they had a confirmed diagnosis of ACS based on one or more of the following: clinical presentation, electrocardiogram findings, elevated cardiac biomarkers, or coronary angiography demonstrating ≥50% luminal narrowing. Only those with unstable angina, non-ST-elevation myocardial infarction (NSTEMI), or ST-elevation myocardial infarction (STEMI) and complete datasets were included.
Exclusion criteria
Exclusion criteria included incomplete lipid profiles, blood samples collected beyond 24 hours of Coronary Care Unit (CCU) admission, triglyceride levels >400 mg/dL, hemodynamic instability, cardiogenic shock, chronic kidney disease (estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m²), acute renal failure at admission, or alcohol consumption exceeding 14 units per week.
Statistical analysis
All patient data were anonymized before analysis. Statistical analyses were carried out using IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). Categorical data were expressed as frequencies and percentages and compared using Pearson's chi-square, Fisher's exact, or Fisher-Freeman-Halton tests, as appropriate. Continuous variables were assessed for normality. Normally distributed data were reported as mean ± standard deviation (SD); skewed variables were presented as median and interquartile range (IQR). Comparisons between groups used the Mann-Whitney U test. Logistic regression was employed to identify factors associated with premature CAD, with odds ratios (ORs) and 95% confidence intervals (CIs) reported. A p-value <.05 was considered statistically significant.
Results
Among 2,000 ACS patients, 637 (31.9%) had premature CAD and 1,363 (68.1%) had non-premature CAD. Patients with premature CAD were younger (median age 49 [IQR 44-54] vs. 71 [IQR 65-79], p<0.001) and more frequently male (68.4%). Smoking was more prevalent (32.8% vs. 9.4%, p<0.001), as was a family history of dyslipidemia (20.4% vs. 3.7%, p<0.001). in contrast, diabetes (52.7% vs 72.9%; p<0.001), hypertension (53.7% vs. 76.0%, p<0.001) and prior myocardial infarction (11.6% vs. 16.4%, p=0.005) were less frequent in the premature CAD group, as shown in Table 1. cardiological assessment revealed that ST segment elevation was more common in premature CAD (29.4% vs. 23.0%, p=0.002).
Lipid parameters were significantly elevated in the premature CAD group, with serum total cholesterol (174.0 mg/dl vs. 145.0 mg/dl, p<0.001), LDL-C (108.3 mg/dl vs. 85.1 mg/dl, p<0.001) and corrected LDL-C (155.8 mg/dl vs 147.3 mg/dl, p<0.001). A greater proportion of premature CAD patients had LDL-C ≥100 mg/dl (57.1% vs. 38.8%, p < .001) and cholesterol ≥200 mg/dl (28.4% vs 15%, p<0.001).
Triglyceride levels were also higher (median 124.9 mg/dl vs. 106.3 mg/dl; p<0.001), with more patients exceeding 150 mg/dl (37.0% vs. 24.9%, p<0.001). HDL-C was marginally higher in premature CAD (p=0.004), as shown in Table 2 and Figure 1.
Box plot illustrating the serum lipid levels in patients with premature and non-premature coronary artery disease (CAD). The Y-axis indicates the percentage of patients. The box represents the interquartile range, with the median indicated by the central line. Whiskers show minimum and maximum values excluding outliers (round markers) and extreme values (asterisks). Abbreviations: LDL – Low-Density Lipoprotein; TG – Triglyceride
FH risk scores were significantly higher among patients with premature CAD. According to the DLCN criteria, possible FH was observed in 185/637 (29.0%) patients with premature CAD compared with 249/1363 (18.3%) in the non-premature group, while probable/definite FH occurred in 77/637 (12.1%) versus 20/1363 (1.5%), respectively (both p<0.001). Similarly, the Simon Broome diagnostic criteria demonstrated higher rates of possible FH in the premature CAD group (188/637 [29.5%] vs. 41/1363 [3.0%]) and definite FH (3/637 [0.5%] vs. 0/1363 [0.0%]; p<0.001), as shown in Table 2 and Figures 2, 3.
Bar chart showing the distribution of Dutch Lipid Clinic Network criteria classifications in patients with premature and non-premature coronary artery disease (CAD).
Bar chart showing the Simon Broome Diagnostic Criteria categories in patients with premature and non-premature coronary artery disease (CAD). The Y-axis represents the percentage of patients.
Regarding lipid-lowering therapy, prior statin use was significantly lower in the premature CAD group compared to the non-premature group (49.0% vs. 61.9%; p<0.001), as shown in Table 1. During hospitalization, nearly all patients received statins in accordance with guideline-recommended care for ACS. At discharge, statin prescription rates remained high and comparable between groups, while ezetimibe (10.4% vs. 6.2%) and evolocumab (1.9% vs. 0.7%) use was higher in the premature CAD group, reflecting a trend toward more intensive lipid-lowering in younger high-risk patients. These patterns are detailed in Table 3. Also, coronary angiography was performed more often in premature CAD (90.7% vs. 83.6%, p<0.001), as shown in Table 3.
Multivariate risk analysis revealed several significant positive predictors for premature CAD: smoking (OR=4.71, 95% CI: 3.68-6.03, p<0.0001), family history of dyslipidemia (OR=6.73, p<0.0001), LDL-C ≥100 mg/dl (OR=2.10, p<0.0001), total cholesterol ≥200 mg/dl (OR=2.26, p<0.0001), and TG ≥150 mg/dl (OR 1.77, 95% CI 1.45-2.17). Negative predictors were diabetes mellitus (OR=0.41, p<0.0001), hypertension (OR=0.37, p<0.0001), and prior statin use (OR=0.59, p<0.0001) as presented in Table 4 and Figure 4.
Forest plot of log-transformed odds ratios of risk factors for premature coronary artery disease (CAD). Red markers indicate statistically significant increased risk, green markers indicate statistically significant decreased risk, and blue markers indicate non-significant associations.Abbreviations: DM – Diabetes Mellitus; PAD – Peripheral Arterial Disease; CVS – Cardiovascular Disease; MI – Myocardial Infarction; PCI – Percutaneous Coronary Intervention; PVD – Peripheral Vascular Disease; LDL-C – Low-Density Lipoprotein Cholesterol; HDL-C – High-Density Lipoprotein Cholesterol; TG – Triglyceride; DLC –Dutch Lipid Clinic; SB – Simon Broome.
Discussion
This study provides a comprehensive comparison between premature and non-premature CAD in patients presenting with ACS, revealing clear differences in demographics, risk factors, lipid abnormalities, diagnostic assessment, and in-hospital management. Patients with premature CAD were younger and predominantly male, consistent with prior literature [16,17]. Smoking (OR: 4.71) and family history of dyslipidemia (OR: 6.73) emerged as the strongest factors associated with premature CAD, in agreement with large international studies such as INTERHEART that identified smoking and dyslipidemia as major drivers of early myocardial infarction [18,19].
Unlike older patients, in whom metabolic syndromes are dominant contributors, premature CAD appears more strongly linked to behavioral and genetic risk factors. The lower prevalence of diabetes and hypertension in the premature group (p<0.001 for both) supports a distinct pathogenic pathway and is consistent with regional data showing a reduced metabolic burden among younger patients despite serious cardiovascular events [20].
Atherogenic lipid abnormalities were a defining feature of premature CAD in our cohort. Patients with early-onset disease demonstrated significantly higher total cholesterol, LDL-C, corrected LDL-C, and triglyceride levels (all p<0.001). Elevated lipid thresholds, including total cholesterol ≥200 mg/dL, LDL-C ≥100 mg/dL, and triglycerides ≥150 mg/dL, were independently associated with premature CAD (OR: 2.10 and OR: 1.77), underscoring their role in early atherosclerosis development [21].
Clinical assessment using FH diagnostic tools further highlighted the genetic contribution to premature disease. The DLCN criteria identified higher rates of both possible and probable/definite FH in premature CAD, and similar findings were observed with the Simon Broome classification. These results are consistent with prior evidence demonstrating underdiagnosis and undertreatment of FH, particularly in younger adults presenting with ACS [22,23]. Given that untreated FH can increase the risk of premature CAD up to 20-fold [24], early detection and family-based cascade screening are essential, especially in regions with limited access to specialized lipid services. Despite differing risk profiles, both groups presented with similar ACS subtypes, suggesting convergence of ischemic outcomes despite distinct etiologies. Premature patients were more likely to undergo coronary angiography and receive interventional therapy, potentially reflecting clinical decision-making patterns and selection bias. Notably, a substantial proportion of conservatively managed premature patients had non-obstructive coronary findings, suggesting mechanisms such as microvascular dysfunction or vasospasm that are increasingly recognized in younger populations [25].
Discharge pharmacotherapy was broadly similar between groups, with high statin and aspirin use. However, younger patients more frequently received ezetimibe and PCSK9 inhibitors, consistent with guideline-directed management of FH or persistent hyperlipidemia [26]. Although corrected LDL-C was slightly higher in premature CAD, it was not significant in multivariate analysis (p=0.081), possibly reflecting acute lipid variability and methodological limitations [27].
The inverse association of prior statin therapy, diabetes, and hypertension with premature CAD may reflect delayed disease onset in treated chronic conditions, survivorship effects, and the stronger influence of genetic and behavioral factors, particularly smoking in younger individuals. The widespread use of intensive lipid-lowering therapy in premature CAD aligns with contemporary guideline recommendations for aggressive risk reduction in high-risk young patients [28].
These findings underscore the need for targeted public health strategies focusing on early identification of at-risk young individuals, particularly smokers and those with a family history of dyslipidemia. Recommended approaches include early lipid screening, age-adjusted risk assessment tools, and implementation of cascade testing and universal cholesterol screening in young adults, as endorsed by international guidelines [29,30].
Social determinants of health also play a critical role in premature CAD. Socioeconomic status, education, occupational stress, healthcare access, and urban lifestyle influence both disease prevalence and severity. Individuals from disadvantaged backgrounds are more likely to smoke, maintain unhealthy diets, and receive inadequate preventive care, all of which accelerate atherosclerosis [31].
Addressing these upstream determinants through public health policy and education is essential to reduce disparities in early cardiovascular disease.
Limitations
This study has several limitations. It’s a cross-sectional observational study that prevents the assessment of causality or long-term outcomes. The absence of genetic confirmation for FH limits diagnostic precision. Additionally, the single-center setting may reduce the generalizability of our findings. Lifestyle, dietary patterns, and BMI were not evaluated, and the imaging data lacked advanced diagnostic modalities. Future multicenter, prospective studies incorporating genetics are needed.
Conclusions
Premature CAD in patients presenting with ACS shows a distinct profile with higher rates of smoking, dyslipidemia, and FH, but fewer traditional comorbidities. This study is unique in applying dual FH diagnostic criteria in a large, real-world cohort from an underrepresented region. These findings highlight the need for early detection and aggressive lipid-lowering strategies in high-risk younger adults.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heart disease epidemic in Pakistan: women and men at equal risk Am Heart J Jafar TH Jafary FH Jessani S Chaturvedi N 2212261502005 https://www.sciencedirect.com/science/article/abs/pii/S 000287030400657 X 1608692210.1016/j.ahj.2004.09.025 · doi ↗ · pubmed ↗
- 2Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society Eur Heart J Nordestgaard BG Chapman MJ Humphries SE 347834903420132395625310.1093/eurheartj/eht 273PMC 3844152 · doi ↗ · pubmed ↗
- 3Homozygous familial hypercholesterolaemia: new insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society Eur Heart J Cuchel M Bruckert E Ginsberg HN 214621573520142505366010.1093/eurheartj/ehu 274PMC 4139706 · doi ↗ · pubmed ↗
- 4Mutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the Copenhagen General Population Study estimated a prevalence of 1 in 217Eur Heart J Benn M Watts GF Tybjærg-Hansen A Nordestgaard BG 138413943720162690894710.1093/eurheartj/ehw 028 · doi ↗ · pubmed ↗
- 5Defining severe familial hypercholesterolaemia and the implications for clinical management: a consensus statement from the International Atherosclerosis Society Severe Familial Hypercholesterolemia Panel Lancet Diabetes Endocrinol Santos RD Gidding SS Hegele RA 850861420162724616210.1016/S 2213-8587(16)30041-9 · doi ↗ · pubmed ↗
- 6Genetic identification of familial hypercholesterolemia within a single U.S. health care system Science Abul-Husn NS Manickam K Jones LK 354201610.1126/science.aaf 700028008010 · doi ↗ · pubmed ↗
- 7Association of socioeconomic position with health behaviors and mortality JAMA Stringhini S Sabia S Shipley M Brunner E Nabi H Kivimaki M Singh-Manoux A 1159116630320102033240110.1001/jama.2010.297PMC 2918905 · doi ↗ · pubmed ↗
- 8Fourth universal definition of myocardial infarction (2018)Circulation Thygesen K Alpert JS Jaffe AS Chaitman BR Bax JJ Morrow DA White HD 051138201810.1161/CIR.000000000000061730571511 · doi ↗ · pubmed ↗