Thoracoscopic-guided paraesophageal abscess drainage in foreign body-induced esophageal perforation: a case report
Mu-Chou Lin, Ying-Yuan Chen

TL;DR
A 76-year-old woman with a contained mediastinal abscess from an esophageal perforation was successfully treated with thoracoscopically guided drainage, avoiding major surgery.
Contribution
Demonstrates the safety and efficacy of thoracoscopic-guided drainage for contained mediastinal abscesses in esophageal perforation.
Findings
Thoracoscopic-guided percutaneous drainage achieved source control without pleural contamination.
The patient recovered fully with complete healing of the esophageal perforation.
This approach offers an organ-preserving option for selected cases of contained mediastinal abscesses.
Abstract
Esophageal perforation is a life-threatening emergency, especially when diagnosis is delayed or when the thoracic esophagus is involved. Controlling mediastinal contamination is critical, yet the optimal drainage strategy for contained mediastinal abscesses remains controversial. We report the case of a 76-year-old woman with a foreign body-induced lower thoracic esophageal perforation complicated by a contained paraesophageal abscess. After endoscopic removal of an impacted blister pack, primary repair was not feasible due to severe inflammation and friable tissue. Video-assisted thoracoscopic exploration revealed an intact mediastinal pleura with a localized abscess. Thoracoscopically guided percutaneous drainage using a 14-Fr pigtail catheter was performed to achieve source control while avoiding uncontrolled pleural contamination. The patient recovered uneventfully, with complete…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
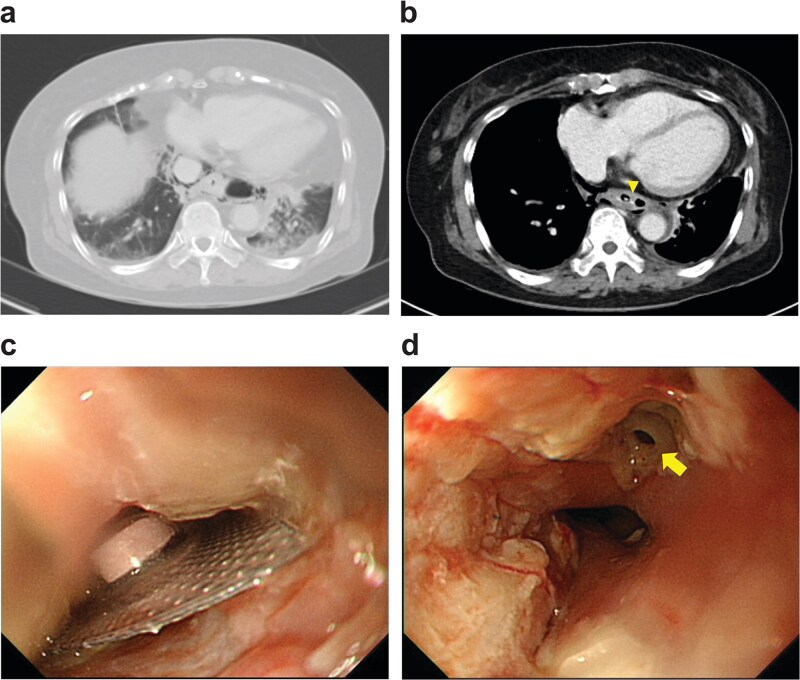 Figure 1
Figure 1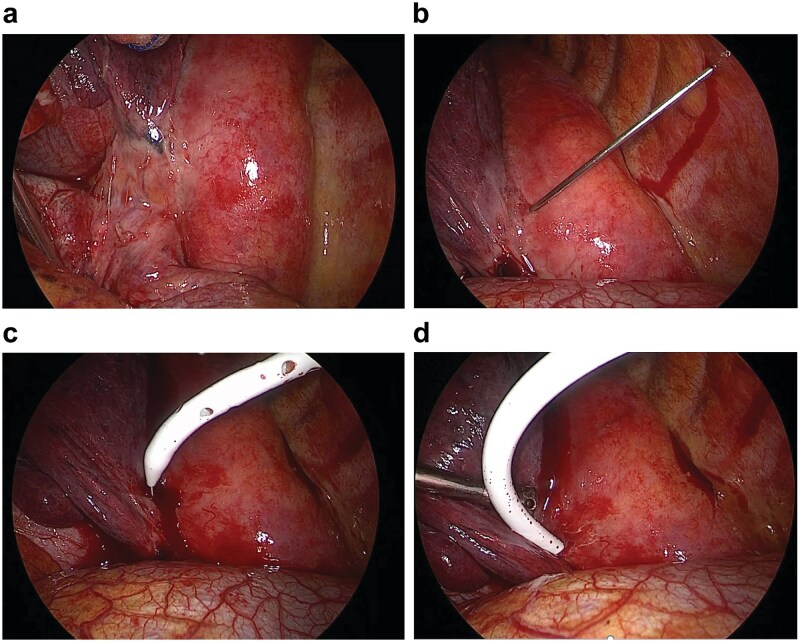 Figure 2
Figure 2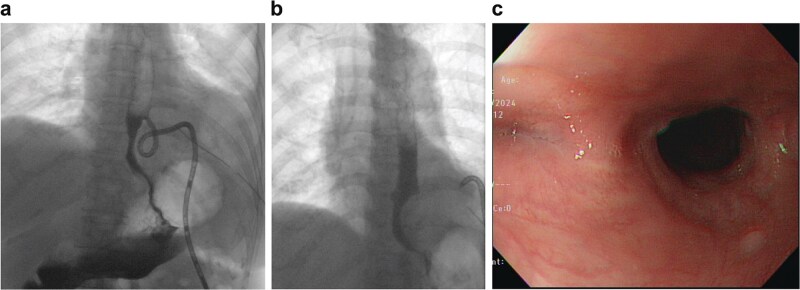 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Pneumothorax, Barotrauma, Emphysema
Introduction
Esophageal perforation is an uncommon but potentially life-threatening condition, particularly with delayed diagnosis or thoracic involvement. Mortality remains high and is largely determined by the extent of mediastinal or pleural contamination and adequacy of source control [1, 2]. Although early primary repair is considered standard, delayed presentation often necessitates alternative strategies focused on infection control and nutritional support [3, 4].
Fundamental management principles include prompt pleural and mediastinal drainage, eradication of infection with broad-spectrum antibiotics, and enteral nutritional support [2, 5]. While nonoperative management may be feasible in selected patients, operative intervention is frequently required to achieve reliable source control [3].
The optimal drainage strategy for localized mediastinal abscesses remains controversial. Conventional incision and drainage may disrupt an initially contained infection, whereas endoscopic or computed tomography (CT)-guided percutaneous drainage is limited by restricted visualization and procedural control [6, 7]. In patients with preserved mediastinal pleural integrity, thoracoscopically guided drainage may provide an organ-preserving alternative. We report a case of foreign body-induced lower thoracic esophageal perforation complicated by a contained paraesophageal abscess, successfully managed using this approach.
Case report
A 76-year-old woman with a history of gastroesophageal reflux disease and gastric mucosa-associated lymphoid tissue lymphoma under regular surveillance presented to the emergency department with epigastric pain and progressive dysphagia over 2 days. On arrival, her vital signs were stable, including a temperature of 37.3°C, heart rate of 95 beats/min, respiratory rate of 20 breaths/min, and blood pressure of 127/71 mmHg.
Upright chest radiography demonstrated a retrocardiac air pocket located between the T10 vertebral level and the descending aorta. Chest computed tomography (Fig. 1a and b) revealed a radiopaque foreign body lodged in the lower thoracic esophagus, approximately 3 cm above the esophagogastric junction, accompanied by pneumomediastinum and a small left pleural effusion. These findings raised strong concern for foreign body-induced esophageal perforation with mediastinal infection or early empyema. Following multidisciplinary consultation with the gastroenterology team, emergency surgical intervention under general anesthesia was undertaken.
(a) Lung and (b) mediastinal windows show a radiopaque foreign body lodged in the lower thoracic esophagus (arrow tip). (c) Esophagogastroduodenoscopy reveals an impacted blister pack in the lower thoracic esophagus. (d) A 4 × 4 mm perforation visible after the blister was removed (solid arrow).
Esophagogastroduodenoscopy identified an impacted blister pack in the lower thoracic esophagus (Fig. 1c), which was removed using endoscopic forceps. A 4 × 4 mm perforation with an acutely suppurative base was visualized at 35 cm from the incisors (Fig. 1d). Although the defect was small, the surrounding tissue was severely inflamed and friable, rendering primary or reinforced repair unfeasible. Given concern for mediastinal contamination, left-sided video-assisted thoracoscopic surgery (VATS) was performed for definitive evaluation and source control.
Upon entry into the pleural cavity, a small volume of freely flowing turbid effusion was aspirated. Inspection of the posterior mediastinum revealed a focal, tense bulge along the left posteroinferior aspect of the esophagus (Fig. 2a), corresponding to the paraesophageal abscess identified on preoperative CT. The mediastinal pleura appeared intact, with no evidence of gross perforation or disruption.
Video-assisted thoracoscopy. (a) Focal, tense bulging mass along the lower esophagus. (b–d) 14-Fr pigtail catheter introduced into the abscess cavity using the Seldinger technique.
To avoid creating a wide communication between the pleural space and the abscess cavity, a thoracoscopically guided percutaneous drainage strategy was chosen. Under direct thoracoscopic visualization, an 18-gauge Chiba needle was advanced into the bulging mediastinal lesion, yielding purulent material. A 14-Fr pigtail catheter (Cook Incorporated, Bloomington, USA) was then inserted using the Seldinger technique and advanced into the abscess cavity (Fig. 2b–d, Video 1), with continuous purulent return confirming correct placement. Residual purulent material was evacuated, and the pleural cavity was irrigated with 3000 ml of sterile normal saline until the effluent was clear.
Two 24-Fr chest tubes were placed before wound closure—one in the posterior costophrenic gutter and the other adjacent to the pigtail catheter—to facilitate postoperative drainage and monitoring. A feeding jejunostomy was constructed to ensure enteral nutrition.
Postoperatively, the patient was kept nil per os, with continuous negative-pressure drainage via a vacuum reservoir connected to the pigtail catheter. Enteral feeding was initiated on postoperative day (POD) 3. Oral contrast esophagography on POD 30 (Fig. 3a) showed minimal contrast drainage through the pigtail catheter without extravasation, consistent with a controlled fistula. The catheter was gradually withdrawn. On POD 49, repeat imaging revealed a small residual blind-ending mediastinal pouch without evidence of leakage (Fig. 3b). The pigtail catheter was removed on POD 52. At 3-month follow-up, endoscopy confirmed complete healing without stricture formation (Fig. 3c), and the patient resumed a normal diet.
(a) Oral contrast esophagography on POD 30. (b) Oral contrast esophagography on POD 49. (c) Three-month follow-up endoscopy confirmed complete healing without stricture formation.
Discussion
Management of esophageal perforation remains challenging, and therapeutic decisions should be individualized based on clinical status, imaging findings, and intraoperative assessment [2, 4]. Nonoperative management may be appropriate in selected patients with early-detected, instrument-related perforations, minimal symptoms, and well-contained mediastinal infection without distal obstruction [2, 3]. Adjunctive endoscopic clipping, stent placement, or endoluminal vacuum therapy have expanded options but remain limited by risks of migration, incomplete sealing, and reduced procedural control in contaminated fields [7].
In this case, endoscopic foreign body removal under general anesthesia allowed controlled extraction while minimizing the risk of exacerbating the esophageal defect. VATS provided direct visualization of the mediastinum and pleural cavity, enabling real-time assessment of contamination and selection of an appropriate drainage strategy. When infection remains localized, targeted drainage may suffice, whereas extensive mediastinal or pleural contamination necessitates more aggressive interventions, including wide debridement, pleural decortication, esophageal diversion, or T-tube placement. Given the anticipated need for prolonged fasting, enteral feeding access was essential to maintain nutritional status and avoiding long-term parenteral nutrition.
Thoracoscopic drainage of mediastinal abscesses secondary to esophageal perforation has been reported only sporadically. Chung and Ritchie described successful thoracoscopic drainage of a giant mediastinal abscess from cervical esophageal perforation using two 32-Fr chest tubes, resulting in survival of a patient with fulminant sepsis [8]. Subsequent reports have also documented favorable outcomes using thoracoscopic approaches in selected cases [9, 10]. In our case, a 14-Fr pigtail catheter was chosen to achieve controlled drainage. Compared with large-bore chest tubes, pigtail catheters are less prone to dislodgement, and Seldinger placement minimizes the risk of creating a large defect in the abscess wall. Prior CT-guided series have shown that small-caliber catheters can provide effective mediastinal abscess drainage [6].
Thoracoscopic-guided catheter placement offers additional advantages over CT-guided drainage, including avoidance of transgressing lung parenchyma and allow direct surgical control. When mediastinal pleural integrity is preserved and the abscess is well localized, this approach represents a feasible, organ-preserving option within a structured decision-making framework.
Supplementary Material
Video_1_rjag189
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbas G, Schuchert MJ, Pettiford BL et al. Contemporaneous management of esophageal perforation. Surgery 2009;146:749.19789035 10.1016/j.surg.2009.06.058 · doi ↗ · pubmed ↗
- 2Brinster CJ, Singhal S, Lee L et al. Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004;77:1475–83.15063302 10.1016/j.athoracsur.2003.08.037 · doi ↗ · pubmed ↗
- 3Altorjay Á, Kiss J, Vörös A et al. Nonoperative Management of Esophageal Perforations. Ann Surg 1997;225:415–21.9114801 10.1097/00000658-199704000-00011 PMC 1190750 · doi ↗ · pubmed ↗
- 4Chirica M, Champault A, Dray X et al. Esophageal perforations. J Visc Surg 2010;147:e 117–28. 10.1016/j.jviscsurg.2010.08.00320833121 · doi ↗ · pubmed ↗
- 5Cameron JL, Kieffer RF, Hendrix TR et al. Selective nonoperative management of contained intrathoracic esophageal disruptions. Ann Thorac Surg 1979;27:404–8.110275 10.1016/s 0003-4975(10)63335-8 · doi ↗ · pubmed ↗
- 6Arellano RS, Gervais DA, Mueller PR. Computed tomography–guided drainage of mediastinal abscesses: clinical experience with 23 patients. J Vasc Interv Radiol 2011;22:673.21439848 10.1016/j.jvir.2011.01.427 · doi ↗ · pubmed ↗
- 7D’Cunha J, Rueth NM, Groth SS et al. Esophageal stents for anastomotic leaks and perforations. J Thorac Cardiovasc Surg 2011;142:39.21683837 10.1016/j.jtcvs.2011.04.027 · doi ↗ · pubmed ↗
- 8Chung DA, Ritchie AJ. Videothoracoscopic drainage of mediastinal abscess: an alternative to thoracotomy. Ann Thorac Surg 2000;69:1573–4.10881846 10.1016/s 0003-4975(00)01189-9 · doi ↗ · pubmed ↗