Effect of Lee Silverman Voice Treatment-BIG Intervention Versus Balance Training via Tele-rehabilitation on Balance and Functional Mobility Among Community-Dwelling Elderly: A Comparative Study
Meghana P Chavan, Priti N Agni

TL;DR
This study compares two tele-rehabilitation methods for improving balance and mobility in elderly people, finding that LSVT-BIG is more effective for functional mobility.
Contribution
The novel contribution is evaluating LSVT-BIG's effectiveness in elderly individuals via tele-rehabilitation compared to traditional balance training.
Findings
Both LSVT-BIG and balance training improved balance and mobility in elderly participants.
LSVT-BIG showed significantly better results in functional mobility compared to conventional training.
Improvements were achieved through tele-rehabilitation, indicating its viability for elderly care.
Abstract
Introduction: Elderly individuals often experience loss of confidence, gait abnormalities, and impaired balance, which can lead to fear of falling and limitations in functional mobility. Lee Silverman Voice Treatment-BIG (LSVT-BIG) addresses balance and activities of daily living (ADLs) in individuals with Parkinson’s disease by training them to increase the amplitude of movements from head to toe. It targets functional mobility through “functional component movements,” in which a specific task is selected and the individual is trained to perform it with large-amplitude movements and then apply it to real-life activities. LSVT-BIG has been shown to improve balance and mobility in Parkinson’s disease, which are also features of the "ageing syndrome." Hence, this study aims to explore its role in the geriatric population, compared with traditional balance training methods, through…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
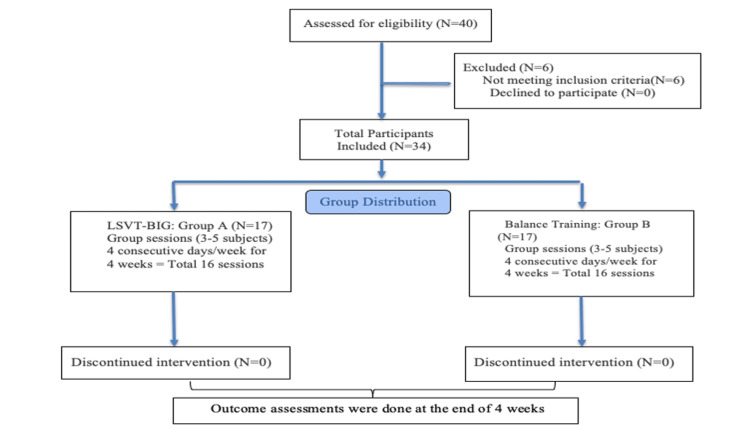 Figure 1
Figure 1 Figure 2
Figure 2| Group A | Intervention |
| Intervention | Lee Silverman Voice Treatment-BIG (LSVT-BIG) |
| Dosage | Four consecutive days per week for four weeks (16 sessions in one month) |
| Session duration | Sixty minutes per session |
| Repetitions | Minimum of 8-12 repetitions per task |
| Effort level | Maximum patient-perceived effort daily (8-9 on a 1-10 scale) |
| Session phase | Task | Exercise | Repetitions/duration |
| First half (45 min) | Task 1: maximum sustained movements (seated) | BIG stretch: floor to ceiling | 8 reps, 10-sec hold |
| BIG stretch: side to side | 8 reps, 10-sec hold | ||
| Task 2: repetitive/directional movements (standing) | Forward BIG step | 16 reps (8 each leg) | |
| Sideways BIG step | 16 reps (8 each leg) | ||
| Backward BIG step | 16 reps (8 each leg) | ||
| Forward BIG rock and reach | 20 reps (10 each leg) | ||
| Sideways BIG rock and reach | 20 reps (10 each leg) | ||
| Task 3: functional component movements | Functional activity components | 5 reps per component | |
| Second half of session (15 min) | Walking component | BIG walking included as part of hierarchy tasks | |
| Group B | Intervention |
| Intervention | Conventional balance training |
| Dosage | Four consecutive days per week for four weeks (16 sessions in one month) |
| Session duration | Sixty minutes per session |
| Repetitions | Minimum of 8-12 repetitions per task |
| Effort level | Maximum patient-perceived effort daily (8-9 on a 1-10 scale) |
| Session component | Duration | Activities/description |
| Warm-up | Five minutes | Stepping exercises: forward and lateral walking at a safe moderate speed. Raising both arms overhead and lowering. Neck exercises: trunk rotations |
| Training (conventional balance exercises) | Fifty minutes (3-4 min/activity) | Marching in place; standing with feet close together; walking forward 10 steps and pivoting 180°; alternate single-leg standing; sit-to-stand from chair with arms crossed; heel raises holding chair; tandem standing; back and side leg raises holding chair; walking forward, sideways, and backward; marching with high leg lift; tandem walking along a line; stepping in different directions; mini wall squats; obstacle walking |
| Cool-down | Five minutes | Forward walking at moderate speed. Joint mobility exercises: raising arms overhead and lowering |
| Exercise progression | Throughout training | Reducing base of support; closing eyes; increasing movement speed; using unstable surfaces (e.g., soft pillow) |
| Age (years) | Group A | Group B |
| Median | 71 | 68 |
| Mean | 71.64 | 69.76 |
| Standard deviation | 5.43 | 5.48 |
| Gender | Number of subjects | Percentage | |
| Group A | Group B | ||
| Females | 8 | 8 | 47 |
| Males | 9 | 9 | 53 |
| Total | 17 | 17 | 100 |
| Mini-BESTest scores | Mean | Std. deviation | N | p-value | Significance | |
| Group A (LSVT-BIG) | Pre | 23.17 | 1.74 | 17 | <0.0001 | Significant |
| Post | 25.05 | 1.56 | 17 | |||
| Group B (CBT) | Pre | 22.82 | 1.74 | 17 | <0.0001 | Significant |
| Post | 24.35 | 1.76 | 17 | |||
| TUG scores | Mean | Std. deviation | N | p-value | Significance | |
| Group A (LSVT-BIG) | Pre | 11.52 | 1.06 | 17 | <0.0001 | Significant |
| Post | 9.88 | 0.92 | 17 | |||
| Group B (CBT) | Pre | 10.76 | 1.30 | 17 | 0.0003 | Significant |
| Post | 9.94 | 1.29 | 17 | |||
| Mini-BESTest score | Mean | Std. deviation | p-value | Significance |
| Group A (LSVT-BIG) | 1.88 | 0.85 | 0.2622 | Not significant |
| Group B (CBT) | 1.52 | 0.94 |
| TUG score | Mean | Std. deviation | p-value | Significance |
| Group A (LSVT-BIG) | -1.64 | 0.86 | 0.0066 | Significant |
| Group B (CBT) | -0.82 | 0.72 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Stroke Rehabilitation and Recovery · Prosthetics and Rehabilitation Robotics
Introduction
In India, there is a rapid increase in the elderly population, which is expected to reach approximately 326 million by 2050. This trend raises increasing concern regarding various socioeconomic and health-related issues [1]. With advancing age, individuals face challenges in maintaining independence and self-confidence while performing activities of daily living (ADLs), despite higher rates of functional decline and disability observed among community-dwelling elderly individuals [2]. ADLs require multiple components of balance, and impairment in these components progressively compromises functional mobility and quality of life (QOL). During normal ageing, physiological changes in the multisensory system affect balance and lead to more fearful movement patterns, thereby influencing the efficiency of functional task performance. Age-related changes in bone density, cartilage integrity, joint flexibility, and proprioception contribute to increased musculoskeletal stiffness and weakness, adversely affecting balance [3]. Additionally, increased displacement and velocity of the center of pressure (CoP) are observed due to poor postural control during tasks requiring both static and dynamic balance. With advancing age, disruption of the sensorimotor control system further affects postural control and balance [4]. This results in impaired mobility and induces a psychological fear of falling, which in turn leads to reduced participation in ADLs among older adults [5]. Therefore, balance training and conventional exercise programs play an important role in improving postural control by enhancing lower-limb strength and joint proprioception, thereby reducing the risk of falls.
Lee Silverman Voice Treatment-BIG (LSVT-BIG) is an intervention originally developed for individuals with Parkinson’s disease (PD) and is derived from the speech treatment LSVT-LOUD, which is used to manage speech deficits such as hypophonia [6]. LSVT-BIG addresses balance and ADLs in PD by training individuals to increase the amplitude of movements from head to toe. It also targets functional mobility through “functional component movements,” wherein a specific task is selected and the individual is trained to perform it using large-amplitude movements, followed by retraining in real-life activities [6]. LSVT-BIG incorporates key principles of motor learning, including high intensity, salience, multiple repetitions, and progressive complexity. These principles facilitate activity-dependent motor learning and neuroplasticity, thereby enhancing movement generalization and automaticity. LSVT-BIG has shown benefits in stroke rehabilitation, and researchers are exploring its application in other neurological conditions [7]. While several interventions such as Tai Chi and various forms of yoga have been explored to improve balance and functional mobility in the elderly, LSVT-BIG may also be effective in addressing balance and mobility impairments seen in Parkinson’s disease, which share similarities with manifestations of the ageing syndrome [7,8]. Hence, this study aims to examine the role of LSVT-BIG in geriatrics and its effects on balance and functional mobility, which are common features of ageing.
Tele-rehabilitation has emerged as a valuable approach in the field of rehabilitation, offering time- and cost-effective healthcare services, particularly for vulnerable populations such as the elderly and individuals with disabilities [9]. It has been utilized in the rehabilitation of various conditions, including stroke, multiple sclerosis, cardiorespiratory disorders, and psychological conditions, and has demonstrated effectiveness in improving quality of life, functional abilities, and reducing long-term symptoms [10]. However, there is limited literature on the effectiveness of tele-rehabilitation in improving balance and functional mobility among community-dwelling elderly individuals.
Thus, this study contributes to the existing literature by examining the role of balance training delivered through tele-rehabilitation in the geriatric population, while also exploring LSVT-BIG as a potential intervention to improve balance and functional mobility in the elderly. The study holds social relevance by promoting healthy ageing and enhancing community participation among older adults.
Materials and methods
This was a comparative study conducted over a period of 18 months among community-dwelling, ambulatory adults aged 65-80 years in a tertiary care physiotherapy outpatient department and community setting. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Institutional ethical approval was obtained prior to study commencement, and written informed consent was obtained from all participants. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Participants were screened based on predefined inclusion and exclusion criteria. Inclusion criteria comprised community-dwelling elderly individuals who were not engaged in structured exercise programs, were accessible for tele-rehabilitation, and had caregiver support during intervention sessions. Exclusion criteria included individuals with medical, neurological, or sensory conditions limiting exercise participation; those with high or minimal fall risk (Mini -Balance Evaluation Systems Test (Mini-BESTest) score <19.5 or ≥28; Timed Up and Go (TUG) test >13.5 seconds); and individuals unwilling to participate.
Sample size was calculated using the OpenEpi website (Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. www.OpenEpi.com, updated 2013/04/06), with a 95% CI and 80% power, accounting for a 10% attrition rate. The required sample size was determined to be 17 participants per group (50%), resulting in a total sample size of 34 participants (100%). Participants were equally allocated to two intervention groups with comparable baseline characteristics.
Figure 1 depicts the study design and participant flow throughout the research process. The study received approval from the Institutional Ethics Committee (IEC), and participants were recruited using convenience sampling from the community. The study procedure was explained in the participants’ preferred language, and informed consent was obtained. Eligible participants were assigned to either Group A (Tables 1, 2) or Group B (Tables 3, 4), with 17 participants in each group. Both interventions were delivered via tele-rehabilitation in small groups. Outcome assessments were conducted offline by the same assessor before and after the intervention to ensure consistency. Balance was assessed using the Mini-BESTest, and functional mobility was assessed using the TUG test. The therapist administering the interventions was certified in the LSVT-BIG method and provided the respective interventions accordingly. During tele-rehabilitation sessions (Figure 2), participants were instructed to exercise in a safe home environment near fixed support surfaces to minimize the risk of falls and were accompanied by a family member for safety. Family members were briefed on the exercise protocol, and instructional videos were provided prior to the sessions. Attendance was monitored throughout the intervention period, and reminders were sent to promote adherence. Post-intervention assessments were conducted by the same assessor.
Participant flow diagram
Therapist’s screen while conducting the session through tele-rehabilitation
Results
Data from 34 participants were collected, recorded in a Microsoft Excel spreadsheet (Microsoft Corp., Redmond, WA, USA), and analyzed using GraphPad Prism software version 9.4.0 (453) (Dotmatics, Boston, MA, USA). Qualitative variables were expressed as absolute numbers and percentages, while quantitative variables were expressed as mean and standard deviation. The Shapiro-Wilk test was used to assess the normality of data distribution (Tables 5, 6). For intra-group analysis, a paired t-test was used to compare pre- and post-intervention Mini-BESTest scores in Group A and Group B, and TUG scores in Group B. As the TUG scores in Group A did not follow a normal distribution, the Wilcoxon signed-rank test was used to compare pre- and post-intervention values in this group (Tables 7, 8). For inter-group analysis, an unpaired t-test was used to compare Mini-BESTest scores between Group A and Group B, while the Mann-Whitney U test was used to compare TUG scores between the two groups (Tables 9, 10). A p-value < 0.05 was considered statistically significant.
Discussion
This is one of the pioneer studies to document and explore the effect of LSVT-BIG on balance and functional mobility in healthy elderly individuals through tele-rehabilitation. The age and gender distribution of participants in both groups were comparable, as shown in Table 5 and Table 6, indicating baseline similarity between the groups. The study demonstrated statistically significant intra-group improvements (Tables 7, 8) in Mini-BESTest and Timed Up and Go (TUG) scores in both Groups A and B. However, no statistically significant inter-group difference was observed in Mini-BESTest scores, as both groups showed comparable improvement in balance (Tables 9, 10).
The modest improvement in balance observed following LSVT-BIG may be attributed to repetitive, high-amplitude daily exercises that emphasize “BIG” movements, static posturing, and enhanced joint mobility, thereby reducing tissue rigidity. The use of exaggerated movements with strong distal sensory input (such as foot stomping and hand slapping) may facilitate sensory recalibration and sustained muscle activation, contributing to improved balance control. Previous work has shown that LSVT-BIG improves proprioceptive performance by recalibrating proprioceptive processing in individuals with PD [11]. In the present study, multidirectional movements such as forward, sideways, and backward BIG stepping, as well as forward rock and reach, may have positively influenced balance, which is commonly affected in community-dwelling elderly individuals due to age-related physiological changes.
LSVT-BIG also demonstrated statistically significant improvements in TUG scores, indicating a positive effect on functional mobility among the elderly. While prior studies have reported improvements in functional mobility following LSVT-BIG in individuals with PD, its effects had not been previously explored in a healthy elderly population [12]. The intervention includes dynamic exercises such as rock and reach, sideways rock and reach, and BIG walking. These exercises resemble normal gait patterns and require coordination between the upper and lower extremities, along with reciprocal ankle dorsiflexion and plantarflexion to facilitate a heel-to-toe walking pattern. The sideways rock and reach exercise is performed bilaterally and may contribute to improved truncal rotation. BIG walking emphasizes high-amplitude walking with increased arm swing and longer step lengths, aiming to override slow and reduced movement patterns [13,14]. BIG sit-to-stand was included as one of the functional component exercises relevant to activities of daily living. Both groups demonstrated statistically significant pre- to post-intervention improvements in balance and functional mobility.
The findings of this study are consistent with previous research examining the effects of functional balance training in the ageing population [3,4]. Studies have shown that functional balance training plays an important role in maintaining and improving functional abilities in older adults [8]. The improvements observed in the present study may be attributed to the multisensory approach adopted, incorporating visual, vestibular, and somatosensory inputs encountered during daily activities, thereby enhancing balance and functional mobility. Lower limb strengthening exercises such as sit-to-stand, wall squats, and heel raises likely contributed to improved functional mobility by enhancing lower limb muscle strength.
The results are also consistent with studies that implemented structured balance programs ranging from 4 to 25 weeks, involving positional variations, directional walking, and sensory challenges, which led to improvements in static and dynamic balance, functional mobility, and a reduction in fear of falling [3,4,8]. The present study, which combined offline assessments with online interventions, demonstrated statistically significant intra-group improvements, suggesting that both LSVT-BIG and conventional balance training delivered through tele-rehabilitation were effective in improving balance and functional mobility in community-dwelling elderly individuals.
A systematic review by Velayati et al. [9] examined the effectiveness of tele-rehabilitation in elderly individuals with chronic health conditions and highlighted the need for further research, as several studies reported outcomes comparable to conventional rehabilitation. This suggests that tele-rehabilitation may serve as an alternative or adjunct to traditional outpatient rehabilitation, reducing resource burden. Similarly, Tyagi et al. [15] concluded that tele-rehabilitation can be utilized for health promotion strategies in the elderly and as a complementary service delivery model. Thus, the present study adds to the growing body of literature supporting the effectiveness of LSVT-BIG delivered through tele-rehabilitation in improving balance and functional mobility in the elderly population.
Limitations
The study was limited by its restricted geographical scope, which may affect the generalizability of the findings. Additionally, age stratification was not performed due to unequal distribution across age groups. Outcome assessments were conducted only at pre- and post-intervention time points, with no follow-up to evaluate long-term or carry-over effects. Furthermore, subjective measures of quality of life were not included, despite the potential psychological benefits of the intervention. These aspects may be considered as future directions for research.
Conclusions
This study concludes that both LSVT-BIG and balance training delivered through tele-rehabilitation significantly improved balance and functional mobility in the elderly population. However, when compared to balance training alone, the LSVT-BIG program demonstrated superior and statistically significant improvements in functional mobility.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Relationship between fear of falling, balance impairment and functional mobility in community dwelling elderly Innov Aging Kumar S Vendhan GV Awasthi S Tiwari M Sharma VP 4852192008 https://d 1wqtxts 1xzle 7.cloudfront.net/69505447/Relationship_Between_Fear_of_Falling_Bal 20210912-29244-ydj 9b 0.pdf?1738424263=&response-content-disposition=inline%3B+filename%3D Relationship_Between_Fear_of_Falling_Bal.pdf&Expires=1768807302&Signature=Pcbn Ofn 66Dta 7z BG 9DT 5a DVEGK Ymu 6Lk 7cr ARF 2Et 7DX 41su PEK 5Ino Jh ZOO 7h~k 40lg Ek~CCL Ob
- 2A study on correlation between depression, fear of fall and quality of life in elderly individuals Int J Res Med Sci Mishra N al Int J Res Med Sci Mishra N Mishra AK Bidija M 1456146052017 https://www.msjonline.org/index.php/ijrms/article/view/3088
- 3The effect of balance and coordination exercises on quality of life in older adults: a mini-review Front Aging Neurosci Dunsky A 318112019 https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2019.00318/full?TB_iframe=true&width=921.6&height=921.63180304810.3389/fnagi.2019.00318 PMC 6873344 · doi ↗ · pubmed ↗
- 4Balance performance is task specific in older adults Biomed Res Int Dunsky A Zeev A Netz Y 69870172017 https://onlinelibrary.wiley.com/doi/pdf/10.1155/2017/69870172901881710.1155/2017/6987017 PMC 5605868 · doi ↗ · pubmed ↗
- 5Age-related changes in the structure and function of skeletal muscles Clin Exp Pharmacol Physiol Faulkner JA Larkin LM Claflin DR Brooks SV 10911096342007 https://onlinelibrary.wiley.com/doi/pdfdirect/10.1111/j.1440-1681.2007.04752.x?casa_token=v-Hx Zt 88ph EAAAAA:NG 3hpa 6y R Po 5zm Z Tw 3of Pt O 1l T Mvu Sz A-4xhiu HU Ic 6gk Zhkdahf 3g E 56T 6k 85ajet U 5Ms DS Zux Ve TP 7A 5E 1788035910.1111/j.1440-1681.2007.04752.x · doi ↗ · pubmed ↗
- 6The JFK BIG study: the impact of LSVT BIG® on dual task walking and mobility in persons with Parkinson’s disease Brain Behav Isaacson S O’Brien A Lazaro JD Ray A Fluet G 636641302018 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5909018/10.1589/jpts.30.636PMC 590901829706722 · doi ↗ · pubmed ↗
- 7Outcomes following LSVT BIG in a person with idiopathic normal pressure hydrocephalus: a case report J Neurol Phys Ther Fillmore S Cavalier G Franke H Hajec M Thomas A Moriello G 2202274420203251630210.1097/NPT.0000000000000319 · doi ↗ · pubmed ↗
- 8Comparison between tai chi and balance-strength training exercise to decrease fear of fall and improving balance and functional mobility in elderly J Novel Physiother Kumar C 35072017 https://www.researchgate.net/publication/318438176_Comparison_between_Tai_Chi_and_Balance-Strength_Training_Exercise_to_Decrease_Fear_of_Fall_and_Improving_Balance_and_Functional_Mobility_in_Elderly