Giant parieto-occipital encephaloceles: always a dismal prognosis? A case report and review of the literature
Wouter J. Dronkers, Irene M. J. Mathijssen, Attie Go, Victor Volovici, Jochem K. H. Spoor

TL;DR
An infant with a severe brain malformation showed unexpected stability and development, challenging assumptions about poor outcomes.
Contribution
This case report challenges the assumption that giant encephaloceles always lead to poor outcomes by presenting a positive long-term follow-up.
Findings
The patient remained stable after birth and showed developmental progress at 4 years old.
Surgical reconstruction was successfully performed at 4 weeks of age.
The case suggests that long-term expectations for such conditions may need reconsideration.
Abstract
The presented case involves an infant with a prenatally diagnosed giant encephalocele including parts of the occipital and superior parietal lobes, as well as the superior cerebellum. Imaging revealed a complex encephalocele with absence or hypoplastic aspects of venous structures, including the vein of Galen and transverse and sigmoid sinus. Clinically, despite the anticipated poor prognosis, the patient remained stable after delivery, leading to a reassessment of the initial palliative care plan. Surgical reconstruction of the encephalocele was performed at 4 weeks of age. The most recent follow-up was conducted at 4 years of age. The patient demonstrated significant developmental progress including speech, language, and motor skills without complaints of headache or nausea. The presented case highlights the medical and ethical challenges physicians face while dealing with pediatric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
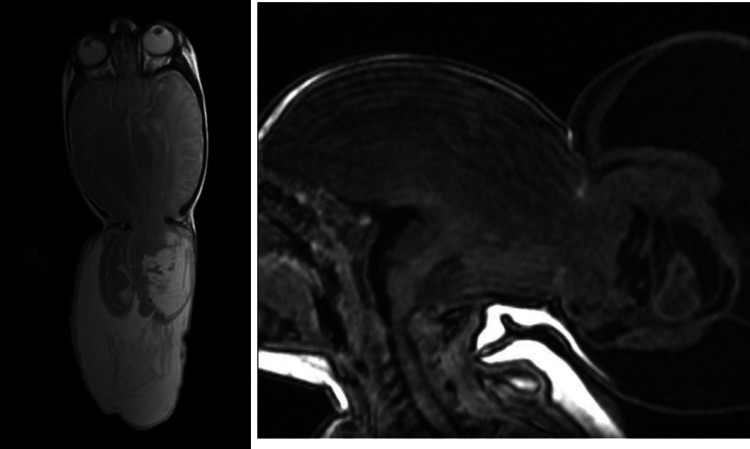 Figure 1
Figure 1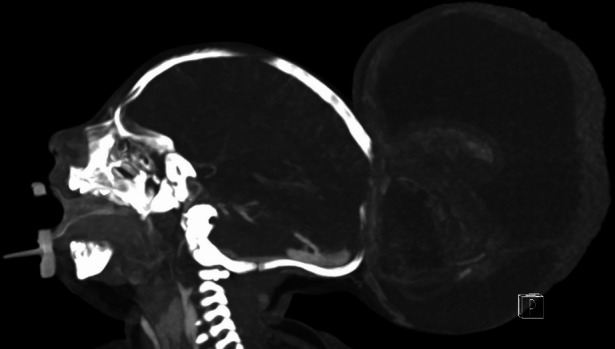 Figure 2
Figure 2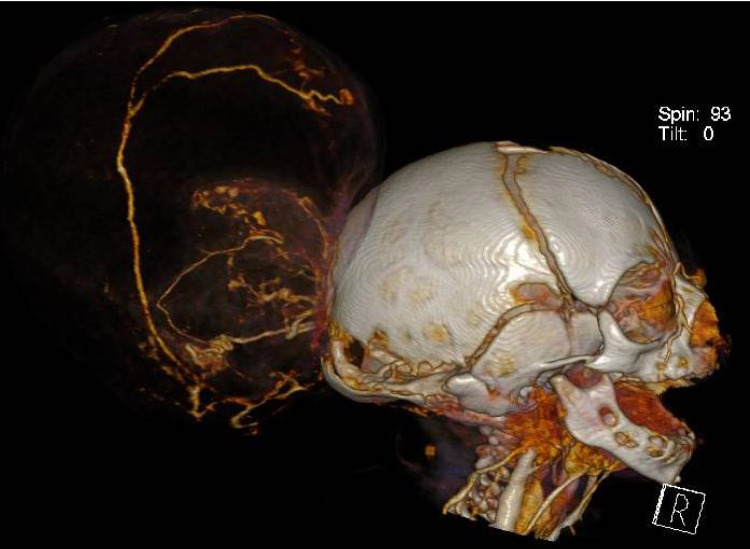 Figure 3
Figure 3 Figure 4
Figure 4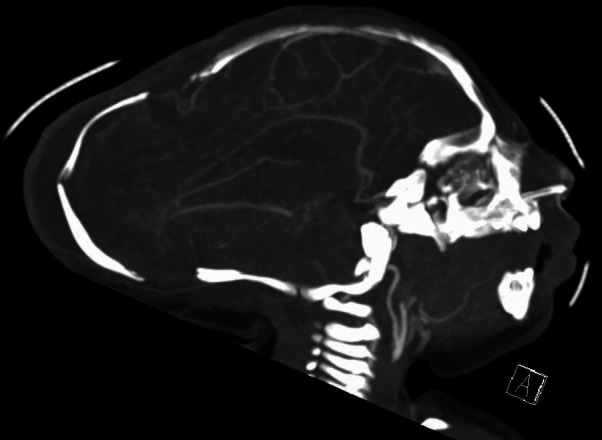 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Surgical Oncology · Cerebrospinal fluid and hydrocephalus · Teratomas and Epidermoid Cysts
Case report
An encephalocele refers to a severe congenital neurological condition which is characterized by herniation of neural tissue through a defect of the neurocranium. Encephalocele, which is considered a neural tube defect, has an estimated prevalence of 1–5 per 10,000 livebirths [1]. Classification of encephalocele is based on the anatomical location of the skull defect. Most often, the encephalocele is located occipitally [2]. In cases in which the encephalocele is larger than the patient’s head, it is referred to as “giant encephalocele” [3].
Prognosis in patients with a giant encephalocele is largely related to the location, size of the cele, amount of brain tissue affected, and presence of other intra- and extracranial anomalies (Table 1) [2, 4]. Although mortality rates are relatively low in patients with giant occipital encephalocele, various developmental issues exist (Table 2). Delayed milestones are frequently reported ranging from mild cognitive impairment to severe retardation. Motor function including being able to sit or walk without assistance is important yet infrequently reported outcomes. Therefore, adequate counseling of parents and treatment of these patients remain challenging from a medical and ethical point of view. Table 1. Demographic and radiological characteristicsAuthorPatients (female)Sac, dimensionsSac, contentsDatta et al. [5]4 (1)10 × 14 cm–18 × 20 cmCystic with small amount of neural tissue (n = 3); significant amount of neural tissue (n = 1)Atallah et al. [6]1 (1)40 cm circumferenceCystic with small amount of neural tissueQudsieh et al. [3]7 (5)12 × 10 × 9 cm – 15 × 12 × 10 cmNot individually specifiedDeora et al. [7]1 (1)98 cm circumferenceCystic with small amount of neural tissueSingh et al. [8]11 (5)Not specifiedNot individually specifiedMurthy et al. [9]1 (1)20 × 15 × 28 cmCystic with small amount of neural tissueNaik et al. [10]1 (1)26 × 34 × 30 cmCystic with small amount of neural tissueKanesen et al. [11]1 (1)44 cm circumferenceCystic with small amount of neural tissueOzdemir et al. [12]4 (4)14 × 18 cm–20 × 24 cmSignificant amount of neural tissue (n = 3); cystic without neural tissue (n = 1)Canaz et al. [13]1 (0)9 × 8 cm and 10 × 9 cmSignificant amount of neural tissueMahapatra et al. [14]13 (NS)**NSNot individually specifiedSather et al. [15]1 (1)19 × 9 cmCystic with small amount of neural tissueAndarabi et al. [16]1 (0)38–60 cm circumferenceCystic with small amount of neural tissueMohanty et al. [17]2 (NS)25 × 12 cm–30 × 25 cmSignificant amount of neural tissue (n = 2)Mardzuki et al. [18]3 (2)22 × 8 cm–28 × 15 cmCystic with small amount of neural tissue (n = 2); not specified (n = 1)Neupane et al. [19]1 (0)20 × 15 × 17 cmCystic with small amount of neural tissueNS not specified, cm centimeterThe reported patient had two encephaloceles**Only patients with occipital encephaloceles were collectedTable 2Shunt dependency, outcomes, and mortalityAuthorFU timeShuntOutcomeMortalityDatta et al. [5]1–13 years2Age-appropriate milestones (n = 2)Delayed milestones (n = 2)1Atallah et al. [6]40 months1Delayed milestones (n = 1)0Qudsieh et al. [3]2 years0Delayed milestones in speech and walking (number of patients not specified)1Deora et al. [7]1 year1Age-appropriate milestones; able to walk and crawl; able to track objects0Singh et al. [8]6 months – 4 years4Delayed milestones (n = 2); doing well (n = 2); lost to follow-up (n = 2); not specified (n = 2)3Murthy et al. [9]2 years1Delayed milestones0Naik et al. [10]1 year1Age-appropriate milestones; able to hold head; sit without assistance0Ozdemir et al. [12]18–40 months0Normal motor & mental development (n = 2); motor & mental retardation (n = 2)0Canaz et al. [13]3 years0Delayed milestones; walking without assistance; equal use of all extremities0Mahapatra et al. [14]6 months – 4 years5Age-appropriate milestones (n = 9); delayed milestones (n = 2)2Sather et al. [15]2 years1Delayed milestones; walking without assistance; equal use of all extremities; few word vocabulary0Andarabi et al. [16]2 years0Age-appropriate milestones0Mohanty et al. [17]2 years1Delayed milestones (n = 1); not specified (n = 1)0Mardzuki et al. [18]3 years1Doing well (n = 2); cerebral palsy (n = 1)0Neupane et al. [19]NS1Good state of health0NS, not specified
The presented case involved an infant with a prenatally diagnosed severe encephalocele involving herniation of the occipital and superior parietal lobes and superior cerebellum, delivered within our tertiary referral center.
In the presented case, the parents had been counseled by colleagues from the neonatology department before and after delivery regarding the assumed poor prognosis, and the pediatric palliative care team was engaged. The patient was discharged at one week of age with a plan for best supportive, palliative care. In the subsequent days, the patient’s clinical condition remained stable. A reassessment of the initial management plan was undertaken within the multidisciplinary boards, and the patient was readmitted at three weeks of age for further diagnostic evaluation and treatment.
Imaging studies (Fig. 1) demonstrated a severe meningoencephalocele with herniation of both the occipital lobes as well as part of the parietal lobes and the superior cerebellar hemispheres and vermis. Additional CT-angiography (Figs. 2 and 3) identified the confluence of sinuses at the level of the skull defect, with the sinus rectus located within the encephalocele. Notably, imaging also revealed the absence of the vein of Galen and a hypoplastic left transverse and sigmoid sinuses.Fig. 1. Preoperative postnatal MRI provides an axial and sagittal view of the preoperative MRI showing herniating neural tissueFig. 2Preoperative CT-angiography reveals the absence of a vein of Galen complex and a hypoplastic transverse and sigmoid sinus on the left sideFig. 3Preoperative CT-angiography
Reconstruction of the encephalocele and skull defect was performed at four weeks of age, together with the Plastic- and Reconstructive Surgery service. The meningocele was opened and the edges of the dura mater under the bone were exposed. Care was taken to not injure the exposed venous outflow. Necrotic tissue was removed from the occipital lobes. These were noted to be smooth, without gyral imprint and without M4 and P4 vessels running on their surface with the use of ultrasound. After excision, the remaining vital brain tissue was covered with a dural substitute. Strips of bone were cut from the skull surrounding the defect and fixated in a fashion covering the maximal surface of the defect with minimal cranial expansion. The extra skin was removed and the cele was closed (Figs. 4 and 5). The procedure was performed with less than 250-mL blood loss. The postoperative phase was uneventful.Fig. 4. Pre and postoperative clinical photography represents the preoperative (left picture) and postoperative (right picture)Fig. 5. Postoperative CT-angiography, sagittal view
The most recent follow-up was conducted at 4 years of age. At this time, significant progress in language, speech, and motor skill development (e.g., being able to walk without assistance and grasp and hold items using both hands) was observed. The patient is able to form up to seven-word sentences and count up to 30. Notably, the patient exhibited no complaints of headache, nausea, or vomiting and imaging studies show development of the parts of the brain not involved in the encephalocele. However, assessment of visual function reveals impairments in vision and color perception.
The case presented demonstrates a complex giant meningoencephalocele, with aberrant venous anatomy, with absence of the vein of Galen and hypoplastic transverse/sigmoid sinuses, but with a relatively less severe clinical presentation than imaging studies and scientific literature suggest. The subsequent evolution might challenge the paradigm to generalize poor outcome to all patients with complex giant encephaloceles.