Major Adverse Limb Events and Death After Successful Endovascular Revascularization: BEST-CLI Trial
Scott Kinlay, Alik Farber, Matthew T. Menard, Michael B. Strong, Michael D. Dake, John Kaufman, Peter A. Schneider, Michael S. Conte, Palma M. Shaw, Vikram S. Kashyap, Kenneth Rosenfield, Gheorghe Doros, Jeffrey J. Siracuse, Richard J. Powell

TL;DR
This study finds that certain patient factors, not endovascular techniques, are linked to worse outcomes after successful revascularization in patients with severe leg ischemia.
Contribution
Identifies patient-specific risk factors for adverse outcomes after successful endovascular revascularization in CLTI patients.
Findings
End-stage renal disease and wounds at or above the ankle increase risk of MALE or death after femoral-popliteal interventions.
Diabetes and longer procedure time are associated with worse outcomes after below-knee popliteal-tibial interventions.
Endovascular techniques like drug-coated devices do not consistently affect MALE or death risk in CLTI patients.
Abstract
Chronic limb-threatening ischemia (CLTI) has a high risk of limb amputation without revascularization. In the Best Surgical Therapy in CLTI (BEST-CLI) trial, endovascular revascularization had a higher risk of major adverse limb events (MALE) or death compared with surgical bypass with a good quality vein. However, endovascular revascularization is still required for patients with poor vein options or high surgical risk. We assessed the factors related to MALE or death among patients with a successful endovascular intervention in the BEST-CLI trial. All patients with successful endovascular revascularization in the BEST-CLI trial were followed for a mean of 2.7 years. Baseline patient characteristics, lesion characteristics, and endovascular techniques were compared with the subsequent risk of MALE or death. Multivariable models estimated hazard ratios (HRs) and 95% CIs from Cox…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
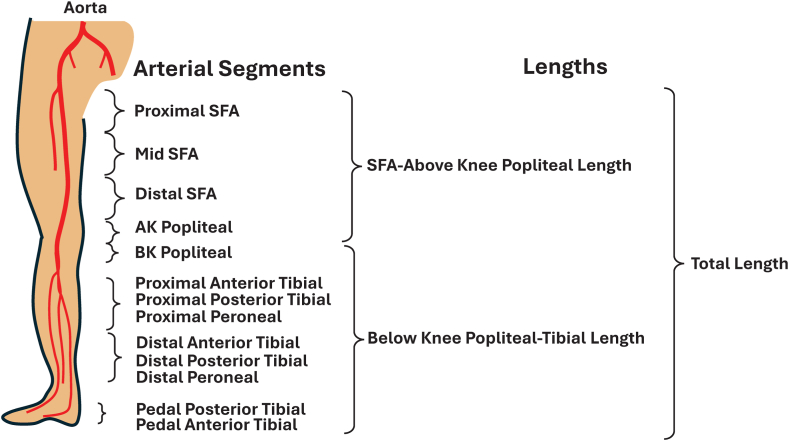 Figure 1
Figure 1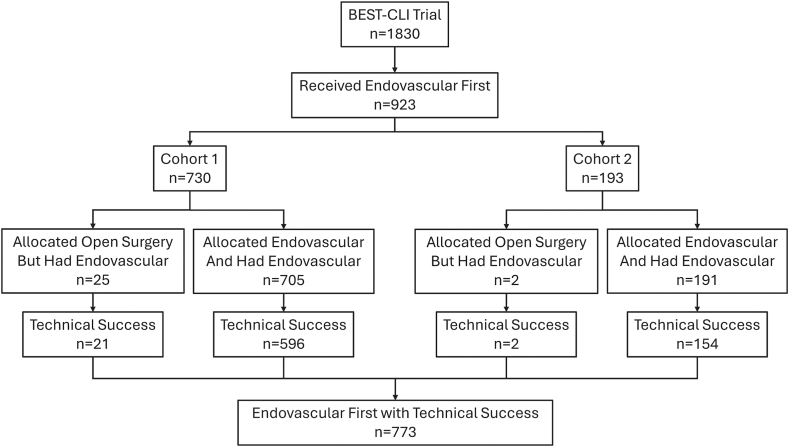 Figure 2
Figure 2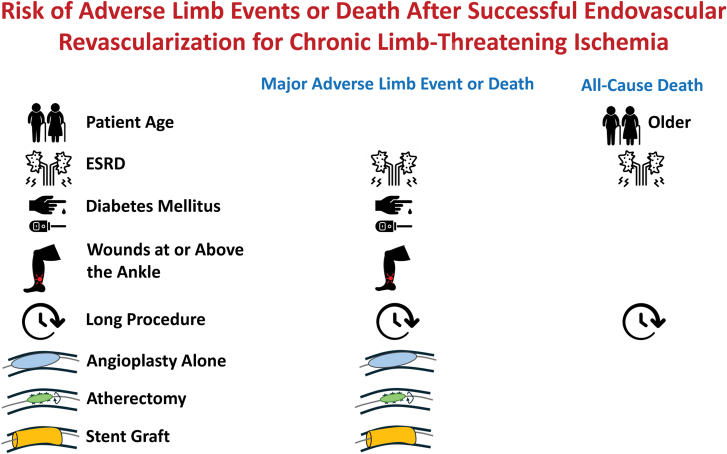 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Vascular Procedures and Complications · Aortic aneurysm repair treatments
Introduction
Chronic limb-threatening ischemia (CLTI) is associated with a high risk of major amputation and death.1^,^2 Revascularization improves limb preservation and maintains functional independence in patients.
There are a multitude of endovascular revascularization options for peripheral artery disease (PAD), including plain balloon angioplasty, drug-coated balloons, drug-eluting stents, bare-metal stents, stent grafts, and atherectomy.3 These endovascular therapies are used either as definitive treatment or as adjunctive therapies to modify plaque (eg, atherectomy or laser) in arteries above and below the knee. Recently, 2 major clinical trials, the Best Endovascular versus Best Surgical Therapy in Patients with Clinical Limb Ischemia (BEST-CLI) trial4 and the Bypass versus Angioplasty for Severe Ischemia of the Leg - 2 (BASIL-2) trial,5 compared infrainguinal surgical bypass versus endovascular revascularization in patients with CLTI who were deemed eligible for both approaches. The studies came to divergent conclusions, with endovascular revascularization having worse limb and survival outcomes than surgical bypass with greater saphenous vein in BEST-CLI, similar outcomes to bypass with other conduits in BEST-CLI, and better outcomes to bypass in BASIL-2. Trying to synthesize these inconsistent results has proved difficult,6 with the endovascular community raising questions about endovascular treatment in BEST-CLI, including the severity of arterial disease, the use of advanced endovascular techniques, and the use of drug-eluting stents and balloons.
The objective of this post-hoc analysis of the BEST-CLI trial was to describe the patient and limb characteristics and endovascular techniques used in patients with successful index endovascular procedures. We assessed the relationship of these factors to MALE or death over the duration of the study.
Methods
This was an as-treated analysis of all the subjects in the BEST-CLI trial (ClinicalTrials.gov number NCT02060630) who had a successful endovascular revascularization as their initial mode of revascularization. Procedural success was defined as the ability to cross the lesion with a wire, a residual stenosis <50%, and in-line flow to the foot in at least 1 tibial artery.4 Patients who experienced endovascular technical failure were reported previously and excluded from this analysis.7 The trial protocol was approved by the ethics committee at each participating site, and study details were reported in the main results of the BEST-CLI trial.4
Patient population
Patients included were 18 years or older with CLTI defined as arterial insufficiency of the lower limb with ischemic foot pain at rest, a nonhealing ulcer, or gangrene and corroborated with hemodynamic criteria. Patients with successful endovascular revascularization included 750 subjects randomized to endovascular therapy in either of the 2 cohorts, and 23 patients who were randomized to infrainguinal bypass, but who received endovascular revascularization instead. Patient characteristics included risk factors for atherosclerosis, comorbidities, medication use, prior interventions, physical examination, and lower extremity noninvasive studies.4
Limb characteristics
Limb characteristics included the presence of ischemic rest pain and tissue loss, wound location, and the wound, ischemia, and foot infection (WIfI) wound classification.8 Procedural factors included access sites, procedural time, the endovascular techniques used, and the use of closure devices. Complications included arterial thrombosis, embolization, dissection, or perforation during the procedure.
The lower extremity arterial tree was divided into 3 superficial femoral artery (SFA), 2 popliteal artery, 6 tibial artery, and 2 pedal artery segments (Figure 1). For each segment, the operators visually estimated the most severe stenosis or occlusion and lesion length. Since device use was markedly different for below-knee versus above-knee interventions, we generated a variable termed “SFA-above-knee popliteal artery” and described the most severe stenosis and the sum of lesion lengths treated in these segments. Similarly, a second variable of “below-knee popliteal artery-tibial” described the most severe stenosis and the sum of the lesion lengths treated in these segments. Analyses on device use were stratified by these 2 regions, acknowledging that some patients had interventions in both regions. Total lesion length was the sum of the SFA to above–knee popliteal length and the below-knee-to-popliteal artery-tibial length (Figure 1). In multivariable analyses, lesion lengths for SFA-popliteal lesions and popliteal-tibial lesions were categorized as <100 mm, 100 <200 mm, and >200 mm.Figure 1Arterial segments used to determine lengths in the analysis. AK, above knee; BK, below knee; SFA, superficial femoral artery.
Endovascular technique
Endovascular techniques used were recorded for every treated infrainguinal arterial segment. Plain angioplasty alone was defined as the use of balloon dilation in any given segment without any additional techniques. Other techniques per segment included any use of plain or cutting balloon angioplasty, bare-metal stent, drug-coated balloon, drug-eluting stent, stent graft, laser atherectomy, other atherectomy, mechanical thrombectomy, or any combination of these techniques. For multivariable analyses, we compared the use versus no use of these devices. The use of luminal reentry devices and embolic protection devices was also recorded.
Outcomes
The primary outcome for this analysis was MALE or death, with MALE defined as above-ankle amputation of the index limb, or a major index-limb reintervention (new bypass, interposition graft revision, thrombectomy, or thrombolysis).4 Major index-limb reinterventions were adjudicated by an independent multidisciplinary clinical-events committee as part of the parent BEST-CLI trial. We also assessed risk factors for all-cause death over follow-up. Patients were followed up to 7 years for a median of 2.7 years (IQR, 1.6-4.0).
Statistical analysis
Patient, limb, and endovascular techniques were described using means and standard deviations or percent, as appropriate. Differences between patients who did versus who did not have a subsequent MALE or death were assessed using χ^2^ tests for categorical data and summarized as numbers and percentages. Continuous data are reported as means with standard deviations or as medians with interquartile ranges and compared using t tests or Kruskal-Wallis tests. Cox proportional hazards models were used to determine univariable and multivariable hazard ratios (HRs) and 95% CI for the outcomes according to patient, cohort 1 or 2, and endovascular factors stratified by patients having interventions above or below the knee. Variables were entered into the multivariable models based on clinical significance or if they had a P value < .2 in the descriptive tables. These analyses were exploratory and were not adjusted for multiple tests of significance. A P value of <.05 was used for statistical significance. All statistical analyses were performed with SAS version 9.4 (SAS Institute).
Results
Of the 1830 patients enrolled in the BEST-CLI trial, 923 (50%) had endovascular revascularization as their first revascularization treatment, including 27 subjects who were initially randomized to the surgical bypass arm. Of these, 773 (84%) subjects had a successful endovascular revascularization at the index procedure (Figure 2).Figure 2Flow diagram for defining the cohort of subjects receiving a successful endovascular revascularization as the first procedure.
Patient and limb characteristics
Table 1 compares the baseline characteristics of patients who did and did not experience a MALE or death event following successful endovascular therapy. Subjects who experienced a MALE or death event in follow-up were more likely to have diabetes mellitus, heart failure, or end-stage renal disease (ESRD). Table 2 similarly compares the limb and lesion characteristics among patients who did and did not experience a MALE event after endovascular therapy. Of all patients, 95% had WIfI wound stage of 1 or higher, 82% had treatment in the SFA-above-knee popliteal artery territory, and 62% had treatment in the below-knee popliteal artery-tibial territory, and 45% had treatment in both territories. MALE or death was not related to lesion length, total occlusions, total contrast volume, or the use of arterial closure devices (Table 2). However, MALE or death was associated with longer procedure times (P = .0004). Complications were rare, but only arterial thrombus was related to a MALE or death (P = .012).Table 1. Baseline patient characteristics by subsequent major adverse limb event or death.CharacteristicsMALE or deathn = 381No MALE or deathn = 392P valueAge, y66.9 ± 10.266.9 ± 9.6.73Female sex107 (28)124 (32).28Race.16 White266 (70)287 (74) Black70 (19)74 (19) Other37 (10)21 (5) Mixed6 (2)6 (2)Ethnicity.50 Hispanic61 (16)56 (14) Non-Hispanic320 (84)336 (86)BMI, kg/m^2^28.1 ± 6.028.1 ± 6.0.95Hypertension334 (88)336 (86).43Hyperlipidemia276 (72)280 (71).75Diabetes282 (74)253 (65).004Current smoking139 (37)137 (35).66Prior infrainguinal revascularization of the index limb23 (6)23 (6).92Heart failure33 (9)14 (4).003Prior stroke57 (15)48 (12).27COPD67 (18)52 (13).10End-stage renal disease63 (17)23 (7)<.0001Medications Statin270 (71)278 (71).99 Aspirin252 (66)274 (70).26 Clopidogrel99 (26)99 (25).82 Prasugrel2 (1)2 (1).98 Ticagrelor8 (2)2 (1).05 Direct oral anticoagulant18 (5)15 (4).54 Warfarin27 (7)26 (7).80Values are mean ± SD or n (%).BMI, body mass index; COPD, chronic obstructive pulmonary disease; MALE, major adverse limb events.Table 2. Baseline limb and lesion characteristics in patients by subsequent major adverse limb event or death.CharacteristicsMALE or deathn = 381No MALE or deathn = 392P valueAnkle-brachial index0.60 ± 0.310.60 ± 0.32.46Ischemic rest pain261 (69)244 (62).07Tissue loss152 (78)431 (75).29Worst wound location.19 No wounds69 (18)91 (24) Any toe wound187 (50)194 (50) Forefoot or hindfoot wound81 (22)77 (20) Ankle or above-ankle wound38 (10)23 (6)WIfI wound stage.07 0 (no ulcer)70 (19)92 (24) 1 (small shallow ulcer)158 (43)169 (44) 2 (deep ulcer with exposed bone)112 (30)105 (28) 3 (extensive ulcer forefoot/heel)29 (8)16 (4)Lesion characteristics SFA or above-knee popliteal artery320 (84)316 (81).22 Below-knee popliteal or tibial artery249 (65)231 (59).07 Total occlusion in SFA to above-knee popliteal artery segment222 (69)226 (72).40 Total occlusion in below-knee popliteal to tibial artery segment133 (53)137 (60).56 Total lesion length, mm245 ± 186227 ± 171.21 SFA to above–knee popliteal artery length, mm188 ± 139171 ± 132.12 Below–knee popliteal to tibial artery length, mm132 ± 137151 ± 152.29Procedural characteristics Primary Antegrade access150 (39)133 (34).12 Total procedure time, minutes171 ± 101148 ± 89.0004 Contrast volume, mL119 ± 85115 ± 79.82 Access closure device.43 None140 (37)116 (30) Perclose60 (16)60 (15) Starclose26 (7)29 (7) Angioseal74 (20)83 (21) Mynx60 (16)76 (19) Other15 (4)21 (5)Complications Arterial thrombus16 (4)5 (1).012 Arterial embolization12 (3)14 (4).75 Flow-limiting dissection39 (10)36 (9).62 Perforation or Rupture7 (2)16 (4).07Values are mean ± SD or n (%).WIfI, wound, ischemia, and foot infection.
Endovascular techniques
Table 3 shows the use of various endovascular techniques in combinations of different arteries by patient treated. Treatments in multiple arteries were common, with treatment of all 3 arteries (SFA, popliteal, and tibial) in 182 (24%) patients, and 2 arteries in 329 (43%) patients. Plain balloon angioplasty alone was used in only 123 (16%) cases and most commonly in the infrapopliteal arteries. Drug-coated balloons were used in 245 (32%), self-expanding drug-eluting stents were used in 132 (17%), and balloon-expandable drug-eluting stents were used in 89 (12%) patients.Table 3. Endovascular procedure characteristics by artery group.Artery groupTotalSFA alonePopliteal aloneTibial/peroneal aloneSFA and poplitealSFA and tibial/peronealPopliteal and tibial/peronealSFA and popliteal and tibial/peronealN139181041846481182772aAngioplasty aloneb10 (7)1 (6)63 (61)8 (4)6 (9)16 (20)19 (10)123 (16)Angioplasty—standard balloonb84 (61)10 (56)97 (93)121 (66)60 (94)72 (89)168 (92)612 (79)Angioplasty - cutting balloon8 (6)0 (0)5 (5)9 (5)3 (5)3 (4)13 (7)41 (5)Angioplasty drug-coated balloon42 (30)6 (33)5 (5)66 (36)17 (27)39 (48)70 (39)245 (32)Stent bare–metal self- expanding66 (48)6 (33)0 (0)93 (51)28 (44)17 (21)82 (45)292 (38)Stent bare–metal balloon expandible10 (7)2 (11)3 (3)18 (10)3 (5)0 (0)18 (10)54 (7)Stent drug–eluting self-expanding34 (25)2 (11)6 (6)36 (20)13 (20)6 (7)35 (19)132 (17)Stent drug–eluting balloon expandible14 (10)0 (0)17 (16)6 (3)10 (16)10 (12)32 (18)89 (12)Any drug eluting/coated device80 (58)8 (44)28 (27)98 (53)31 (48)48 (59)112 (62)405 (53)Stent graft self-expanding16 (12)2 (11)1 (1)32 (17)5 (8)1 (1)7 (4)64 (8)Stent graft balloon expandible3 (2)2 (11)0 (0)8 (4)1 (2)0 (0)1 (1)15 (2)Laser2 (1)1 (6)0 (0)4 (2)1 (2)3 (4)4 (2)15 (2)Luminal reentry device5 (4)0 (0)0 (0)3 (2)0 (0)0 (0)3 (2)11 (1)Mechanical Thrombectomy0 (0)1 (6)0 (0)3 (2)4 (6)1 (1)7 (4)16 (2)Angioplasty alone includes standard balloon or cutting or scoring balloon with no other interventions. Several of the other interventions could have occurred in any artery, thus the total number of treatments exceeds the numbers of subjects in each arterial group.Values are n (%).aOne subject had plain balloon angioplasty to the common femoral artery.bAngioplasty alone = no other device used. Angioplasty—standard balloon = balloon angioplasty with another treatment.
Table 4 shows the endovascular techniques used at the index revascularization divided into above- and below-knee interventions according to subsequent MALE or death. The most common techniques in the SFA-above-knee popliteal territory, ranked from the highest to the lowest, were bare-metal stent (43%), drug-coated balloons (34%), plain balloon angioplasty (24%), drug-eluting stents (18%), atherectomy (12%), and stent grafts (10%). The most common techniques in the below-knee popliteal-tibial territory were plain balloon angioplasty (74%), drug-coated balloons (18%), atherectomy (12%), bare-metal stents (8%), and drug-eluting stents (5%). Combinations of atherectomy and drug-coated balloons were used in 3% to 8% of lesions, and combinations of drug-coated balloons with bare-metal stents in 0% to 10% of lesions. At least 1 drug-eluting/coated technology was used in 330 (52%) interventions in the SFA-above-knee popliteal interventions and 157 (33%) below-knee popliteal to tibial interventions.Table 4. Univariable associations for MALE or death according to endovascular techniques used to treat lesions in the superficial femoral to above–knee popliteal artery and the below–knee popliteal to tibial artery segments.MALE or deathNo MALE or deathP valueSFA to above–knee popliteal arteryn = 320n = 316 Any plain angioplasty84 (26)69 (22).19 Any atherectomy40 (13)32 (10).35 Any bare-metal stent136 (43)132 (42).85 Any drug-coated balloon108 (34)104 (33).82 Any drug-eluting stent58 (18)54 (17).73 Any drug-coated/eluting device168 (53)162 (51).76 Any stent graft34 (11)25 (8).24 Any laser12 (4)2 (1).007 Any mechanical thrombectomy device8 (3)3 (1).22 Any luminal reentry device1 (0.3)8 (3).02 Combination treatment Atherectomy with drug-coated balloon24 (8)21 (7).67 Drug-coated balloon with bare-metal stent34 (11)21 (7).07Below-knee popliteal artery to tibial arteryn = 249n = 231 Any plain angioplasty182 (73)176 (76).44 Any atherectomy31 (12)26 (11).69 Any bare-metal stent21 (8)15 (7).42 Any drug-coated balloon42 (17)44 (19).53 Any drug-eluting stent16 (6)10 (4).31 Any drug-coated/eluting device84 (34)73 (32).62 Any stent graft1 (0.4)4 (2).20 Any mechanical thrombectomy device8 (3)2 (1).11 Any luminal reentry device1 (0.4)1 (0.4)>.99 Combination treatment Atherectomy with drug-coated balloon8 (3)9 (4).81 Drug-coated balloon with bare-metal stent5 (2)0 (0).06Multiple combinations used in some patients.Values are n (%).
In the SFA-above-knee popliteal artery territory, MALE or death events were higher in patients having laser atherectomy compared with no laser atherectomy (4% vs 1%, P = .007) and lower with the use of luminal reentry devices (0.3% vs 3%, P = .02), but these techniques were used rarely. In the below-knee popliteal artery-tibial territory, MALE or death was not associated with any endovascular technique.
Subjects in cohort 1 had a similar risk of MALE death compared with those in cohort 2 (HR, 0.98, 95% CI, 0.68, 1.41). Therefore, this variable was not included in the multivariable models.
Multivariable models
Table 5 shows HR from the multivariable analyses for the primary outcome of MALE or death related to patient, limb, and procedural characteristics among patients who had 1 or more lesions treated in the SFA-above-knee popliteal artery segments or the below-knee popliteal-tibial artery segments. For patients with above-knee interventions, the risk of MALE or death was higher with ESRD (HR, 1.64, 95% CI, 1.17, 2.29), a wound at or above the ankle (HR, 2.13, 95% CI, 1.38, 3.29), longer procedural times (HR, 1.15 per 120 minutes, 95% CI, 1.02, 1.03), angioplasty alone (HR, 1.38, 95% CI, 1.04, 1.83), and atherectomy or laser (HR, 1.59, 95% CI, 1.05, 2.41). For patients with below-knee interventions, the risk of MALE or death was higher with diabetes (HR, 1.69, 95% CI, 1.18, 2.43), ESRD (HR, 1.80, 95% CI, 1.26, 2.57), a wound above the ankle (HR, 1.90, 95% CI, 1.10, 3.27), and longer procedure times (HR, 1.28 per 120 minutes, 95% CI, 1.11, 1.47).Table 5. Multivariable risk of major adverse limb events (MALE) or death according to patient factors in 636 patients having successful superficial femoral-popliteal artery endovascular interventions and 480 patients having successful popliteal-tibial artery endovascular interventions.VariableMALE or deathSuperficial femoral-popliteal artery (n = 636)Popliteal-tibial artery (n = 480)No. of events320249Patient factors Age, per y0.99 (0.98-1.01)1.00 (0.99-1.02) Race WhiteReferenceReference Black1.08 (0.79-1.47)0.96 (0.69-1.34) Mixed0.38 (0.09-1.56)0.71 (0.25-2.01) Other1.26 (0.84-1.88)1.09 (0.71-1.66) Diabetes1.26 (0.97-1.65)1.69 (1.18-2.43)a End-stage renal disease1.64 (1.17-2.29)a1.80 (1.26-2.57)a Current smoker1.09 (0.85-1.39)1.26 (0.91-1.73) Worst wound location Ankle or above vs none2.13 (1.38-3.29)a1.90 (1.10-3.27)b Any toe vs none1.03 (0.76-1.40)0.80 (0.56-1.16) Fore/hind foot vs none1.20 (0.83-1.72)0.78 (0.52-1.19)Procedural factors Procedure time at 120 minutes1.15 (1.02-1.03)b1.28 (1.11-1.47)a SFA-popliteal length 100-200 mm vs <100 mm0.92 (0.68-1.26)1.09 (0.79-1.50) >200 mm vs <100 mm1.04 (0.79-1.37)0.83 (0.59-1.18) Angioplasty alone1.38 (1.04-1.83)b0.87 (0.60-1.26) Bare-metal stent1.19 (0.88-1.60)1.07 (0.62-1.87) DCB1.02 (0.73-1.43)0.74 (0.49-1.14) Drug-eluting stent1.15 (0.83-1.59)1.15 (0.66-2.03) Stent graft1.47 (1.00-2.18)0.25 (0.03-1.87) Atherectomy or laser1.59 (1.05-2.41)b1.16 (0.75-1.79) Atherectomy and DCB0.74 (0.40-1.36)1.11 (0.43-2.85) BMS and DCB1.06 (0.65-1.75)2.51 (0.82-7.67) Mechanical thrombectomy1.91 (0.92-3.94)1.65 (0.75-3.67)Values are hazard ratio (95% CI).DCB, drug-coated balloon; SFA, superficial femoral artery.aP < .01.bP < .05.
Table 6 shows the HR from the multivariable analyses for all-cause death. For patients with above-knee interventions, the risk of death was higher for greater age (HR =1 .03 per year, 95% CI, 1.02, 1.05), ESRD (HR, 2.36, 95% CI, 1.61, 3.47), a wound in the fore/hind foot (HR, 1.70, 95% CI, 1.09, 2.67), and longer procedural time (HR, 1.19 per 120 minutes, 95% CI, 1.02, 1.40). For patients with below-knee interventions, the risk of death was higher for greater age (HR, 1.04 per year, 95% CI, 1.02, 1.05), ESRD (HR, 2.60, 95% CI, 1.74, 3.89), and longer procedural time (HR, 1.20 per 120 minutes, 95% CI, 1.01, 1.41). The use of bare-metal stents with drug-coated balloon use was also associated with a higher risk below the knee (HR, 4.77, 95% CI, 1.18, 19.38), but the wide CI indicate the small number of patients with this intervention.Table 6. Multivariable risk of all-cause death according to patient factors in 636 patients having successful superficial femoral-popliteal artery endovascular interventions and 480 patients having successful popliteal-tibial artery endovascular interventions.VariableAll-cause deathSuperficial femoral-popliteal artery n = 636Popliteal-tibial artery n = 480The No. of events209175Patient factors Age, per y1.03 (1.02-1.05)∗1.04 (1.02, 1.05)∗ Race WhiteReferenceReference Black1.26 (0.85-1.86)0.91 (0.61-1.37) Mixed0.81 (0.19-3.37)1.05 (0.36-3.10) Other1.11 (0.67-1.85)1.24 (0.75-2.03) Diabetes1.37 (0.97-1.94)1.40 (0.89-2.21) End-stage renal disease2.36 (1.61-3.47)a2.60 (1.74-3.89)a Current smoker1.09 (0.79-1.51)1.07 (0.72-1.60) Worst wound location Ankle or above vs none1.66 (0.92-2.97)1.92 (0.93-3.99) Any toe vs none1.02 (0.68-1.53)1.14 (0.69-1.87) Fore/hind foot vs none1.70 (1.09-2.67)b1.54 (0.90-2.63)Procedural factors Procedure time at 120 minutes1.19 (1.02-1.40)b1.20 (1.01-1.41)b SFA-popliteal length 100-200 mm vs <100 mm0.86 (0.58-1.26)0.97 (0.65-1.45) >200 mm vs <100 mm0.91 (0.64-1.29)0.57 (0.37-0.89) Angioplasty alone1.41 (0.99-2.00)1.24 (0.79-2.29) Bare-metal stent1.05 (0.72-1.53)1.42 (0.76-2.68) DCB1.13 (0.74-1.73)1.04 (0.63-1.72) Drug-eluting stent0.89 (0.58-1.37)1.25 (0.60-2.58) Stent graft1.25 (0.76-2.06)0.62 (0.08-4.72) Atherectomy or laser1.06 (0.60-1.87)1.34 (0.79-2.29) Atherectomy and DCB0.79 (0.35-1.80)0.35 (0.07-1.70) BMS and DCB1.27 (0.68-2.37)4.77 (1.18-19.38)b Mechanical thrombectomy1.04 (0.37-2.93)0.80 (0.23-2.79)Values are hazard ratio (95% CI).DCB, drug-coated balloon; SFA, superficial femoral artery.aP < .01.bP < .05.
Overall, the patient characteristics were more strongly and consistently related to adverse outcomes than the endovascular techniques. Multivariable models excluding procedure time yielded similar results.
Discussion
This analysis of patients who had successful endovascular index revascularization in the BEST-CLI trial describes the wide variety of endovascular techniques that were used. Patients with successful endovascular procedures in the trial had a wide range of lesion lengths, and many procedures required advanced endovascular techniques, including drug-coated balloons and stents. Although some experienced endovascular specialists may have used more advanced techniques, including drug-coated technologies or completed endovascular procedures in a shorter time (which was consistently associated with outcomes), we found no consistent effect of the devices on MALE or death in the BEST-CLI study. Overall, patient factors rather than procedural factors were more strongly associated with adverse outcomes.
Patient and wound factors
Patient factors associated with MALE or death included diabetes mellitus, ESRD, and a wound at or above the ankle. These factors have also been identified in previous studies.2^,^9^,^10 However, the WIfI wound stage was not related to MALE or death, in contrast to other studies of endovascular revascularization for PAD, where it was associated with poorer healing and mortality.11, 12, 13, 14 Other studies show that wound severity is the most important factor in the WIfI score for determining the risk of adverse limb outcomes and mortality.15^,^16 Our findings may reflect differences in the patient population or wound care between BEST-CLI and other observational studies. For example, the BEST-CLI study required subjects to have a life expectancy of more than 2 years and have an acceptable risk for open surgical revascularization. These criteria would have excluded many patients with a high risk of death because of comorbidities, frailty, poor nutrition, or lack of distal arterial targets who are more commonly in the highest WIfI grades.17, 18, 19
Lesion and procedural factors
Unlike other studies,2^,^20^,^21 we found that more complex vascular disease, manifested as longer lesion lengths and chronic total occlusions of the SFA-above-knee popliteal segment, was not associated with MALE or death in univariable or multivariable analyses. This may relate to the method of assessing lesion length, which was based on visual estimates by the operators. That stated, our results are consistent with a prior study where lesion length was related to repeat revascularization, but not MALE.22
MALE or death after SFA-above-knee popliteal artery interventions occurred more often in patients having angioplasty alone, atherectomy or laser, and stent graft placement. Atherectomy is associated with a higher risk of distal embolization in large registries.23^,^24 However, the use of these devices is also more common in complex and calcified diseases.22^,^25 Stent grafts used above the knee were also associated with a higher risk of major reintervention and an increased risk of MALE. Meta-analyses suggest that covered stents offer no benefit in preventing MALE26 and may be associated with worse outcomes than drug-eluting stents.27 However, like atherectomy, they are used for arterial perforation, and their use may reflect more complex disease or procedures. Despite these findings, MALE was not higher in patients having these endovascular procedures in the below-knee-tibial region, and none were related to all-cause death in either region. The lack of consistent relationships to these end points and the potential for reverse causation (complex lesions require advanced techniques) support the use of adjunctive therapies if they are required for optimal plaque modification (Graphic Abstract).
Drug-coated balloons or drug-eluting stents were used in 52% of SFA-above-knee popliteal interventions and 33% of below-knee popliteal artery to tibial interventions. During the BEST-CLI trial, there were concerns about the safety of drug-coated technologies, and there were no approved drug-coated balloons for use below the knee in the United States. These likely limited their overall use in the trial, although their use was comparable with data from national registries reporting over a similar time as the trial.28^,^29 The efficacy of drug-coated technologies is less well known for CLTI, but as there was no consistent difference in the risk of MALE or all-cause death with drug-coated/eluting devices above or below the knee, this adds to more recent trial data and registries supporting their safety.30, 31, 32, 33, 34, 35, 36, 37, 38 Although short-term studies suggest improved patency with drug-eluting technologies used in below-the-knee endovascular revascularization,39, 40, 41 their efficacy with longer follow-up requires further elaboration.42 Our analysis did provide some evidence to support the use of drug-coated balloons after atherectomy, which had a significantly lower risk of MALE compared with atherectomy alone in the SFA-popliteal artery distribution. Although this combination is intuitively attractive, other studies have failed to show long-term benefit compared with drug-coated balloons alone.43^,^44
Markers of extent and complexity of disease
A unifying hypothesis to explain the patient and procedural factors associated with adverse limb events could be their relationship to the extent and complexity of macrovascular and microvascular PAD. Diabetes mellitus and ESRD are well known to impair the microcirculation and cause wounds disproportionally to other atherosclerosis risk factors.45, 46, 47 Other studies indicate that wounds and other factors related to microvascular disease may be more important determinants of major adverse limb outcomes in CLTI.22 Long procedural times and atherectomy could be markers for more diffuse or calcified atherosclerosis, typical of more advanced stages of disease, which in itself is related to a higher risk of adverse limb outcomes.23^,^24^,^48 Thus, differences in outcomes between endovascular techniques likely reflect the use of some technologies (eg, atherectomy) in more complex disease (Central Illustration).Central IllustrationFactors related to adverse outcomes after successful endovascular revascularization for chroniclimb-threateningischemia (CLTI) in theBEST-CLIstudy. ESRD, end-stage renal disease.
Limitations
This analysis of the BEST-CLI study was an observational design, and the results may include unknown confounders. The pragmatic design of the trial, incorporating a wide range of permutations of endovascular devices, renders it challenging to make direct comparisons of individual device efficacy or assess the numerous permutations of different combinations of treatment. However, we were able to describe and assess the risk of some of the more common combinations of devices. The limitations of visual estimates of lesion length and complexity will be addressed in a recently funded assessment of baseline angiograms from the BEST-CLI study. Some associations may be affected by confounding, for example, devices such as atherectomy, stent grafts, and mechanical thrombectomy are likely indicators of more complex and/or calcified disease. As such, their relationships to adverse limb outcomes may reflect the extent and severity of the underlying disease rather than the direct effects of these devices. Similarly, longer procedure times could also reflect lesion complexity or operator experience in endovascular procedures.
Conclusions
A wide variety of endovascular techniques and lesion severity were used in cases of successful endovascular revascularization in the BEST-CLI study. The relationships of patient and endovascular techniques to adverse outcomes likely reflect the extent and severity of PAD and identify patients who may benefit from closer surveillance after endovascular revascularization. There were no consistent relationships between the endovascular techniques, including drug-coated balloons and drug-eluting stents, and major adverse limb outcomes or death in this study of high-risk patients with CLTI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Farber A.Chronic limb-threatening ischemia N Engl J Med 379201817118010.1056/NEJ Mcp 170932629996085 · doi ↗ · pubmed ↗
- 2Kinlay S.Sobieszczyk P.Eisenhauer A.C.Ostrowski S.Todoran T.M.Patient and limb outcomes 10 years after endovascular revascularization of the superficial femoral artery for peripheral artery disease: the Boston Femoral Artery Endovascular Revascularization Outcomes (Boston FAROUT) study Vasc Med 28202329029810.1177/1358863 X 23117405237211818 PMC 10527919 · doi ↗ · pubmed ↗
- 3Thanigaimani S.Sun D.Ahmad U.Anning N.Tian K.Golledge J.Network meta-analysis of randomised controlled trials comparing the outcomes of different endovascular revascularisation treatments for infra-inguinal peripheral arterial disease causing chronic limb threatening ischaemia Eur J Vasc Endovasc Surg 68202424625410.1016/j.ejvs.2024.05.01438754723 · doi ↗ · pubmed ↗
- 4Farber A.Menard M.T.Conte M.S.Surgery or endovascular therapy for chronic limb-threatening ischemia N Engl J Med 38720222305231610.1056/NEJ Moa 220789936342173 · doi ↗ · pubmed ↗
- 5Bradbury A.W.Moakes C.A.Popplewell M.A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): an open-label, randomised, multicentre, phase 3 trial Lancet 40120231798180910.1016/S 0140-6736(23)00462-237116524 · doi ↗ · pubmed ↗
- 6Kinlay S.Revascularization for chronic limb-threatening ischemia-synthesizing inconsistency J Soc Cardiovasc Angiogr Interv 45202510262310.1016/j.jscai.2025.102623 PMC 1212606540454267 · doi ↗ · pubmed ↗
- 7Powell R.J.Farber A.Doros G.The incidence and consequences of endovascular technical failure in patients with chronic limb-threatening ischemia: results from the best endovascular versus best surgical therapy in patients with critical limb-threatening ischemia (BEST-CLI) trial J Vasc Interv Radiol 366202595095910.1016/j.jvir.2025.02.02040015448 · doi ↗ · pubmed ↗
- 8Mills J.L.Sr.Conte M.S.Armstrong D.G.The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (W If I)J Vasc Surg 592014220234.e 110.1016/j.jvs.2013.08.00324126108 · doi ↗ · pubmed ↗