Digital Medicine and Artificial Intelligence in Chronic Myeloid Leukemia: Current Applications, Challenges, and Future Directions
Chingiz Asadov, Aytan Shirinova, Zohra Alimirzoyeva, Aypara Hasanova

TL;DR
AI and digital tools are transforming CML care by improving diagnosis, treatment, and personalized medicine, but challenges like data quality and patient trust must be addressed.
Contribution
This review systematically examines AI applications in CML and highlights the need for ethical, validated, and patient-centered AI integration.
Findings
AI/ML improves diagnostic accuracy in hematology through cytomorphology and flow cytometry.
Multimodal ML frameworks enhance disease classification and outcome prediction in CML.
Robust validation and MLDevOps infrastructure are critical for safe AI clinical integration.
Abstract
Chronic myeloid leukemia (CML) has become a paradigm for targeted therapy with BCR-ABL1 tyrosine kinase inhibitors (TKIs). However, the growing volume and complexity of clinical, molecular, and imaging data challenge traditional decision-making based on static risk scores. Digital health technologies and artificial intelligence (AI) offer new opportunities to enhance diagnosis, risk stratification, and treatment personalization in CML. This narrative review is based on a focused literature search in PubMed/MEDLINE and Web of Science (2010-2025), combined with expert selection of pivotal studies in CML, digital health, and AI. We included peer-reviewed original research and reviews describing applications of digitalization, AI, or machine learning (ML) in CML or closely related hematologic malignancies, as well as key publications on ethics, regulation, patient perspectives, and ML…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
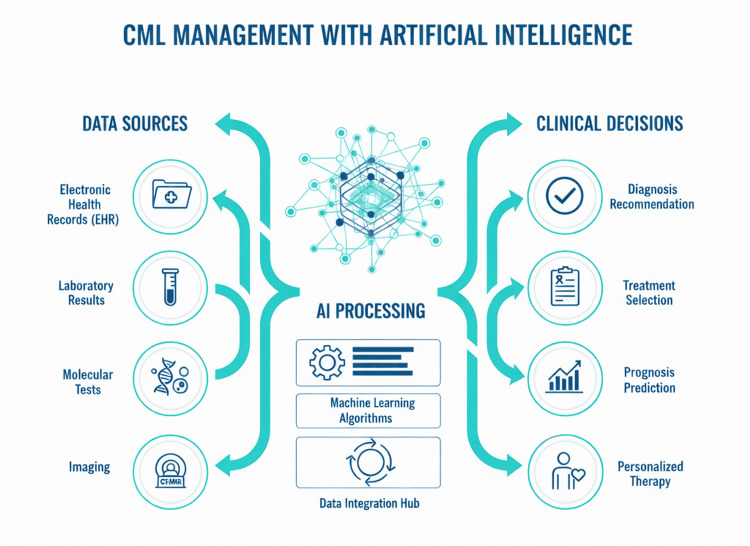 Figure 1
Figure 1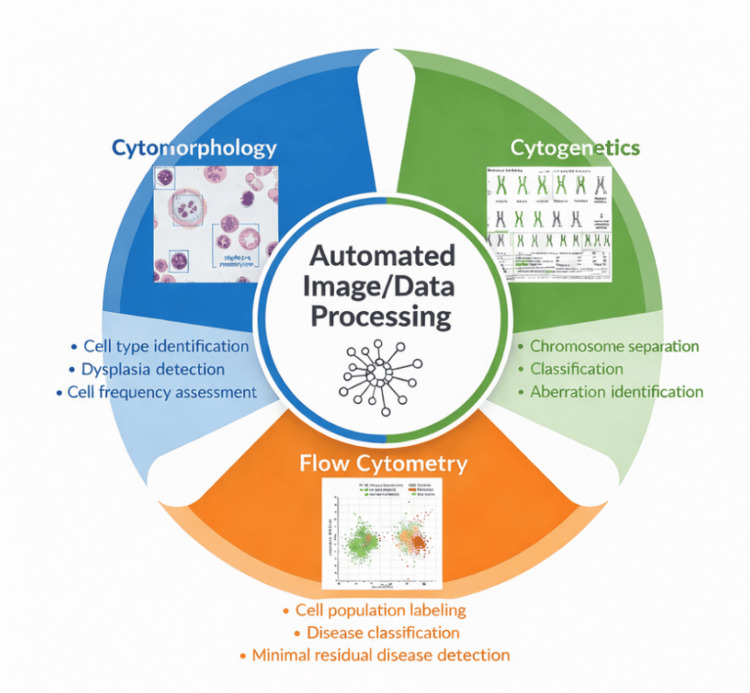 Figure 2
Figure 2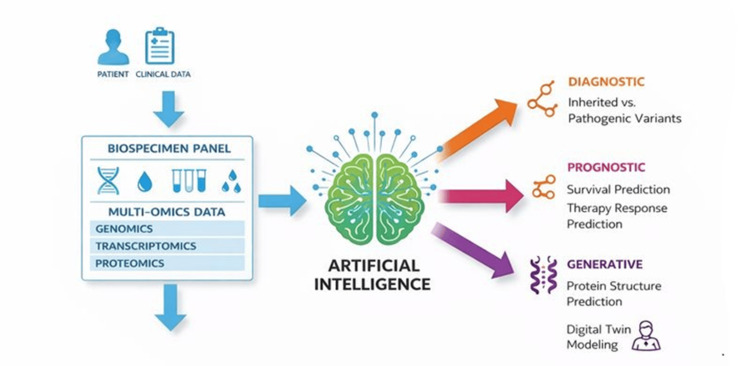 Figure 3
Figure 3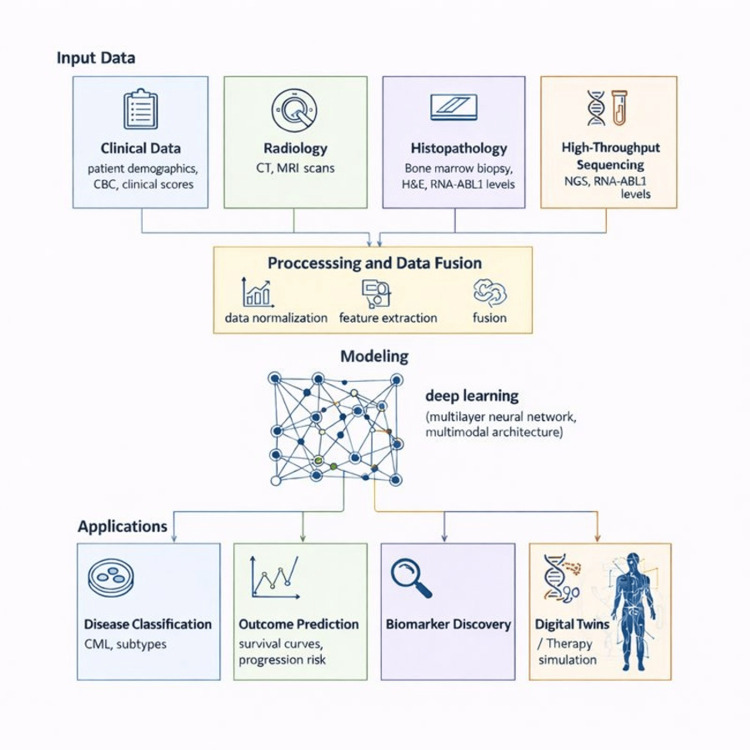 Figure 4
Figure 4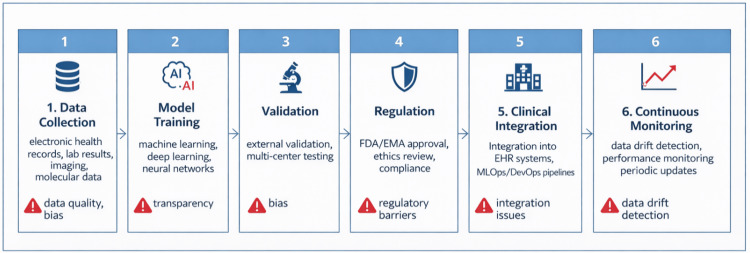 Figure 5
Figure 5| Category | Key Algorithms/Models | Data Input Types | Clinical Application | Key Benefit |
| Diagnostics | CNNs (e.g., ResNet), deep learning | Blood/marrow smears, cytogenetics | Automated cell counting, blast detection | Reduced subjectivity, expert-level speed |
| Prognostics | LEAP, Random Forest, XGBoost | EHR, molecular status, age | Predicting DMR and treatment failure | Higher accuracy than Sokal/ELTS scores |
| Monitoring | Ghost cytometry, trend analysis | Flow cytometry, PCR dynamics | Label-free cell detection, recurrence risk | Ultra-early detection of relapse |
| Drug discovery | Graph neural networks, deep learning | Chemical libraries, genomics | Identifying new TKIs, overcoming resistance | Accelerated in silico screening |
| Maintenance | MLDevOps frameworks | Real-time clinical data | Continuous model monitoring | Ensuring reliability and safety in practice |
| Tool Name | Manufacturer | Primary Function | Hematology Application | Regulatory Status | Notes |
| DiffMaster™ Octavia | MetaSystems GmbH (Germany) | Automated blood smear analysis (leukocyte differential) | Leukocyte classification, blast detection, leukemia screening (incl. CML) | CE-mark (EU) | ~95% accuracy for differentials |
| Morphogo System | Sinovation Ventures (China) | Digital bone marrow morphology | Bone marrow cell classification, dysplasia detection | CE-mark | High-accuracy bone marrow cell ID |
| CellaVision DM Series | CellaVision AB (Sweden) | Automated blood smear analysis | Differential counting, anomaly flagging (leukemias, MDS) | FDA 510(k), CE-mark | Widely used; >95% accuracy on normal samples |
| KaryoXpert | (Research development) | Automated chromosome segmentation & classification | Cytogenetic karyotyping (Ph+ chromosome in CML) | In development | No manual labeling needed |
| Epic Sepsis Model (CDSS) | Epic Systems (USA) | Sepsis prediction in EHR | Monitoring complications in CML patients on TKIs | FDA-cleared (criticized) | Failure example: poor external validity |
| LEAP (Leukemia AI Program) | MD Anderson Cancer Center (USA) | TKI response prediction | Optimal TKI selection in CML (imatinib/dasatinib etc.) | Research platform | AUC ~0.82; improves survival |
| PathAI | PathAI Inc. (USA) | Digital bone marrow pathology | MDS/leukemia classification from biopsies | FDA-cleared (some oncology) | Transferable to CML; genetics correlation |
| Mindpeak APAS® Dx | Mindpeak (Germany) | Blood/bone marrow smear analysis | Leukemia cell classification | CE-mark | AML/ALL/CML diagnosis; >90% sensitivity |
| Method/Technology | Task/Application | Key Results/Metrics | Source/Notes |
| CNN | AML/ALL/CML classification based on bone marrow morphology | High accuracy in CML classification | Huang et al. [ |
| Deep adversarial learning | CML diagnosis from bone marrow images | High accuracy in detecting characteristic features | Zhang et al. [ |
| AI-automated leukocyte differential | Automated peripheral blood differential counting (>10,000 samples) | Near-expert performance | Haferlach et al. [ |
| Ghost cytometry + AI | Label-free detection of CML cells | Strong correlation with BCR-ABL1 levels (IS) | Suzuki et al. [ |
| CNN/SVM/K-means/watershed | Cell segmentation and classification in smears | Accuracy >95–98% | Dese et al. [ |
| Deep learning on flow cytometry | Automated MRD assessment and classification | Hematologist-level accuracy | Matek et al. [ |
| Method/Algorithm | Task/Predicted Outcome | Key Variables/Features | Results/Metrics | Source/Notes |
| Classification and Regression Trees (CART) | Achieving MMR (MR3.0) by 24 months on imatinib | Clinical + molecular + peripheral blood parameters | PPV ~73–96%; higher specificity than some traditional scores | Banjar et al. [ |
| Extreme Gradient Boosting (XGBoost) / LEAP-style modeling | Optimal TKI selection (e.g., imatinib/dasatinib/nilotinib/ponatinib) | Large baseline feature set (multivariable clinical/lab) | Improved outcomes with AI-guided therapy; AUC ~0.82 reported for LEAP | Sasaki et al. [ |
| Multiple ML algorithms (eight models) | 5-year survival prediction | Clinical and laboratory data | Superior performance vs. traditional scores (reported) | Shanbehzadeh et al. [ |
| Neural networks/SVM (conceptual multi-factorial ML) | Molecular response, TFR success, progression risk | Drug transporter polymorphisms (e.g., OCT1/ABCB1), miRNAs, BCR-ABL1 kinetics | Improved stratification vs. single-score approaches (reported across studies) | Examples include transporter/immune/kinetics studies [ |
| Multimodal ML/polygenic modeling | DMR prediction; TFR probability; relapse risk post-discontinuation | Clinical + genomic + BCR-ABL1 kinetics (± immune markers) | Early/ongoing evidence; personalization potential | Transcriptomic ML approach (abstract) [ |
| Classical multivariable models (Cox regression) | TFR outcome prediction | Duration of TKI, depth/stability of MR, baseline risk | Modest discrimination (c-index ~0.63–0.68 reported) | EURO-SKI [ |
| Genomic/biomarker-enhanced predictors (under ML development) | Enhanced TFR prediction | Transcript type (e13a2/e14a2), kinetics, immunophenotype | Signal for improved prediction; ML models require validation | Kinetics and biomarkers [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Myeloid Leukemia Treatments · Digital Imaging for Blood Diseases · Artificial Intelligence in Healthcare and Education
Introduction and background
Over the past two decades, the introduction and refinement of BCR-ABL1-targeting tyrosine kinase inhibitors (TKIs) have transformed chronic myeloid leukemia (CML) from a fatal disease into a chronic condition with near-normal life expectancy for most patients [1,2]. As CML management has evolved, the volume and complexity of longitudinal clinical and molecular data have increased, challenging traditional risk-stratification approaches.
In parallel, digitalization of healthcare and advances in artificial intelligence (AI) and machine learning (ML) have opened new horizons in data-driven medicine. CML, with its well-defined molecular driver, standardized response criteria, and structured follow-up, represents an ideal model for exploring the integration of AI into routine hematology practice. Treatment response is monitored using BCR-ABL1 levels on the International Scale, with key milestones including major molecular response (MMR), deep molecular response (DMR), and treatment-free remission (TFR) after planned TKI discontinuation in selected patients.
In this review, we provide an overview of current and emerging applications of digital medicine and AI in CML, summarize key evidence and limitations, and outline future directions for safe and meaningful clinical integration [3].
Review
Search strategy and selection criteria
This narrative review is based on a focused literature search combined with expert selection of pivotal studies in the fields of CML, digital health, and artificial intelligence. We searched PubMed/MEDLINE and Web of Science for English-language articles published between January 2010 and January 2026. The final search was completed on 10 January 2026 using combinations of the following terms: “chronic myeloid leukemia” OR “CML” AND “artificial intelligence” OR “machine learning” OR “deep learning” OR “digital health” OR “electronic health records” OR “clinical decision support” OR “ghost cytometry” OR “drug discovery”. Representative search strings included: (“chronic myeloid leukemia” OR CML) AND (“artificial intelligence” OR “machine learning” OR “deep learning” OR “digital health” OR “clinical decision support” OR telemedicine OR “ghost cytometry”). Additional relevant articles were identified by screening reference lists of key reviews and original research papers. This narrative review did not follow a PRISMA protocol, and formal duplicate screening or risk-of-bias assessment was not performed.
We prioritized peer-reviewed original studies and reviews that (i) involved adult CML patients, (ii) when CML-specific data were limited, we included studies from other hematologic malignancies only if they addressed a methodological gap clearly relevant to CML (e.g., flow cytometry analysis frameworks, histopathology algorithms), and we explicitly note this extrapolation in the text described concrete applications of digitalization, AI, or ML to diagnosis, prognosis, treatment selection, drug development, or patient monitoring, or (iii) addressed cross-cutting issues such as ethics, regulation, patient perceptions, and ML operations (MLDevOps) in medical AI. When CML-specific data were limited, we selectively included high-impact examples from broader hematology or oncology to illustrate general principles with clear relevance to CML.
This review does not aim to be a systematic review and does not provide a quantitative meta-analysis. Instead, it seeks to synthesize representative and influential work to highlight current capabilities, identify gaps, and propose priority areas for future research and clinical implementation of AI and digital medicine in CML.
Digitalization and data medicine in CML
Modern healthcare systems are increasingly driven by large-scale digital data. For CML, effective management depends on the ability to aggregate, harmonize, and analyze longitudinal information from multiple sources. Figure 1 illustrates a conceptual “Data → AI → Decision” framework for CML.
Digital Data Flow and the Role of Artificial Intelligence in CML Management.Data from multiple sources about CML patients, including electronic health records (EHR), laboratory results, molecular tests, imaging, and clinical parameters, are integrated on a unified digital platform. AI and ML algorithms process these heterogeneous data to generate clinical decision support for diagnosis, prognosis, and personalized treatment. Created by the authors with the assistance of generative AI tools (layout and icons refined via Midjourney / DALL·E), based on concepts from cited literature [4,5].AI: artificial intelligence; ML: machine learning; CML: chronic myeloid leukemia; EHR: electronic health records.Image credit: Created by the authors with the assistance of AI tools.
Electronic Health Records and Real-World Data
Large institutional and national EHR-based CML cohorts provide real-world evidence (RWE) that complements clinical trial results [4]. However, RWE capture must extend beyond routine laboratory and treatment data to include rare but life-threatening events. For example, spontaneous splenic rupture, though exceedingly rare, carries high mortality and is often diagnosed only postmortem [5]. Comprehensive digital registries that systematically capture such complications are essential for training AI models to recognize risk patterns and for generating alerts that could facilitate earlier intervention.
Telemedicine, Remote Monitoring, and Networked Registries
Telemedicine, including video consultations and secure messaging, has become increasingly important for chronic disease management. In CML, it facilitates frequent, low-burden follow-up, review of laboratory results, and timely intervention in case of warning signs. Wearable devices and home monitoring can capture physiological data (heart rate, activity, sleep) and patient-reported outcomes, providing additional signals of toxicity or decompensation. AI-enhanced Internet of Medical Things systems can aggregate such data and prioritize high-risk patients for clinician review [6,7]. Networked cancer registries and international CML collaborations pool genetic and clinical data from multiple regions, enabling the study of rare subgroups, comparison of practice patterns, and external validation of AI models across diverse settings. These efforts increase statistical power for analyzing TFR outcomes, uncommon resistance mechanisms, and late toxicities.
Real-World Evidence Integration and Federated Learning
The integration of RWE from heterogeneous healthcare settings is both an opportunity and a challenge. Differences in BCR-ABL1 assay calibration, monitoring intervals, and treatment protocols can introduce noise that degrades model performance. Nevertheless, RWE captures important aspects of routine care that clinical trials may miss [4].
In-depth real-world analyses have also explored TFR outcomes and longitudinal response patterns in CML cohorts managed in routine clinical settings [8]. Federated learning represents a promising strategy for multicenter AI development without centralizing patient-level data. Models are trained locally at each institution, and only parameter updates are shared and aggregated. This can mitigate privacy and governance concerns while improving model generalizability [9]. For CML, federated learning may be particularly useful for modeling rare scenarios such as T315I mutation or deep, sustained molecular responses enabling TFR. With this digital infrastructure in place, AI methods can be applied across the CML care continuum, including diagnosis, risk modeling, monitoring, and clinical decision support.
Artificial intelligence and machine learning in CML
The application of AI and ML in CML has evolved rapidly over the past decade. Early efforts (approximately 2017-2020) primarily focused on simple rule-based systems and classical ML classifiers (e.g., SVM, random forests) for automated cell counting and basic leukemia cell detection in peripheral blood smears [10,11]. Between 2020 and 2023, deep convolutional neural networks (CNNs), including architectures such as ResNet and U-Net, achieved near-expert performance in cytomorphological classification of bone marrow and peripheral blood images, significantly reducing inter-observer variability and enabling high-throughput analysis [10-14]. Since 2023, the field has progressed toward more advanced multimodal approaches that integrate clinical, genomic, histopathological, and imaging data [15], as well as innovative label-free technologies such as ghost cytometry, which allow non-invasive phenotypic detection of CML-like cells with promising correlation to molecular response markers. This progression reflects a shift from isolated image-analysis tools to integrated, data-driven decision support systems across the entire CML care continuum.
AI and ML methods are being applied across the CML care continuum, from diagnosis to long-term follow-up. The various AI methodologies and their specific applications within the CML clinical workflow, enabled by this digital infrastructure, are summarized in Table 1.
AI in Diagnostic Hematology
Figure 2 demonstrates how AI is integrated into diagnostic hematology through automated data processing.
Main Applications of Artificial Intelligence in Diagnostic Hematology.The central automated image and data processing module branches into three main domains: (1) cytomorphology—identification of cell types in peripheral blood and bone marrow smears, detection of dysplastic features, and quantitative assessment of cell populations; (2) cytogenetics—segmentation and classification of chromosomes and detection of structural and numerical abnormalities; (3) flow cytometry—analysis of immunophenotypic data, labeling of cell populations, disease classification, and MRD detection. Schematic created by the authors using AI-assisted design tools, conceptually grounded in references [10–12,17–19,25–31].AI: artificial intelligence; MRD: minimal residual disease.Image credit: Created by the authors with the assistance of AI tools.
Cytomorphology
Digital microscopy and deep learning (DL) have achieved near-expert performance in classifying blood and marrow cells. CNN-based models and commercial systems (e.g., Morphogo) can perform differential leukocyte counts, detect blasts, and identify dysplastic features with high accuracy [10-12]. Table 2 summarizes representative commercial AI tools in hematology, bridging research prototypes to clinical solutions; regulatory status and performance may vary by region, indication, and software version, and should be verified locally.
Adversarial DL has also been applied to bone marrow images for leukemia classification, including the identification of CML-compatible morphological features [13]. Unsupervised and semi-supervised ML techniques, such as K-means clustering and watershed segmentation, further refine cell detection and segmentation in blood smears [14]. More recent work has shown improved blood cell classification using U-Net segmentation and lightweight CNN architectures [15]. In addition, label-free and unstained blood smear analysis has expanded rapidly, offering potential pathways toward scalable diagnostics with minimal preprocessing [16]. These systems can serve as pre-screening tools, flagging suspicious smears for priority review and helping to standardize morphology assessment across laboratories.
Flow Cytometry
Multiparameter flow cytometry generates high-dimensional data that are well suited to ML analysis. Benchmark initiatives such as FlowCAP and related comparative studies demonstrated that automated methods can reliably support flow cytometry interpretation [17]. Deep learning models applied directly to expression matrices or gated populations have been used for MRD detection and classification tasks in hematologic malignancies, including multicenter EuroFlow studies in B-cell precursor ALL [18]. While flow cytometry is not used for MRD assessment in chronic-phase CML (where molecular monitoring is the standard), similar AI approaches could be transferable to CML for identifying aberrant myeloid populations at diagnosis or in advanced-phase disease [19].
Cytogenetics and Histopathology
AI has been used to automate chromosome segmentation and classification and to detect numerical aberrations on karyograms [20,21]. However, detection of the t(9;22) translocation characteristic of CML remains technically challenging. Current AI tools may assist with karyogram preprocessing but cannot yet replace expert review for structural variant identification. Broader CML-focused reviews also highlight expanding ML applications in prediction, diagnosis, and longitudinal management [22]. While complex structural variants remain challenging, AI can substantially reduce manual workload and increase analytic consistency.
In histopathology, DL algorithms applied to bone marrow biopsies can correlate morphological patterns (e.g., fibrosis grade, cellularity, megakaryocyte morphology) with genetic lesions and clinical outcomes. Machine learning on bone marrow histology has demonstrated the ability to identify genetic and clinical determinants in MDS populations, providing a transferable methodological paradigm [23]. Recent reviews also describe emerging AI applications and practical implementation challenges for bone marrow histological diagnostics [24]. These tools may eventually help identify CML patients at higher risk of progression based on subtle histologic changes. Table 3 summarizes key studies on AI applications in CML diagnosis, highlighting advances in cytomorphology, flow cytometry, and emerging label-free technologies such as ghost cytometry. Beyond diagnostic automation, similar AI approaches can also be applied to prognostic modeling and individualized treatment selection.
Prognostic Modeling and Individualized Treatment Selection
Traditional CML risk scores (Sokal, Hasford, EUTOS, ELTS) use a limited set of baseline variables. AI methods can incorporate a broader feature set, including longitudinal data and genomic profiles. Recent reviews summarize the current landscape of AI applications and highlight directions for individualized management in adult CML [22,32]. ML models have been developed to predict survival and progression risk using clinical and laboratory variables [33].
AI-based tools, such as the Leukemia Artificial Intelligence Program (LEAP), model predictors of molecular response to frontline imatinib and can guide TKI selection and timing of treatment changes [34]. Integration of gene mutation and expression data with clinical features enables more nuanced risk stratification and outcome prediction [35-37].
Polygenic and Multi-Factorial Risk
CML outcomes are influenced by more than BCR-ABL1 alone. Host genetics (e.g., polymorphisms in drug transporter genes such as OCT1 and ABCB1), immune microenvironment, and comorbidities all play a role [38,39]. Neural networks and other nonlinear ML methods are well suited to model these complex interactions. Supporting data also suggest that deep molecular responses to TKI therapy are accompanied by immune restoration and changes in immune checkpoints/suppressor populations, consistent with a measurable immunologic component of treatment response [40,41]. Broader reviews of ML applications in CML summarize these emerging multi-factorial predictors and their potential clinical uses [3,22,42].
Current ML applications include the following.
Prediction of DMR
Supervised ML models integrating baseline clinical, laboratory, and genetic features have achieved moderate-to-good discrimination (AUC ~0.72-0.82) for predicting DMR achievement on specific TKIs [43]. In addition, classical trial-based models and practice-level predictive frameworks continue to inform response stratification [44,45].
TFR Eligibility and Outcome Prediction
Landmark discontinuation studies established clinical eligibility criteria for TFR attempts based on population-level risks, but these criteria do not reliably predict individual outcomes [44,45]. Early exploratory work using transcriptomic or immune-based biomarkers has been reported, but validated ML models for individualized TFR prediction do not yet exist [46,47]. Emerging evidence also indicates that BCR-ABL1 transcript type, kinetic parameters (doubling/halving times), and immunological biomarkers may enhance prognostic accuracy when integrated into ML frameworks [48-50].
Exploratory biomarker analyses using gene-expression signatures have also been reported in major trial datasets, supporting the feasibility of transcriptomic predictors for DMR (conference abstract evidence) [51]. Dedicated AI/ML models for individualized TFR outcome prediction remain underdeveloped [52]. Development and external validation of such integrated models remain a high-priority area.
This reflects a shift from single biomarkers toward multi-factorial risk signatures that support more individualized treatment decisions.
Table 4 provides an overview of representative AI-based prognostic models in CML, including tools for molecular response prediction, TKI selection, and TFR probability.
In addition to baseline and genomic predictors, AI can also analyze longitudinal molecular data to support real-time response monitoring.
Molecular Response Monitoring and Ghost Cytometry
Automated BCR-ABL1 trend analysis: Standardized definitions of molecular response in CML (MMR, MR4, MR4.5) underpin current management algorithms [53]. However, interpreting serial BCR-ABL1 results remains challenging, particularly in borderline cases. AI-based trend analysis systems can: (i) Quantify log-linear decline in BCR-ABL1 levels; (ii) Estimate halving times and deviations from expected kinetics; (iii) Distinguish analytical variation from true loss of response.
Such tools can generate early alerts for suboptimal responders or impending relapse, supporting timely TKI dose adjustment or switching. The clinical relevance of early molecular kinetics for downstream outcomes, including TFR, has been demonstrated in large clinical datasets [52].
Ghost Cytometry
A recent proof-of-concept study demonstrated the feasibility of label-free detection of phenotypic CML-like cells in peripheral blood using AI-enabled ghost cytometry, with observed correlation between AI-detected cell burden and BCR-ABL1 transcript levels on the International Scale [28,54]. While promising as a potential complementary non-invasive approach, this technology requires substantial further clinical validation before any consideration for MRD assessment or early detection.
AI in Drug Discovery and Precision Medicine
AI contributes across the drug development pipeline. ML and deep generative models can screen large chemical libraries to identify candidate TKIs and allosteric modulators with favorable binding profiles [55-57]. Tools such as AllositePro, CavityPlus, Kinase Atlas, and FTMap help predict allosteric/orthosteric binding sites and ligandable pockets for rational inhibitor development [58].
AI systems such as AlphaFold facilitate modeling of protein structures, including mutant BCR-ABL1 variants, informing structure-based and allosteric drug discovery workflows [59]. More targeted mechanistic modeling of asciminib-related allosteric pathways has also been reported [60]. In silico screening has additionally identified natural compounds (e.g., withaferin A and withanone) as potential modulators of BCR-ABL1 signaling [61].
Figure 3 shows the integration of artificial intelligence and precision medicine in CML.
Integration of Artificial Intelligence in Precision Medicine for CML.Patient-derived clinical data and biospecimens undergo multiomics profiling (genome, transcriptome, proteome). AI algorithms transform these data into three main categories of outputs: (1) diagnostic—identification of inherited and pathogenic genetic variants and driver mutations; (2) prognostic—individualized prediction of survival and treatment response, risk stratification; (3) generative—protein structure modeling, digital twin creation, and in silico therapeutic simulations. Diagram originated by the authors and visually generated/refined with generative AI assistance; content derived from [35–37,54–60].AI: artificial intelligence; CML: chronic myeloid leukemia.Image credit: Created by the authors with the assistance of AI tools.
Clinical Decision Support Systems and Multimodal ML
Clinical decision support systems (CDSSs) can bridge the gap between complex AI models and everyday practice by embedding model outputs into interpretable interfaces aligned with guidelines [62]. General evidence syntheses in digital medicine also summarize CDSS benefits, risks, and implementation strategies [63,64].
In CML, potential applications include: (i) Automated classification of response categories (optimal, warning, failure) based on ELN criteria; (ii) Alerts for delayed molecular monitoring or suspected non-adherence; (iii) Structured TFR eligibility assessments incorporating molecular, clinical, and adherence data [31,33].
Figure 4 presents a multimodal ML platform that integrates clinical variables, imaging, histopathology, and sequencing data into a unified predictive framework.
Integrative Multimodal Machine Learning Platform for the Management of CML.Multiple data sources are integrated into a unified ML pipeline: (1) Clinical data—demographics, complete blood counts, risk scores; (2) Radiology—CT/MRI images (e.g., spleen size, organ involvement); (3) Histopathology—bone marrow biopsy with H&E staining and immunohistochemistry; (4) High-throughput sequencing—NGS panels, RNA-seq, BCR-ABL1 transcript levels. After preprocessing and data fusion, a multilayer neural network learns cross-modal relationships. Clinical applications include disease classification, outcome prediction, biomarker discovery, and digital twin simulations to support personalized treatment planning. Created by the authors with AI tool support for schematic visualisation, based on multimodal AI principles reviewed in [22,31,41].ML: machine learning; CML: chronic myeloid leukemia; CT: computed tomography; MRI: magnetic resonance imaging; H&E: hematoxylin and eosin; NGS: next-generation sequencing; RNA-seq: ribonucleic acid sequencing; BCR-ABL1: breakpoint cluster region–Abelson 1.Image credit: Created by the authors with the assistance of AI tools.
Challenges, ethics, and patient perspectives
Data Quality, Representativeness, and Bias
AI model performance is critically dependent on data quality and representativeness. In CML, key challenges include: (i) İnconsistent BCR-ABL1 assay calibration and reporting; (ii) Variable monitoring frequency and incomplete capture of molecular data in EHRs; (iii) Underrepresentation of patients from low- and middle-income countries and certain ethnic groups.
These issues have been highlighted by international standardization initiatives for molecular monitoring [64]. Models trained on homogeneous, single-center cohorts risk poor generalization and may embed existing healthcare disparities [31]. Addressing these issues requires harmonization of data standards, deliberate inclusion of diverse populations, and routine assessment of performance across subgroups (age, sex, ethnicity, and socioeconomic status).
Transparency, Explainability, and Regulation
The opaque nature of many AI models challenges clinician trust and regulatory oversight. Explainable AI methods such as SHAP and LIME can highlight which features most strongly influence predictions, helping clinicians interpret and, when necessary, challenge AI outputs [65-67].
Regulatory agencies are developing frameworks for AI-based software as a medical device (SaMD) and clinical decision support tools, but guidance is still evolving and may lag behind technological advances [68,69]. The widely implemented Epic Sepsis Model illustrates the risks of insufficient validation: despite broad deployment, external evaluation revealed poor discrimination and calibration, resulting in missed sepsis cases and excessive false alarms [70]. Editorial commentary further emphasized the importance of independent external validation before clinical scaling [71].
Even FDA-cleared AI/ML medical devices have exhibited reporting and performance issues, underscoring the need for clear evaluation metrics and robust post-market surveillance [72]. Emerging work on data drift further demonstrates that model performance can degrade over time as diagnostic criteria, treatment protocols, and patient populations change, necessitating continuous monitoring [73].
These experiences highlight the necessity of: (i) Multicenter external validation; (ii) Transparency regarding model performance and limitations; (iii) Prospective evaluation of clinical impact; (iv) Ongoing performance monitoring in real-world use.
Patient Perspectives and Acceptance
Patients’ attitudes toward AI in oncology are nuanced. Systematic reviews and qualitative studies show cautious optimism about improved diagnostic accuracy and access, but concerns about misdiagnosis, data privacy, and loss of human interaction [74].
Lower educational level is associated with greater discomfort about AI-led diagnosis [75]. The majority of patients prefer AI as an adjunct to, rather than a replacement for, clinicians: in one study, 94% favored human-AI collaboration, and many expressed a preference for additional confirmatory testing when AI and clinician opinions diverged [76].
In CML, where patients often maintain long-term relationships with their hematologists, AI tools should be explicitly framed as augmenting the clinician-patient partnership. Clear communication about AI’s role, limitations, and data governance is essential to maintain trust and engagement.
Lessons From Failed Implementations
As illustrated by the Epic Sepsis Model example discussed above, several general lessons emerge: (i) İnternal validation is insufficient; external and prospective validation are mandatory; (ii) Models must be monitored for performance drift as practice patterns and populations change; (iii) Regulatory and institutional oversight should scrutinize commercial algorithms before broad deployment [70,71].
Applying these lessons to CML, any AI tool intended for high-stakes decisions such as TKI selection or TFR prediction must undergo rigorous external and prospective validation before clinical integration, incorporate continuous performance monitoring to detect drift from evolving treatment protocols or patient cohorts, and receive thorough regulatory and institutional scrutiny to ensure safety and reliability in this high-stakes hematologic malignancy [3,73,77]. Simpler tools, such as automated calculation of BCR-ABL1 kinetics, may require less stringent validation but should still demonstrate accuracy and clinical utility.
Implementation pathway and future directions
Effective integration of AI into CML care requires a lifecycle perspective. Figure 5 outlines key stages from model development to clinical use, highlighting major challenges at each step.
Stages and Main Challenges in Integrating an AI Model from Research into Clinical Practice.The lifecycle of an AI-based diagnostic or prognostic tool comprises six stages: (1) data collection—aggregation and standardization of EHR, laboratory, imaging, and molecular data; (2) model training—development of ML/DL models on large datasets; (3) validation—external and multicenter testing across diverse populations; (4) regulation—approval by agencies (e.g., FDA/EMA) and adherence to clinical decision support standards; (5) clinical integration—embedding into EHR systems, adaptation to clinical workflows, and establishment of MLDevOps processes; (6) continuous monitoring—tracking model performance, detecting data drift, and updating models. Key challenges include data quality and accessibility, algorithmic bias, lack of transparency (“black box” issue), regulatory gaps, integration barriers, and limitations in monitoring infrastructure. Lifecycle diagram developed by the authors using generative AI for illustration; informed by MLDevOps literature [78,79].AI: artificial intelligence; EHR: electronic health records; ML: machine learning; MLDevOps: machine learning development and operations.Image credit: Created by the authors with the assistance of AI tools.
MLDevOps: Sustaining AI Performance Over Time
Machine Learning Development and Operations (MLDevOps) combines ML development with operational best practices to sustain AI performance in dynamic clinical environments [78,79]. The failure of the Epic Sepsis Model demonstrates generalizable lessons for clinical AI deployment: internal validation alone is insufficient and must be supplemented by rigorous external and prospective validation; models require continuous performance monitoring to detect drift amid evolving clinical practices, patient populations, and diagnostic/treatment protocols; and commercial and proprietary algorithms demand thorough regulatory and institutional scrutiny before widespread implementation [70,71,73,79]. These principles apply directly to CML: AI tools for interpreting BCR-ABL1 trends, selecting TKIs, and predicting TFR should be built and maintained using MLDevOps practices [3,80].
In CML, MLDevOps should include: (i) Continuous auditing of discrimination, calibration, and error patterns (including subgroup analyses); (ii) Automated detection of data drift (e.g., from new TKIs, ddPCR adoption, or changes in monitoring); (iii) Pipelines for automated retraining, version control, and rollback; (iv) Multidisciplinary oversight, transparent documentation, and comprehensive audit trails.
Priority Areas for Future Work
Multicenter RWE platforms: Harmonized CML registries and EHR-based datasets are needed to support robust, generalizable AI model development. Standardization of BCR-ABL1 assay reporting on the International Scale, consistent capture of adverse events, treatment changes, and adherence data are essential prerequisites.
Development of validated AI models for TFR prediction: Despite successful TFR in a substantial proportion of eligible CML patients, robust AI-based prediction tools remain limited. Classical TFR models from discontinuation trials rely largely on Cox regression and incorporate a restricted variable set (e.g., TKI duration, depth/stability of molecular response, baseline risk scores), underscoring the need for richer, individualized prediction approaches [56]. Patient-centered endpoints, including quality of life and treatment burden, should also be incorporated into future TFR frameworks [81].
Future ML models should integrate: (i) Longitudinal BCR-ABL1 kinetics (doubling-times, halving-times, trajectory modeling); (ii) Genomic and molecular features (BCR-ABL1 transcript type, additional mutations, gene expression signatures) [82,83]; (iii) İmmunological biomarkers (e.g., NK cell counts, T-cell repertoire diversity); (iv) Patient-reported outcomes (adherence patterns, quality of life, treatment burden) [81].
Such models have the potential to support shared decision-making for TFR attempts and reduce the psychological burden of uncertain outcomes.
Prospective validation of AI tools in clinical practice: Well-designed prospective studies should evaluate whether AI-supported care improves diagnostic accuracy, timeliness of interventions, TFR success rates, and patient-reported outcomes. Randomized trials comparing AI-guided versus guideline-concordant standard care are needed to demonstrate clinical utility beyond retrospective performance metrics.
Workflow integration and usability engineering: AI outputs should be embedded thoughtfully into EHR interfaces and clinical care pathways, minimizing alert fatigue and preserving clinician autonomy. User-centered design involving hematologists, nurses, and patients from the outset is critical to ensure adoption and sustained use.
Ethical and equitable implementation: Policies and technical safeguards should protect patient privacy, reduce algorithmic bias, and avoid exacerbating disparities in access to advanced CML care. Deliberate inclusion of underrepresented populations in training and validation cohorts, transparency regarding model limitations, and governance frameworks prioritizing autonomy and informed consent are essential.
Economic evaluation and health technology assessment: Cost-effectiveness analyses comparing AI-enhanced versus conventional CML management strategies remain limited. Health economic modeling should assess not only direct costs (diagnostics, TKIs) but also indirect costs (productivity loss, caregiver burden) and patient-centered outcomes (quality-adjusted life years, treatment-free survival).
Economic Considerations in AI Implementation for CML
Lifelong TKI therapy and monitoring impose a substantial financial burden: hundreds of thousands of dollars per patient annually [2,84].
Recent 2024-2025 data indicate: (i) Imatinib remains the most cost-effective first-line agent [85]; (ii) When incorporating TFR and dose reduction, imatinib dominates in cost-effectiveness [86]; (iii) Asciminib requires significant price reduction to achieve an acceptable incremental cost-effectiveness ratio [87]; (iv) TFR substantially reduces costs by enabling therapy discontinuation [88,89].
AI enhances cost-effectiveness by (i) Personalized TKI selection and early switching → reduced treatment failures and line-of-therapy costs; (ii) Risk-adapted monitoring → decreased frequency of qPCR testing; (iii) Early detection of relapse and toxicity → prevention of complications and hospitalizations; (iv) Optimized TFR prediction → increased success rates and savings on lifelong therapy.
In hematology, AI has already demonstrated high return on investment through reduction of unnecessary procedures [90].
Limitations of this review
This work is narrative, rather than a systematic, review and is therefore subject to several important limitations. First, although we conducted a focused literature search in PubMed/MEDLINE and Web of Science and complemented it with expert selection of key publications, we did not follow a predefined protocol (e.g., PRISMA), did not perform duplicate independent screening, and did not carry out a formal quality or risk-of-bias assessment of individual studies. As a result, selection bias and publication bias cannot be excluded, and the included evidence may overrepresent positive or high-profile results. Second, the heterogeneity of study designs, populations, endpoints, and performance metrics across AI and digital health applications in CML precluded quantitative synthesis or meta-analysis and limits the comparability of reported outcomes. Third, some AI approaches with clear conceptual relevance to CML are currently supported only by small, single-center, or preclinical studies, and their generalizability to broader, real-world CML populations remains uncertain. Fourth, we focused on English-language publications from 2010 onward; potentially relevant work published in other languages or outside the indexed databases may have been missed. Finally, the rapidly evolving nature of AI and digital medicine means that newer tools and regulatory developments may have emerged after the completion of our literature search. These limitations should be considered when interpreting the scope and implications of the findings discussed in this review.
Conclusions
Digital medicine and AI are creating new opportunities to improve the diagnosis, risk stratification, treatment selection, and long-term management of chronic myeloid leukemia. Emerging applications range from automated morphology and flow cytometry analysis to molecular trend interpretation, adherence monitoring, and AI-assisted drug discovery, all of which may support more precise and individualized care. However, many of these tools remain in exploratory or early clinical stages, and robust prospective validation is still required. A notable gap is the absence of clinically validated AI or machine-learning models for individualized treatment-free remission prediction, despite its major clinical, psychological, and economic implications. Developing explainable models that integrate BCR-ABL1 kinetics, transcript type, and host factors represents an important research priority.
Experience from other medical domains also shows that technical performance alone does not guarantee clinical benefit. Successful implementation of AI in CML will require rigorous multicenter validation, transparent and guideline-aligned models, appropriate regulatory oversight, and active involvement of clinicians and patients in system design and evaluation. With careful development and integration into clinical workflows, AI-driven approaches have the potential to support more personalized, evidence-based, and patient-centered care for individuals living with CML.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Long-term outcomes of imatinib treatment for chronic myeloid leukemia N Engl J Med Hochhaus A Larson RA Guilhot F 91792737620172827302810.1056/NEJ Moa 1609324 PMC 5901965 · doi ↗ · pubmed ↗
- 2Chronic myeloid leukemia: 2025 update on diagnosis, therapy, and monitoring Am J Hematol Jabbour E Kantarjian H 219122129920243909301410.1002/ajh.27443 · doi ↗ · pubmed ↗
- 3Application of artificial intelligence in chronic myeloid leukemia (CML) disease prediction and management: a scoping review BMC Cancer Ram M Afrash MR Moulaei K 10262420243916465310.1186/s 12885-024-12764-y PMC 11337640 · doi ↗ · pubmed ↗
- 4The case for real-world evidence in the future of clinical research on chronic myeloid leukemia Clin Ther Webster J Smith BD 3363494120193070960910.1016/j.clinthera.2018.12.013 · doi ↗ · pubmed ↗
- 5An autopsy presentation of spontaneous splenic rupture in chronic myeloid leukemia: a rare case report J Med Surg Public Health Kanani J Sheikh MI 2024
- 6Effectiveness of digital care platform C My Life for patients with chronic myeloid leukemia: results of a patient-preference trial BMC Health Serv Res Verweij L Ector GI Smit Y van Vlijmen B van der Reijden BA Hermens RP Blijlevens NM 2282320233689051210.1186/s 12913-023-09153-9PMC 9994406 · doi ↗ · pubmed ↗
- 7Enhancing remote patient monitoring with AI-driven Io MT and cloud computing technologies Sci Rep Damera VK Cheripelli R Putta N Sirisha G Kalavala D 240881520254061785210.1038/s 41598-025-09727-z PMC 12228823 · doi ↗ · pubmed ↗
- 8In-depth analysis for TKI-driven real-world management of 201 CML patients using TFR Front Pharmacol Micu ML Cira SF Zdrenghea M 16730561620254128261610.3389/fphar.2025.1673056 PMC 12631139 · doi ↗ · pubmed ↗