Sudden Cardiac Arrest in Proximal Femur Fracture: The Role of Admission Blood Parameters
Hüseyin Aldemir

TL;DR
An elderly patient with a hip fracture suddenly died from cardiac arrest, highlighting the importance of admission blood parameters in predicting risk.
Contribution
This case emphasizes the clinical significance of elevated neutrophil-to-lymphocyte ratio and hyponatremia as early indicators of mortality risk in elderly hip fracture patients.
Findings
Elevated NLR and hyponatremia on admission were associated with sudden cardiac arrest in a geriatric hip fracture patient.
Sudden PEA arrest in ED may be linked to undiagnosed pulmonary embolism or fat embolism syndrome.
Early mortality can occur before surgery in high-risk geriatric hip fracture patients.
Abstract
Proximal femur fractures in the elderly are associated with high mortality rates due to reduced physiological reserve and a high risk of thromboembolic events, where admission laboratory parameters can serve as early indicators of clinical vulnerability. This case highlights a catastrophic clinical deterioration in a 92-year-old man who was admitted following a fall resulting in a displaced right intertrochanteric fracture. On admission, the patient was hemodynamically stable, but laboratory findings revealed an elevated neutrophil-to-lymphocyte ratio (NLR) of 10.1 and significant hyponatremia (126 mmol/L), reflecting high physiological stress and reduced compensatory reserve. Approximately 10 hours after admission, during preoperative preparation, he developed sudden dyspnea, hypotension, and pulseless electrical activity (PEA). Despite 30 minutes of advanced cardiac life support, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
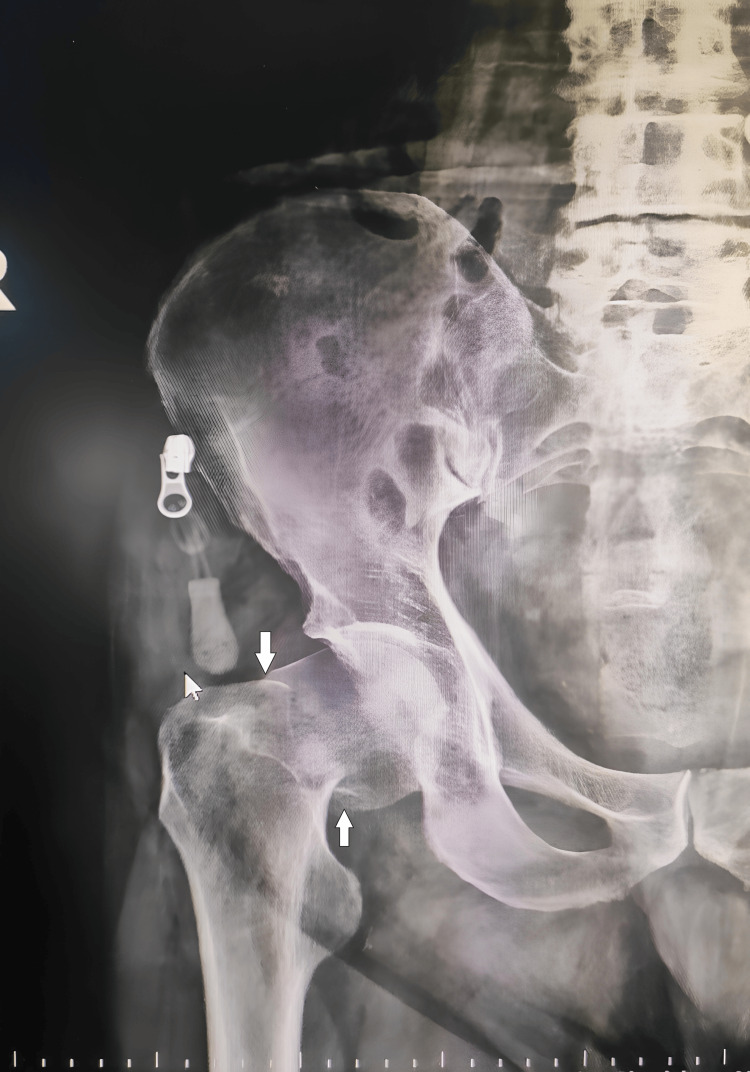 Figure 1
Figure 1| Laboratory parameter | Admission value | Reference range |
| Hemoglobin | 9.6 g/dL | 13.5-17.5 g/dL |
| White blood cell count | 13.9 × 10⁹/L | 4.5-11.0 × 10⁹/L |
| Neutrophil count | 11.1 × 10⁹/L | 2.0-7.0 × 10⁹/L |
| Lymphocyte count | 1.1 × 10⁹/L | 1.0-3.0 × 10⁹/L |
| Neutrophil-to-lymphocyte ratio (NLR) | 10.1 | 1.0-3.0 |
| Serum sodium | 126 mmol/L | 135-145 mmol/L |
| Serum creatinine | 1.4 mg/dL | 0.7-1.3 mg/dL |
| Blood urea nitrogen (BUN) | 42 mg/dL | 7-20 mg/dL |
| C-reactive protein (CRP) | 19.4 mg/L | <5 mg/L |
| Arterial blood gas analysis parameter | Admission (stable) | During cardiac arrest (PEA) | Reference range |
| pH | 7.38 | 6.98 | 7.35-7.45 |
| PaO₂ | 86 mmHg | 42 mmHg | 80-100 mmHg |
| PaCO₂ | 40 mmHg | 58 mmHg | 35-45 mmHg |
| HCO₃⁻ | 24 mmol/L | 13 mmol/L | 22-26 mmol/L |
| Lactate | 1.9 mmol/L | 11.8 mmol/L | 0.5-2.2 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Bone fractures and treatments · Nutrition and Health in Aging
Introduction
Proximal femur fractures in elderly patients represent a major public health challenge, frequently associated with significant early mortality and a high burden of comorbidities [1,2]. These injuries often trigger a systemic inflammatory response, leading to life-threatening thromboembolic and cardiopulmonary complications such as massive pulmonary embolism (PE) and fat embolism syndrome (FES) [3,4]. Studies have shown that the risk of fatal PE is particularly high within the first 24-48 hours of injury, often occurring before surgical stabilization can be achieved [4]. Furthermore, admission laboratory markers, including the neutrophil-to-lymphocyte ratio (NLR) and serum sodium levels, may reflect the patient's underlying physiological stress and reduced compensatory reserve, which are recognized as predictors of mortality in geriatric trauma patients [5,6]. Identifying these high-risk patients upon emergency department (ED) admission is vital, as sudden clinical deterioration may lead to a diagnostic challenge, especially when symptoms of PE and FES overlap [1-3].
Case presentation
A 92-year-old male patient was brought to the ED after a fall from standing height at home. He had been fully ambulatory prior to the fall. There was no known history of cardiovascular disease, malignancy, anticoagulant use, or recent immobilization. On admission, the patient was conscious, cooperative, and oriented. Vital signs were stable with a blood pressure of 140/85 mmHg, heart rate of 90 beats/min, respiratory rate of 18 breaths/min, oxygen saturation of 96% on room air, and body temperature of 36.6°C. Electrocardiography showed a normal sinus rhythm. Physical examination revealed pain, shortening, and external rotation of the right lower extremity. Pelvic radiography demonstrated a displaced right intertrochanteric fracture (Figure 1).
Anteroposterior pelvic radiograph showing a displaced right intertrochanteric fracture
Initial laboratory evaluation at ED admission revealed several abnormal blood parameters (Table 1).
During the preoperative evaluation and clinical preparation process, the patient remained under observation in the ED, while preoperative anesthesia evaluation and surgical preparation were initiated.
Approximately 10 hours after admission, during preoperative preparation, the patient suddenly developed acute dyspnea and hypotension, followed rapidly by loss of consciousness. The cardiac monitor revealed pulseless electrical activity (PEA). Immediate cardiopulmonary resuscitation was initiated according to advanced cardiac life support protocols. Despite 30 minutes of resuscitative efforts, return of spontaneous circulation could not be achieved. In contrast to the initial arterial blood gas analysis, the analysis obtained during cardiac arrest demonstrated severe hypoxemia, hypercapnia, and profound metabolic acidosis accompanied by markedly elevated lactate levels, consistent with severe tissue hypoperfusion (Table 2).
Discussion
Early mortality following proximal femur fractures remains a significant clinical concern, particularly in elderly patients [1,2]. Delays in surgical management and early physiological derangements have been associated with adverse short-term outcomes after hip fractures [2-4]. Admission laboratory abnormalities may help identify patients with limited physiological reserve in this vulnerable population [5,6]. Specifically, elevated NLR and electrolyte imbalances, such as hyponatremia, as seen in our patient, should be viewed as risk indicators of clinical frailty rather than direct predictors of acute embolic events [1,7]. In the present case, the patient demonstrated multiple abnormal laboratory findings at ED admission despite being hemodynamically stable and fully conscious. The sudden clinical deterioration characterized by acute dyspnea and PEA suggests an acute obstructive cause of cardiac arrest rather than a primary cardiac etiology. Massive PE was considered a potential clinical hypothesis among other differential diagnoses, given the abrupt onset of respiratory compromise, rapid hemodynamic collapse, severe hypoxemia, and refractory PEA arrest. Elderly patients with lower extremity fractures may be at increased risk of thromboembolic complications, even in the early post-injury period [4]. FES was also considered in the differential diagnosis. Although FES is more commonly reported 12-72 hours after injury, early presentations have been described, particularly in elderly patients with long bone or proximal femur fractures [3]. Although the classic triad was not fully present, FES cannot be definitively excluded. Fulminant forms of FES have been described where rapid cardiac arrest occurs without petechial rash or neurological findings. Therefore, a more balanced comparison must be made, as both massive PE and early-onset FES are plausible causes for such a catastrophic collapse [3,4]. This case highlights the diagnostic challenges faced in the ED when catastrophic deterioration occurs before definitive imaging can be obtained. In the absence of confirmatory evidence, such as D-dimer levels, CT pulmonary angiography, bedside echocardiography, or a post-mortem examination, the diagnosis of massive PE or FES remains speculative and unconfirmed.
Conclusions
In conclusion, proximal femur fractures in geriatric patients carry a significant risk of sudden, catastrophic complications that may occur even before surgical intervention. While admission laboratory parameters, specifically an elevated NLR and hyponatremia, are associated with increased mortality, they should be interpreted as risk indicators reflecting a compromised physiological reserve rather than direct predictors of acute embolic events. In cases of sudden cardiovascular collapse, massive PE and FES represent a formidable diagnostic challenge. However, in the absence of confirmatory imaging, D-dimer levels, or autopsy findings, the definitive etiology in this case remains a speculative and unconfirmed diagnosis. This report underscores the necessity of maintaining a high clinical suspicion for both PE and FES in the emergency department, as these events can lead to rapid clinical deterioration in patients with limited compensatory mechanisms, even when a definitive diagnostic conclusion cannot be reached.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frailty as a determinant of mortality, surgical timing and hospital stay in proximal femur fractures: a retrospective cohort study Eur J Orthop Surg Traumatol Comodo RM Di Gialleonardo E Bocchino G 1963520254036936910.1007/s 00590-025-04312-6PMC 12078435 · doi ↗ · pubmed ↗
- 2Unveiling the hidden risks: 90-day mortality and complications in older adults with proximal femur fractures Aging Clin Exp Res Roitzsch C Beyer F Schaser KD Riedel R Mäder M Postler A 2203720254068274910.1007/s 40520-025-03134-0PMC 12276096 · doi ↗ · pubmed ↗
- 3Incidence of fat embolism syndrome in femur fractures and its associated risk factors over time-a systematic review J Clin Med Lempert M Halvachizadeh S Ellanti P Pfeifer R Hax J Jensen KO Pape HC 27331020213420570110.3390/jcm 10122733 PMC 8234368 · doi ↗ · pubmed ↗
- 4Timing of pulmonary embolisms in femur fracture patients: Incidence and outcomes J Trauma Acute Care Surg Kim YJ Choi DH Ahn S Sohn CH Seo DW Kim WY 952956802016 https://journals.lww.com/jtrauma/abstract/2016/06000/timing_of_pulmonary_embolisms_in_femur_fracture.17.aspx 2689116110.1097/TA.0000000000001014 · doi ↗ · pubmed ↗
- 5Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study BMJ Roche JJ Wenn RT Sahota O Moran CG 137433120051629901310.1136/bmj.38643.663843.55PMC 1309645 · doi ↗ · pubmed ↗
- 6Neutrophil-to-lymphocyte ratio for predicting postoperative mortality after hip fracture surgery: a systematic review and meta-analysis J Orthop Surg Res Liu C Zheng J Bai Y Gan L Gu Y 10722020254140290010.1186/s 13018-025-06495-4PMC 12706907 · doi ↗ · pubmed ↗
- 7The incidence of hyponatremia in hospitalized patients due to hip fracture and its effect on mortality Cukurova Med J Kayaokay K Arslan Yurtlu D 601606482023 https://dergipark.org.tr/en/pub/cumj/article/1284848