Distinct Characteristics of Patients With Fragility Hip Fracture in Greece: Evidence From the Greek National Fragility Hip Fracture Registry Utilizing the Minimum Common Data Set
Efthymios Iliopoulos, Theo Tosounidis, Reichan Molla Mustafa, Athanasia Charmpi, Fotios Tilkidis, Alkison Kotsis, Dimitra Melissaridou, Maria Sentona, Georgios Graikos, Androniki Kyprianou, Irini Tatani, Ioannis Gkiatas, Byron Chalidis, Ioannis V Papachristos, Christiana Zidrou

TL;DR
This study uses Greece's first national hip fracture registry to show that Greek patients have unique characteristics and healthcare challenges, such as delayed surgeries and high mortality rates.
Contribution
The study presents the first national fragility hip fracture registry in Greece, offering insights into local healthcare system performance and patient outcomes.
Findings
Most patients were elderly females with peri-trochanteric fractures and high pre-injury independence.
Only 31% of patients received surgery within 48 hours, leading to longer hospital stays and higher mortality.
Greek 30-day mortality rates are comparable to other European countries despite healthcare system delays.
Abstract
Background Over the past two decades, fragility hip fracture registries have been implemented in various countries worldwide. These registries have played a key role in documenting the state of individual health care systems, highlighting the specific challenges they face, and showcasing the unique characteristics of each population. The aim of the present study is to highlight the distinct characteristics of the Greek fragility hip fracture patients, utilizing the data from the first two years of the first national fragility hip fracture registry in Greece. Materials and methods Nine orthopaedic departments from eight hospitals across the country participated in this prospective multicenter study. All cases of hip fragility fractures between September 2022 and December 2024 were prospectively recorded in a centralized database. Data collection was based on the 21-point Minimum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
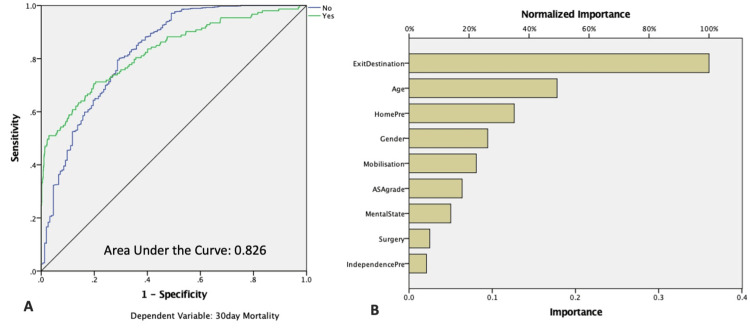 Figure 1
Figure 1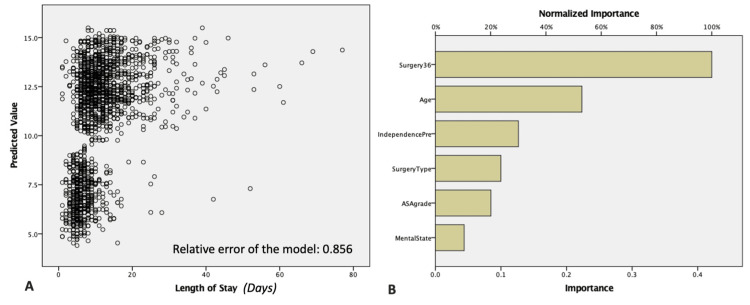 Figure 2
Figure 2| Variables | Frequency | Percentage | p-value for 30-day mortality | p-value for LOS | ||
| Sex | Female | 1510 | 70.6 | <0.001* | 0.73 | |
| Male | 629 | 29.4 | ||||
| Age (Years) | 82.38 | ±8.43 | <0.001* | 0.048* | ||
| Pre-Injury Residence | Own Home | 2006 | 94.5 | <0.001* | 0.7 | |
| Nursing Home | 93 | 4.4 | ||||
| Hospital | 12 | 0.6 | ||||
| Rehabilitation Centre | 4 | 0.2 | ||||
| Unknown | 7 | 0.3 | ||||
| Missing Values | 17 | (0.8) | ||||
| Pre-Injury Mobility | Free | 838 | 39.8 | <0.001* | 0.02* | |
| Outside with 1 stick | 511 | 24.3 | ||||
| Outside with 2 sticks | 301 | 14.3 | ||||
| Inside only – Never Outside | 392 | 18.6 | ||||
| No Mobility | 32 | 1.5 | ||||
| Unknown | 30 | 1.4 | ||||
| Missing Values | 35 | (1.6) | ||||
| Mental State | Normal | 1368 | 64.0 | <0.001* | 0.007* | |
| Known Dementia | 478 | 22.3 | ||||
| Not-Known Dementia but Positive Tests | 249 | 11.6 | ||||
| Missing Values | 44 | (2.1) | ||||
| ASA Grade (2.72±0.87) | I | 102 | 4.8 | <0.001* | <0.001* | |
| II | 832 | 39.4 | ||||
| III | 784 | 37.1 | ||||
| IV | 345 | 16.3 | ||||
| V | 48 | 2.3 | ||||
| Missing Values | 28 | (1.3) | ||||
| Fracture Type | Intracapsular | 861 | 40.25 | - | - | |
| Peri-trochanteric | 1245 | 58.20 | ||||
| Other & Missing Values | 33 | 1.5 | ||||
| Variables | Frequency | Percentage | p-value for 30-day mortality | p-value for LOS | |
| Fracture Type | Undisplaced Intracapsular | 80 | 3.7 | 0.71 | 0.17 |
| Displaced Intracapsular | 781 | 36.6 | |||
| Intertrochanteric | 1121 | 52.5 | |||
| Subtrochanteric | 124 | 5.8 | |||
| Other | 30 | 1.4 | |||
| Missing Values | 3 | (0.1) | |||
| Type of Surgery | Non-Operative Management | 114 | 5.6 | 0.03* | <0.001* |
| Cannulated Screws | 10 | 0.5 | |||
| Dynamic Hip Screw (DHS) | 11 | 0.5 | |||
| Intramedullary Nailing | 1124 | 54.7 | |||
| Hip Hemiarthroplasty | 688 | 33.5 | |||
| Total Hip Arthroplasty | 71 | 3.5 | |||
| Other | 36 | 1.8 | |||
| Missing Values | 85 | (4) | |||
| Type of Surgery for Intracapsular Fractures | Hip Hemiarthroplasty | 675 | 80.6 | - | - |
| Total Hip Arthroplasty | 70 | 8.4 | |||
| Other | 93 | 11 | |||
| Missing Values | 23 | (2.7) | |||
| Type of Surgery for Peri-Trichanteric (Inter- + Sub- Trochanteric) Fractures | Dynamic Hip Screw (DHS) | 8 | 0.7 | - | - |
| Intramedullary Nailing | 1116 | 91.5 | |||
| Other | 97 | 7.8 | |||
| Missing Values | 24 | (1.9) | |||
| Surgery within 48 hours from admission | Yes | 585 | 30.9 | 0.07 | <0.001* |
| No | 1308 | 69.1 | |||
| Missing Values | 246 | (11.5) | |||
| Type of Anaesthesia | General Anaesthesia | 464 | 24.0 | 0.09 | 0.2 |
| Spinal Anaesthesia | 1461 | 75.5 | |||
| Other | 8 | 0.4 | |||
| Missing Values | 206 | (9.6) | |||
| Variables | Frequency | Percentage | p-value for 30-day mortality | p-value for LOS |
| New Pressure Ulcer | - | - | ||
| Yes | 283 | 13.2 | ||
| No | 1741 | 81.4 | ||
| Missing Values | 115 | (5.4) | ||
| LOS (Days), mean±SD, median (IQR) | 10.68±8.11, 9 (0-132) | 0.27 | - | |
| Medical Support | - | - | ||
| Internal Medicine | 1233 | 59.61 | ||
| Geriatrics | 35 | 1.7 | ||
| None | 764 | 36.6 | ||
| Other | 54 | 2.6 | ||
| Missing Values | 53 | (2.5) | ||
| Mobilisation within 24 hours of Surgery | <0.001* | 0.5 | ||
| Yes | 1096 | 54.2 | ||
| No | 824 | 40.7 | ||
| Missing Values | 219 | (10.2) | ||
| In-Hospital Mortality | - | - | ||
| Yes | 84 | 4.0 | ||
| No | 2020 | 96.0 | ||
| Missing Values | 35 | (1.6) | ||
| Exit Destination | <0.001* | 0.08 | ||
| Own Home | 1233 | 58.9 | ||
| Nursing Home | 57 | 2.7 | ||
| Rehabilitation Centre | 635 | 30.3 | ||
| Unknown | 46 | 2.2 | ||
| Death | 84 | 4.0 | ||
| Missing Values | 84 | (3.9) | ||
| Discharge Osteoporosis Medication | - | - | ||
| Start | 343 | 16.8 | ||
| Continued Same | 155 | 7.6 | ||
| Changed | 47 | 2.3 | ||
| (Subtotal – Patients with anti-osteoporotic medication at discharge) | 545 | 26.6 | ||
| Stopped | 3 | 0.1 | ||
| Unknown | 1499 | 73.2 | ||
| Missing Values | 92 | (4.3) | ||
| 30-Day Mortality | - | 0.27 | ||
| Yes | 175 | 10.9 | ||
| No | 1437 | 89.1 | ||
| Missing Values | 527 | (24.6) | ||
| Variables | Sig. (p) | Beta | OR (95% C.I.) | Independent Variable Importance | Normalised Importance (%) |
| Age (Years) | <0.001* | 1.080 | 1.045 – 1.118 | 0.178 | 49.3 |
| ASA grade | 0.115 | 1.273 | 0.943 – 1.719 | 0.064 | 17.7 |
| Gender | <0.001* | 0.406 | 0.261 – 0.632 | 0.095 | 26.2 |
| Mental State | 0.979 | 0.94 | 0.50 – 1.76 | 0.050 | 13.9 |
| Pre-Injury Residence | <0.001* | 0.287 | 0.156 – 0.531 | 0.126 | 35.1 |
| Pre-Injury Mobility | 0.599 | 1.150 | 0.683 – 1.937 | 0.021 | 5.8 |
| Surgery | 0.521 | 1.963 | 0.251 – 15.369 | 0.025 | 6.9 |
| Mobilisation within 24 hours of Surgery | 0.385 | 5.901 | 0.46 – 73.44 | 0.081 | 22.4 |
| Exit Destination | <0.001* | 0.367 | 0.227 – 0.594 | 0.360 | 100 |
| Variable | Adjusted OR | OR (95% CI) | p-value |
| Age (per year) | 1.06 | 1.029 – 1.085 | <0.001* |
| ASA Grade | 1.31 | 0.983 – 1.740 | 0.065 |
| Gender | 2.17 | 1.486 – 3.178 | <0.001* |
| Metal State | 0.94 | 0.726 – 1.215 | 0.634 |
| Pre-Injury Residence | 2.20 | 1.259 – 3.834 | 0.006* |
| Pre-Injury Mobility | 1.024 | 0.686 – 1.528 | 0.909 |
| Surgery | 0.57 | 0.240 – 1.362 | 0.206 |
| Mobilisation within 24 hours of Surgery | 0.88 | 0.619 – 1.244 | 0.462 |
| Exit Destination | 2.12 | 1.841 – 2.444 | <0.001* |
| Variables | Sig. (p) | Beta | OR (95% C.I.) | Independent Variable Importance | Normalised Importance (%) |
| Age (Years) | 0.098 | -0.042 | -0.080 – 0.007 | 0.223 | 53 |
| ASA grade | 0.661 | -0.010 | -0.495 – 0.314 | 0.085 | 20.1 |
| Pre-Injury Mobility | 0.001* | 0.084 | 0.544 – 2.133 | 0.127 | 30 |
| Mental State | 0.937 | 0.002 | -0.496 – 0.538 | 0.044 | 10.4 |
| Type of Surgery | 0.823 | -0.005 | -0.506 – 0.402 | 0.100 | 23.7 |
| Timing of Surgery | <0.001* | -0.393 | -7.095 – -5.704 | 0.421 | 100 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Bone health and osteoporosis research · Bone fractures and treatments
Introduction
Over the past two decades, fragility hip fracture registries have been established in numerous countries globally, serving as essential tools for evaluating healthcare system performance and establishing a unified benchmarking system. These registries have contributed significantly to identifying system-specific challenges and delineating the distinct epidemiological and clinical characteristics of national populations [1-3]. Throughout the years, such registries have contributed to improvements in local healthcare systems, including reductions in both the time to surgery and patient mortality rates [4,5].
Pioneering registries, such as the National Hip Fracture Registry in the United Kingdom, along with those in the United States, Australia, and New Zealand, and the Scandinavian countries, have now reached a mature stage. These registries are actively identifying key issues and providing data-driven recommendations [1,2,4-7]. While their findings can inform national policies and support country-specific conclusions, direct comparisons between registries have proven to be unreliable and, in some cases, not feasible [8]. This issue has become increasingly evident in recent years, as new registries are being established in new countries, each with distinct healthcare systems and population characteristics, which face different challenges [3,9,10]. The Global Fragility Fracture Network (FFN) has introduced the Minimum Common Data Set, which is a standardized set of 21 variables aimed at harmonizing data collection across different registries and promoting international collaboration in healthcare audits [11].
This study presents the results from the first two years of Greece’s national fragility hip fracture registry, established by the FFN Greek Chapter (FFN-Gr) [12]. It describes key features of the Greek healthcare system and elderly population, identifies local challenges in hip fracture care, and compares the findings with data from other countries.
Preliminary results of this article were previously presented as a wall poster at the 13^th^ Fragility Fracture Network Global Congress, October 2-4, 2025, Porto, Portugal.
Materials and methods
Following an initiative of the FFN Gr [12], a nationwide, multicentre collaborative group was established with the aim of developing the first national registry for fragility hip fractures in Greece. Within this framework, nine orthopaedic departments from eight hospitals distributed across different geographic regions of the country participated in the present study, ensuring broad national representation of clinical practice and patient demographics.
Study population
Eligibility for inclusion in the registry and the present analysis was based on admission to one of the participating orthopaedic departments due to a low-energy fragility fracture of the proximal femur. Fragility fractures were defined as fractures resulting from a fall from standing height or less, or occurring in the absence of significant trauma. Patients were excluded if the fracture resulted from high-energy mechanisms, if they sustained polytrauma, if they were younger than 60 years of age, or if the fracture was considered pathological in nature (e.g., secondary to malignancy).
All consecutive patients presenting with fragility fractures of the hip and treated at the participating centres between September 2022 and December 2024 were prospectively identified and enrolled. Data collection was conducted in a prospective manner at each site by designated members of the orthopaedic or multidisciplinary care teams. To ensure data protection and patient confidentiality, all collected data were anonymised prior to entry and stored in a centralized, secure electronic database accessible only to authorized study personnel.
Data collection
Data collection was standardized across all centres using the 21-point Minimum Common Data Set (MCDS) recommended by the FNN [11]. This dataset includes key variables related to patient demographics, patients’ pre-injury status, fracture characteristics, perioperative management, and hospitalization data, allowing for consistency and comparability both nationally and internationally. More specifically, surgery within 48 hours was calculated from the admission of the patient to the hospital. Mobilisation within 24 hours was calculated from the time the operation ended, was assessed by the physiotherapists in the orthopaedic wards, and was defined as positive when the patient managed to sit out of bed. Pressure ulcers were diagnosed and classified using the European Pressure Ulcer Advisory Panel (EPUAP)/National Pressure Ulcer Advisory Panel (NPUAP) classification system.
Only new ulcers developed during hospitalisation were reported, while pre-existing ulcers were documented but excluded from the analysis. Discharge destination is categorized into mutually exclusive groups: own home, nursing home, inpatient rehabilitation, transfer to another acute hospital, or in-hospital death. Each patient was assigned to a single discharge category. In addition to the standard MCDS variables, the 30-day mortality was recorded as an outcome measure, given its recognized importance as a quality indicator in hip fracture care, via the national civil registry linkage and hospital records, with the preferable end point at 30 days post surgery. In-hospital deaths were included in the 30-day mortality models to avoid immortal time bias.
Ethics
Ethical approval was obtained from the institutional review board of each participating center. The coordinating center approval was granted by the University General Hospital of Alexandrouplis Scientific Ethical Board (approval number ES19/Th21/6-10-2022). Informed consent was waived due to the observational registry design. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Statistical analysis
Data from the central database were analysed using the IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, New York, United States). A significance level of 0.05 was applied for all statistical tests. The same program was used to perform univariate analyses (chi-square test, independent samples t-test, and one-way ANOVA, Mann-Whitney U test) and multivariate models (logistic and multiple regression), as well as neural network-based machine learning factor analysis to evaluate 30-day mortality and in-hospital length of stay. Continuous variables were assessed for normality using the Shapiro-Wilk test and visual inspection of histograms. Normally distributed variables were analyzed using parametric tests, while non-normally distributed variables were analyzed using non-parametric alternatives. Assumptions of linear regression, including normality of residuals and homoscedasticity, were evaluated.
Results
A total of 2139 patients with a fragility hip fracture admitted to the involved orthopaedic departments were included in the study. The majority of the patients were female (70.6%, n=1510) at a mean age of 82.4 ±8.4 years. Almost one quarter of the patients (22.3%, n=478) had known dementia at the time of admission. A significant proportion of the patients (95%, n=2006) were staying at their own home before the injury, and 65% (n=1349) of the patients were fully independent, mobilising freely or with one stick outdoors. Most of the patients had peri-trochanteric hip fractures (58,2%, n=1245), while less frequent were the intracapsular hip fractures. (Table 1).
Most of the patients were treated surgically (94,4%, n=1940), with a mean ASA (American Society of Anesthesiologists) grade of 2.72 ±0.87. The surgical intervention was performed within 48 hours of their admission to the hospital in only 31% (n=585) of the cases, mostly under spinal anaesthesia (75.5%, n=1461), while the rest were under general anaesthesia. Most of the extracapsular fractures were treated by using an intramedullary nail (91.5%, n=1116), and most of the patients with intracapsular fractures were treated with hip hemiarthroplasty (80.6%, n=675) (Table 2).
The mean in-hospital length of stay (LOS) was 10.68 ±8.1 days, with 13.2% (n=283) developing a new pressure ulcer during hospitalisation. LOS was non-normally distributed and is reported as median with interquartile range (IQR) in Table 3; median LOS was nine days (IQR 0-132). Group comparisons were performed using the Mann-Whitney U test. Internal medicine doctors supported the Orthopaedic patients during the more acute hospitalisations in 59% (N= 1233) of the cases. Unfortunately, the number of Geriatric patients was extremely low (only 1.7%), as in Greece, the Geriatric and Orthogeriatric subspecialties are yet to be officially recognised. Only 54.2% (n=1096) of the patients managed to mobilise outside of the bed on the first postoperative day. The most frequent discharge destination was the patients’ home (59%, n=1233), followed by a rehabilitation centre (30.3%, n=635). Unfortunately, only about one fourth of the patients receive anti-osteoporotic medication at discharge (26.6%, n=545). The in-hospital mortality was 4% (n=84); the mortality rate was significantly higher for the patients discharged to rehabilitation clinics compared to those discharged to their own home (p<0.001). Of 2139 patients in the registry, 30-day mortality status was available for 1612 (75.4%). Among patients with complete follow-up, 175 deaths occurred, corresponding to a 30-day mortality of 10.9% (n=175) (Table 3).
Univariate analysis revealed that the age, ASA grade, gender, mental state, the type of residence pre-injury, the level of independence, the conservative management, the mobilisation on the first postoperative day, and the exit destination significantly affected the 30-day mortality of the patients (p<0.001). The length of stay had a positive correlation with increased age and ASA grade (p<0.05). It was also significantly affected by the pre-injury mobility levels, known dementia, type of surgery (with conservative management and cannulated hip screws having significantly less LOS), and the timing of surgery (p=0.02 - <0.001).
Multivariate analysis model with the 30-day mortality as dependent variable revealed that only age, male sex, pre-injury residence, and discharge destination were the only variables that maintained their significant influence on the 30-day mortality (Table 4). Neural network analysis for the 30-day mortality confirmed these results by reaching a good predictive value with an AUC of 0.826. The discharge destination and the age were the most important predictive variables (Table 4 and Figure 1).
Neural Network analysis for the 30-day mortality.A: ROC curve analysis; B: Bar chart for neural network analysis
Multiple imputation using fully conditional specification was performed to address 24.6% missing mortality data (30 imputations). In pooled logistic regression analysis, age (OR 1.06 per year, p<0.001), gender (OR 2.17, p<0.001), pre-admission residence (OR 2.20, p=0.006), and discharge destination (OR 2.12, p<0.001) were independently associated with the 30-day mortality. Other variables were not statistically significant after adjustment (Table 5).
The multivariate model for the length of stay as the dependent variable revealed only the prompt surgical intervention and the pre-injury mobility status as the only significant factors (Table 6). Neural network analysis confirmed that surgery within 48 hours of admission was the most significant factor affecting the prolonged hospital stay (Table 6 and Figure 2).
Neural Network analysis for the length of stay.A: Scatter plot for neural network analysis; B: Bar chart for neural network analysis
Discussion
The establishment of the Fragility Hip Fracture Registry in Greece, led by the FNN-Gr in recent years, has shed light on the challenges facing the Greek healthcare system and offered valuable insights into the conditions within public hospitals [9]. This study highlights several key and distinct characteristics of elderly patients suffering from fragility hip fractures in Greece. Although the majority of these patients do not undergo surgery promptly, the 30-day mortality rate remains relatively moderate at approximately 11%. Factors such as age, gender, and place of residence appear to influence mortality outcomes. Notably, delay in surgery emerged as the primary contributor to prolonged hospital stay, pointing to a clear area for targeted improvement.
Patients from different countries vary in demographics, comorbidities, and fracture types; consequently, healthcare professionals in each system face different challenges, accounting for the local cultural factors as well. In the Greek cohort, the mean age was approximately 82.5 years, comparable to that in several Scandinavian and Central European countries such as Sweden, Denmark, Norway, the United Kingdom, Germany, France, and the Netherlands (82-85 years). However, it was lower than in some Mediterranean countries like Italy and Spain, where the mean age ranges from 86 to 87 years [8,13-15]. In Greece, over 70% of patients were female, a proportion similar to those observed in the United Kingdom, Ireland, and Germany (69-72%). Sweden reported slightly lower rates (66%), while Italy and Spain had higher rates (76-77%). A significant majority (95%) of Greek patients were living independently at home prior to their injury, markedly higher than the European average of 71-75%, and even higher than the higher reported percentages of the United Kingdom, Ireland, and Italy (81-91%) [8,15]. Pre-injury mobility levels in Greece were also comparable to those in other European countries, with about 65% of patients able to walk unaided or with a single walking stick outdoors. The mean ASA score in the Greek cohort was 2.7, with only 55.7% of patients classified as ASA grade III or above. This is noticeably lower than reported figures across Europe, which range from 61% to 74.5% [8,15,16]. Cognitive impairment (either diagnosed dementia or positive cognitive screening) was present in 34% of Greek patients, aligning with the European range of 17% to 44% [8]. Usually, intracapsular hip fractures are more frequent in this type of patient cohort compared to peritrochanteric ones [8]. This proportion is opposite in the Greek and Spanish cohort, with peri-trochanteric fractures reaching almost 60% of hip fragility fractures [8,10,16].
According to a review of European annual reports of hip fracture registries by Werner et al., healthcare systems manage the burden of fragility hip fractures in diverse ways, influenced by local policies, available funding, human resources, and clinical expertise [8]. In Greece, conservative treatment for fragility hip fractures was applied in 5.6% of cases. This rate sits at the higher end of the European spectrum (1-5%), with Ireland reporting a comparable rate of 5%. For intracapsular femoral neck fractures, the most commonly performed procedure in Greece was hip hemiarthroplasty, accounting for 33.5% of cases. In contrast, total hip arthroplasty and cannulated screw fixation were rarely used, at 3.5% and 0.5%, respectively. This treatment pattern is also observed in Spain and the Netherlands. However, other European countries, including Italy, Sweden, and Denmark, show a greater preference for total hip arthroplasty, with rates exceeding 10%. Cannulated screw fixation is more commonly used in Scandinavian countries, where it accounts for 10-15% of treatments. For peritrochanteric fractures, the intramedullary proximal femoral nailing is the preferred method in Greece, used in nearly 55% of cases. The dynamic hip screw (DHS) is rarely chosen, appearing in only 0.5% of cases. A similar preference for intramedullary nails is observed in Germany, Italy, and Spain. Conversely, Ireland and Scandinavian countries report higher DHS usage (15-20%), although IM nails remain the dominant choice. In contrast, DHS is more frequently used in Scotland and England. In terms of anaesthesia, approximately 75% of surgeries in Greece are performed under spinal, a pattern similar to that of Ireland, Italy, and Norway. Sweden and Spain favour spinal anaesthesia even more, with usage rates above 90%, while Germany predominantly uses general anaesthesia (94%). Countries like England, Scotland, and the Netherlands show a more balanced use of both techniques [8].
One significant weakness of the Greek healthcare system is the delayed surgical intervention, with only 30% of patients undergoing surgery within 48 hours of admission, substantially lower than the European average, which ranges from 48% to 95% [8,16]. Additionally, only 55% of patients in Greece were mobilised out of bed on the first postoperative day, again falling short of the European range of 67-82%. This delay in mobilisation contributed to a higher incidence of pressure sores, present in 13% of Greek patients, compared to 3-4.8% in countries such as England, Germany, Italy, and Spain [8]. Approximately 25% of Greek patients were discharged with anti-osteoporotic medications, a rate comparable to Italy and the Netherlands but significantly lower than in countries like England, Ireland, and Denmark. Notably, around 60% of patients in Greece were discharged directly to their homes, the highest percentage reported in Europe, where rates range between 12% and 52% [8,16].
In the Greek cohort, in-hospital mortality was recorded at 4%, while 30-day mortality reached 10.9%. The in-hospital mortality rate aligns with those reported across other European countries, which range from 1.5% to 6%. However, the 30-day mortality rate in Greece was slightly higher than the European average, which falls between 5.5% and 9.5% [8]. Among the variables examined, only increased age, male gender, pre-injury living situation, and discharge destination were found to have a significant impact on mortality. These findings are in line with other registries, such as the Spanish, in which the same factors affect the mortality rates significantly. The Spanish registry reports significant influence by the higher ASA grade and time to surgery more than 48 hours, as well as variables that are not significant in the Greek cohort [16]. Age, gender, ASA grade, cognitive status, and residential status are significant predictor factors for mortality in the Dutch registry, also [17,18]. Although delayed surgery has been shown in cohorts from other countries to be a major contributing factor to higher mortality rates, this association was not observed in the Greek population [19]. The low rates of seeker patients (ASA grade III and above) may have positively affected the mortality rate, counteracting the delays in surgery. Interestingly, only a weak correlation between 30-day mortality and delay in surgery was reported recently from the Spanish registry [16].
The average hospital stay for patients in the Greek cohort was just over 10 days, comparable to durations reported in Scotland, Denmark, Italy, and Spain. In contrast, significantly shorter hospital stays are reported in Sweden, Finland, and the Netherlands, where the average ranges from 4.2 to seven days. On the other end, England, Germany, and Ireland report notably longer hospitalisations, ranging from 15 to 19.5 days [8,16]. Interestingly, the early mobilisation of the patients after surgery had no significant influence on the LOS in the present study, which contradicts the findings of other studies [20]. In Greece, the timing of surgery and the patient’s pre-injury mobility appear to have a significant impact on the length of stay. This correlation is observed in the Spanish registry as well [16]. This highlights a key area for improvement within the Greek healthcare system, prioritising timely surgical intervention as a strategy to reduce hospitalisation duration.
Limitations
Although this study represents the largest Greek cohort to date in terms of patient numbers, the total sample (just over 2,000 patients) remains relatively small when compared to other national registries. The participating hospitals were scattered across the country, mostly located in major cities, but still represent only a small fraction of the national healthcare system. Including a broader and more diverse population would provide a more accurate reflection of the overall Greek healthcare landscape. This study is subject to potential selection bias due to the non-random recruitment of participants, an inherent limitation of all registry studies. Additionally, the findings may have limited external validity, as the sample was drawn from a small number of hospitals, which may differ from other populations in demographic or clinical characteristics. The high incidence of delayed surgeries and their evident impact on length of stay highlight the need to investigate the underlying causes. Addressing these delays presents a clear opportunity for improvements in the national healthcare system.
Conclusions
The introduction of Greece's first national hip fracture registry demonstrates its value as an important tool for assessing the current condition of the country’s healthcare system. Its implementation highlights a systemic shortcoming. Specifically, the low proportion of patients undergoing timely surgical intervention, which leads to significantly prolonged hospital stays. Nevertheless, the 30-day mortality rate remains comparable to that of other European countries. Notably, the high percentage of patients living independently before the injury, along with the significant number who return home after hospitalization, appears to have a positive impact on mortality outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hip fracture registries: utility, description, and comparison Osteoporos Int Sáez-López P Brañas F Sánchez-Hernández N Alonso-García N González-Montalvo JI 115711662820172787295610.1007/s 00198-016-3834-x · doi ↗ · pubmed ↗
- 2Data quality audit of a clinical quality registry: a generic framework and case study of the Australian and New Zealand Hip Fracture Registry BMJ Open Qual Tan AC Armstrong E Close J Harris IA 08201910.1136/bmjoq-2018-000490 PMC 666889831414056 · doi ↗ · pubmed ↗
- 3Alliance for the development of the Argentinian Hip Fracture Registry Arch Osteoporos Monteverde E Diehl M Saieg M 1221720223609888210.1007/s 11657-022-01163-0PMC 9469067 · doi ↗ · pubmed ↗
- 4The impact of a national clinician-led audit initiative on care and mortality after hip fracture in England: an external evaluation using time trends in non-audit data Med Care Neuburger J Currie C Wakeman R 6866915320152617293810.1097/MLR.0000000000000383 PMC 4501693 · doi ↗ · pubmed ↗
- 5Does performance-based remuneration improve outcomes in the treatment of hip fracture?Bone Joint J Griffin XL Achten J Parsons N Costa ML 881887103-B 20213393464910.1302/0301-620X.103B 5.BJJ-2020-1839.R 1PMC 8091000 · doi ↗ · pubmed ↗
- 6Using national hip fracture registries and audit databases to develop an international perspective Injury Johansen A Golding D Brent L 217421794820172880365110.1016/j.injury.2017.08.001 · doi ↗ · pubmed ↗
- 7Incidence and mortality of hip fractures in the United States JAMA Brauer CA Coca-Perraillon M Cutler DM Rosen AB 1573157930220091982602710.1001/jama.2009.1462 PMC 4410861 · doi ↗ · pubmed ↗
- 8Differences in hip fracture care in Europe: a systematic review of recent annual reports of hip fracture registries Eur J Trauma Emerg Surg Werner M Macke C Gogol M Krettek C Liodakis E 162516384820223462347410.1007/s 00068-021-01797-8PMC 9192454 · doi ↗ · pubmed ↗