Orthopedic manifestations as presenting symptoms in children with neuroblastoma: a retrospective case series and clinical review
Siddarth Kamath, Kumar Amerendra Singh, Hitesh H. Shah

TL;DR
About 20% of children with neuroblastoma first show orthopedic symptoms like hip or back pain, which can delay diagnosis if not properly evaluated.
Contribution
This study highlights the importance of considering neuroblastoma in children with atypical musculoskeletal symptoms and abnormal blood markers.
Findings
Seven out of 46 children (20%) initially presented with orthopedic symptoms.
Three children had spinal involvement, and three had hip pain initially misdiagnosed as osteomyelitis.
Six children had severe anemia and elevated inflammatory markers like ESR and CRP.
Abstract
Neuroblastoma is the second most common childhood malignancy. Only a minority of children with metastatic disease present initially to orthopedic surgeons, despite musculoskeletal complaints such as back pain, limb pain, limp, extremity swelling, or findings mimicking osteomyelitis. These vague and nonspecific presentations increase the risk of delayed diagnosis. To study orthopedic manifestations that present as the initial presenting symptoms of neuroblastoma in children and to characterize their clinical, radiological, and laboratory profiles. Forty-six consecutive patients with neuroblastoma were retrospectively evaluated. Medical records were reviewed, with particular attention given to the presence of orthopedic manifestations preceding the diagnosis of neuroblastoma. The children who were presented primarily to the orthopedics department were identified. The details of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
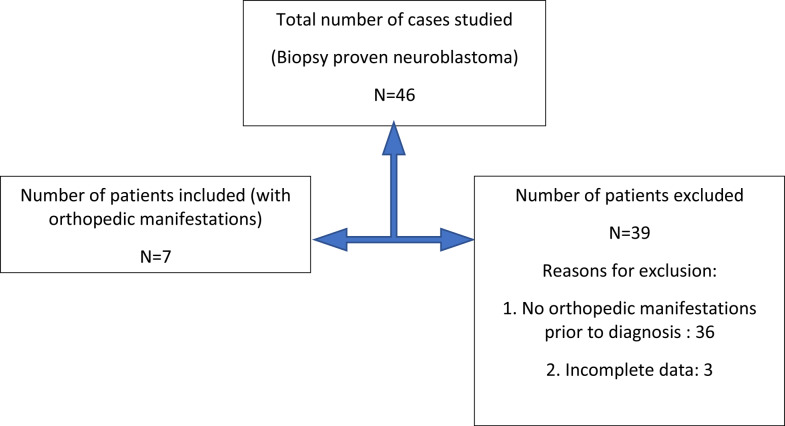 Figure 1
Figure 1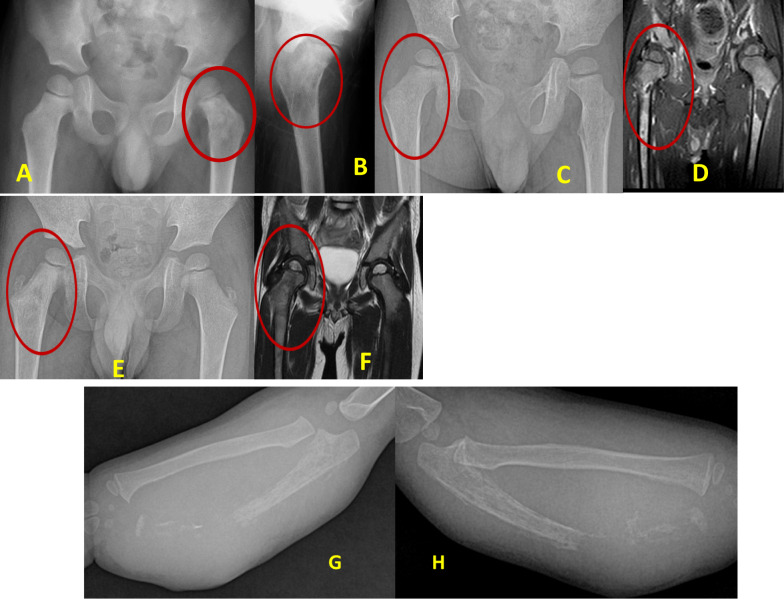 Figure 2
Figure 2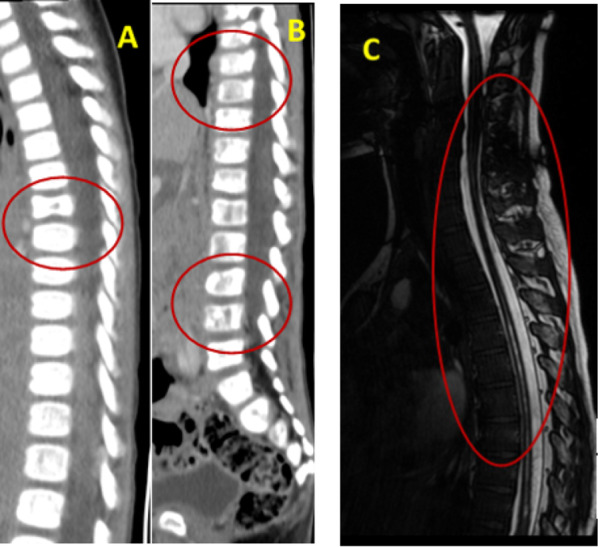 Figure 3
Figure 3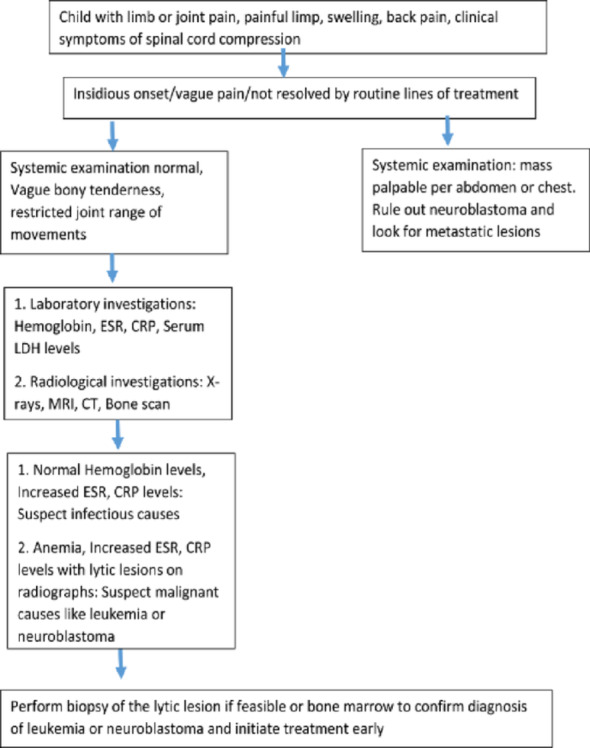 Figure 4
Figure 4- —Manipal Academy of Higher Education, Manipal
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroblastoma Research and Treatments · Management of metastatic bone disease · Orthopedic Infections and Treatments
Introduction
Neuroblastoma is the most common extracranial solid tumor in childhood [1, 2]. It typically arises from primordial neural crest cells of the sympathetic nervous system [1, 15]. Most commonly, the primary tumor is located in the adrenal glands, the sympathetic chain or the lung [1, 15]. Up to 60–70% of children suffering from neuroblastoma present with metastatic disease with high affinity toward the bone and bone marrow [2, 4]. Consequently, orthopedic symptoms ranging from bone pain, limp, and pathological fractures to spinal cord compression are common [3].
The correct diagnosis of neuroblastoma may be delayed because of the evaluation of common local and generalized systemic differentials of a limping child [1]. Local bone diseases such as osteomyelitis; bone tumors such as Ewing sarcoma or osteosarcoma; occult tuberculosis; septic arthritis; Perthes disease; and systemic diseases such as rheumatic disease, leukemia and sickle cell disease pose significant diagnostic dilemmas [1, 11].
25% of children suffering from neuroblastoma present primarily to orthopedic surgeons with symptoms that mimic these common differential diagnoses [3]. Some studies have shown a delay of 15 days to 5 months in establishing a diagnosis of neuroblastoma due to vague presentations [6, 7].
For treatment to be effective, it is paramount to diagnose these rare tumors as early as possible [4]. In the literature reviewed, these orthopedic manifestations are not well described.
The objectives of this study were as follows:
- To evaluate the orthopedic manifestations that serve as initial presenting symptoms in children later diagnosed with neuroblastoma.
- To evaluate the clinical, radiological, and laboratory characteristics associated with thesepresentations.
- Evaluating diagnostic pathways and delays to identify opportunities for earlier recognition.
Materials and methods
Study design
A retrospective case series compliant with the STROBE guidelines was conducted in the Department of Pediatric Orthopedics at a tertiary care hospital between January 2006 and December 2024.
Data collection
The records of all consecutive children aged less than or equal to 18 years at diagnosis with biopsy-confirmed neuroblastoma were included in the study. Children with incomplete medical or imaging data or with other musculoskeletal oncological conditions were excluded from the study.
Data collection
Data were extracted from the hospital records using a structured proforma Fig. 1. The following variables were studied:
Clinical presentations Symptoms in the child, such as pain, limp, bone or joint swelling, back pain or spinal compression.
Radiological investigations X-rays, bone scan reports, and CT or MRI scans that revealed skeletal involvement.
The laboratory findings included the erythrocyte sedimentation rate (ESR), hemoglobin levels, platelet counts, serum lactate dehydrogenase (LDH) levels and blood peripheral smears.
LDH and blood peripheral smears were performed, as elevated LDH or abnormal smears suggest marrow infiltration or alternative hematologic malignancies with atypical clinical presentations.
Initial diagnosis/source of referral whether seen initially by the Pediatric Orthopedic Department or other departments.
Time to diagnosis the time interval between the presentation of symptoms and the establishment of a diagnosis of neuroblastoma by biopsy of the involved site or the bone marrow.
Fig. 1. Flowchart showing patient inclusion for the study
Data analysis
Descriptive statistics were used to summarize the demographic and clinical data. Categorical variables are reported as frequencies and percentages. Continuous variables are expressed as the means Table 1.
Comparisons were made between patients who presented with limb involvement and those who presented with spine involvement using the chi-square test. A p value of < 0.05 was considered to indicate statistical significance. Data analysis was performed using SPSS for Windows Table 2.
Results
Demographic data
A total of 46 consecutive children with biopsy-proven neuroblastoma were included in the study. Seven children fulfilled the inclusion criteria and presented primarily to the orthopedic surgeon.
Table 1. Summarizing demographic data Sex (N = 7)Male = 4Female, N = 3Mean age at presentation (Mean ± SD) (years)4.3 ± 2Mean duration of follow up (Mean ± SD) (months)20 ± 6
Prevalence of orthopedic manifestations
Table 2. Various orthopedic manifestationsOrthopedic manifestationNumber of casesPain in the bone or joint4 (3 children: Pain in the hip joint, 1 child with painful swelling of forearm)Limp or refusal to walk3Back pain or spinal symptoms3Pathological fracture1 (distal ulna)
Painful limp due to effects on the hip joint was the most common presenting symptom.
Radiological features (Figs. 1 and 2)
Fig. 2A–F. Osteolytic lesions marked with red circles. Figure A and B—Showing child 1, who presented with left hip pain and painful limp. X-rays revealed lytic lesions over the proximal femur. The child had anemia and elevated ESR and CRP levels. Child underwent biopsy of the lesion, revealing the diagnosis of neuroblastoma. Figures C and D show child 2, and E and F show child 3, who presented with right hip pain and painful limps. X-rays revealed a subtle lytic lesion over the proximal femur. MRI was performed and revealed osteomyelitis. The child had severe anemia with elevated ESR, CRP and LDH levels. A biopsy and histopathological examination revealed a diagnosis of neuroblastoma. G and H – Child 4, who presented with painful swelling over the forearm. X-rays revealed a lytic lesion over the distal ulna with pathological fracture. A differential diagnosis of osteomyelitis was suspected. The child had anemia and elevated ESR and CRP levels. A biopsy was performed, which revealed a diagnosis of neuroblastoma
Fig. 3(A–C). Osteolytic lesions marked with red circles. Figure A shows child 5, Figure B shows child 6, who presented with symptoms of spinal cord compression and paraplegia. CT scans revealed extensive metastatic lesions over the vertebral body. These lesions were lytic lesions with a surrounding zone of sclerosis. Bone marrow biopsy revealed a diagnosis of neuroblastoma.Figure C–Child 7 presented with infantile neuroblastoma with extensive vertebral metastasis and hydromelia. MRI revealed lesions and cord involvement. Bone marrow biopsy revealed a diagnosis of neuroblastoma
Skeletal involvement on imaging was observed in all 7 children Fig. 3 and 4.
Lytic bone lesions (X-rays) Three children had lytic lesions of the proximal femur that mimicked osteomyelitis. One child had a lytic lesion on the distal ulna with a pathological fracture resembling osteomyelitis.
Spinal lesions with cord compression (CT or MRI) Three children had lytic lesions of the vertebral bone with surrounding zones of sclerosis.
Fig. 4. Diagnostic flowchart
Laboratory investigations
Table 3. Showing laboratory parametersParameterNumber of casesElevated ESR levels6 (Mean ± SD = 94 ± 10)Elevated CRP levels6 (Mean ± SD = 85 ± 8)Anemia7 (Mean ± SD = 7.1 ± 1.3)Elevated platelet counts3Elevated LDH levels3
All the children who presented with orthopedic manifestations were anemic Table 3.
Table 4. Literature review of various studies on the musculoskeletal manifestations of neuroblastomaReferences N Study typeMusculoskeletal manifestationLaboratory investigationsRadiological investigationsRemarksLimitations of the studyBusfield et al. [1]6Retrospective case seriesPain in joint or limb pain, Limp, Bone pain resembling osteomyelitis, Backache, ParaplegiaIncreased ESR levelsOsteolytic bone lesions in the metaphysis, may be bilateral, could resemble onion skin appearance–Only ESR levels and Xray radiographs were studied. Other radiological or laboratory parameters were not evaluatedAshton et al. [12]20Retrospective case seriesHip pain, Nonspecific limping, Limb weakness, Back painLow Hemoglobin, Elevated ESR levelsPerform bone marrow aspiration to confirm diagnosisUltrasound examination and hip aspiration to rule out infectionSuggested bone marrow aspiration only once ultrasound or hp aspiration results were equivocal. This could add to the diagnostic delayWong et al. [7]1Case reportHip and Back painIncreased ESR and LDH levels, AnemiaPerform bone scan in suspicious cases–Small sample sizeMohan et al. [5]1Case reportIrritable hipLow HemoglobinConsider early MRI in vague presentations–Suggested MRI in suspicious lesions. However, MRI findings maybe inconclusive leading to delay in diagnosisThapa et al. [6]2Letter to editorMultiple joint pains mimicking juvenile rheumatoid arthritisLow hemoglobin, High ESR, LDH levelsBone scan to look for marrow infiltration–Small sample sizeNatrajan et al. [13]1Case reportIrritable hipSevere anemia and presence of blasts on peripheral smear––Small sample sizeChu et al. [9]2Retrospective case seriesMultiple joint pains mimicking juvenile rheumatoidarthritis---Abdominal examination and ultrasound evaluation in suspicious cases–Described only the imaging features of metastatic neuroblastomaParmer et al. [3]4Retrospective case seriesIrritable hipAnemia, High ESRTargeted screening of abdomen with ultrasound along with hip ultrasound in suspicious casesFollow with MRI if abdominal screening is negativeSome cases of neuroblastoma cold be extra abdominal. Stepwise diagnostic pathways could lead to delayed biopsy and confirmatory diagnosisAmin et al. [8]2Retrospective case seriesIrritable hipLaboratory investigations are not specificSuggested MRITo keep patients with non specific hip pain in close follow up for upto 3 monthsDeferring a biopsy could lead to diagnostic delaysDaSilva et al. [4]1Case reportIrritable hipAnemia, High ESR, LDHBone scan to diagnose marrow infiltration in suspicious cases–Small sample sizeAbousamra et al. [14]2Retrospective case seriesHip pain, painful limp--––Small sample sizeCurrent study7Retrospective case seriesIrritable hip, Forearm swelling, Spinal metastasis, ParaplegiaAnemia, Increased ESR, CRP, Platelet and LDH levelsCT, MRI are not specific for diagnosisEarly consideration of histopathological examination of suspicious lesions or bone marrowTreatment provided and long term follow-up is not discussedN, Number of cases
Initial clinical misdiagnosis
Among the 7 children with orthopedic symptoms, 4 were initially misdiagnosed with osteomyelitis. Three children had proximal femur involvement, and 1 child had involvement of the forearm Table 4.
Time to diagnosis
The time from the onset of orthopedic symptoms to diagnosis was as follows:
- Limb involvement group: 4.5 weeks (SD 3.5–6).
- Spine involvement group: 2 weeks (SD 1.0–3.0).
This difference was statistically significant (p = 0.01).
Referral patterns
Four children with limb involvement were first seen by the pediatric orthopedic department, 3 children with spine involvement were first seen by the pediatric department, and referrals were sought from the pediatric orthopedic department.
Discussion
This study presents one of the larger cohorts examining orthopedic manifestations as initial presentations of neuroblastoma, demonstrating that approximately one-fifth of children manifested musculoskeletal symptoms before diagnosis. Although this proportion is clinically significant, it likely reflects referral patterns to a tertiary orthopedic center and should be generalized cautiously. Nevertheless, these findings reinforce the importance of maintaining diagnostic vigilance when evaluating persistent or unexplained musculoskeletal complaints in children.
Bone or joint pain and limping were the most frequent presenting symptoms, which is consistent with prior studies reporting high rates of skeletal involvement in disseminated disease [3–6]. However, these symptoms remain nonspecific and overlap with several benign pediatric orthopedic conditions. Back pain and signs of spinal cord compression are more suggestive of serious pathology but typically represent advanced disease, limiting their utility for early detection. Previous studies often emphasize these features as diagnostic clues, but such signs usually appear only after significant tumor progression and may not improve timely diagnosis.
Misdiagnosis of osteomyelitis, which was encountered in four patients in this study, remains a well-documented challenge. Wong et al. and Busfield et al. [1, 7] reported similar diagnostic delays due to overlapping clinical and laboratory features between infection and malignancy. The average diagnostic delay of 4.5 weeks in our cohort was shorter than that in earlier reports; however, this difference may reflect increased institutional awareness rather than inherent improvements in distinguishing early disease. Children with spinal involvement are diagnosed more rapidly because of the urgency of neurological symptoms, again highlighting that dramatic presentations expedite diagnosis, whereas subtle symptoms often lead to delays.
Previous authors have recommended adjunct investigations—MRI, hip aspiration, bone marrow studies, scintigraphy, and abdominal ultrasound—when the clinical findings are atypical [3, 5, 7, 12]. However, much of this guidance stems from small series or case reports, and their diagnostic performance has not been systematically evaluated. Parmar et al. [3] suggested a screening ultrasound examination of the abdomen in children with atypical limp. However, neuroblastoma is known to involve extra-abdominal sites, which could be missed with an abdominal ultrasound and cause further delays in diagnosis. Our findings demonstrate that initial imaging, including MRI, frequently fails to confidently identify malignancy, highlighting the limitations of current modalities when used in isolation. The reliance on biopsy for definitive diagnosis is consistent with previous literature but also illustrates that delays may occur when biopsy is deferred in favor of stepwise testing for more common conditions.
The identification of an atypical metastatic site in the distal forearm further challenges the classical pattern described by Wong et al. and Chu et al. [7, 9], who emphasized axial and proximal appendicular involvement. Such atypical presentations complicate diagnostic reasoning and underscore the need for a low threshold to investigate lytic lesions that do not fit expected clinical patterns. In our cohort, most lesions were osteolytic with surrounding sclerosis, a finding that may mimic infection or healing of bone and contribute to misinterpretation. Although osteolysis has been widely described [2, 4], the variabilityof accompanying reactive changes is underrecognized in the literature and may hinder timely diagnosis.
The role of orthopedic surgeons as early identifiers of malignancy is widely acknowledged, yet prior literature may overstate the practicality of this expectation. Orthopedic clinics frequently encounter nonspecific pain and limp, and without structured evaluation pathways, early malignancy can be easily overlooked. Our findings support the need for standardized protocols for escalating evaluation—particularly when pain persists, imaging is inconclusive, or laboratory abnormalities coexist. Early multidisciplinary involvement may help mitigate diagnostic delays.
Overall, this study highlights both the importance and the limitations of orthopedic presentations as early indicators of neuroblastoma. While musculoskeletal symptoms should prompt consideration of malignancy in atypical cases, their low specificity, variable imaging features, and overlapping differential diagnoses continue to pose significant challenges. Future research should focus on identifying more reliable clinical or imaging markers and evaluating diagnostic algorithms that may facilitate earlier recognition of malignancies in pediatric orthopedic practice.
Strengths
This study is one of the largest single-center studies to focus on the orthopedic manifestations of neuroblastoma. The clinical, radiological and laboratory features were characterized in detail. It includes diagnostic timelines, delays and common misdiagnostic patterns of this condition.
Limitations
This was a single-center retrospective study. The sample size, although representative, may limit generalizability. The treatment details and long-term outcomes were not described in this study.
Conclusion
The results of our study show that a child with neuroblastoma often presents primarily to orthopedic surgeons (20%). Children with atypical hip pain, back pain with severe anemia and elevated ESR and CRP levels should alert the treating orthopedic surgeon to suspect the differential diagnosis as neuroblastoma and consider histopathological confirmation to reduce delays in treatment.