Long-Term Outcomes of Transcatheter Versus Surgical Aortic Valve Replacement Among Patients With Prior Mediastinal Radiation
Hossam Elbenawi, Mahmoud Eisa, Muhammad Eltony, Omar Almaadawy, Ahmed El Shaer, Khaled Elfert, Ramzi Ibrahim, Jeremiah P. Depta, Karim M. Al Azizi, Chien-Jung Lin, Yiannis S. Chatzizisis, Stanislav Henkin, Martha Gulati, Andrew M. Goldsweig, Ayman Elbadawi, Islam Y. Elgendy

TL;DR
The study compares long-term outcomes of two heart valve replacement methods in patients previously treated with chest radiation.
Contribution
It provides the first multinational observational analysis of long-term outcomes of TAVR versus SAVR in patients with prior mediastinal radiation.
Findings
TAVR and SAVR showed similar 5-year mortality rates in patients with prior chest radiation.
No significant difference in stroke or hospitalization rates was found between TAVR and SAVR groups.
The results suggest TAVR is a viable option for patients with prior mediastinal radiation.
Abstract
Limited data suggest that transcatheter aortic valve replacement (TAVR) is associated with similar short-term outcomes to surgical aortic valve replacement (SAVR) among patients with a history of mediastinal radiation. However, the long-term outcomes of TAVR versus SAVR in this growing patient population remain unknown. We identified patients with a history of chest radiation who underwent isolated AVR using the multinational TriNetX database from 2010 through 2025. Propensity score matching was performed to account for differences in baseline characteristics. Outcomes included all-cause mortality, stroke, and all-cause hospitalization at 5 years. The analysis included 933 patients with prior chest radiation who underwent isolated AVR, of whom 785 (84.13%) underwent TAVR, and 148 (15.86%) underwent SAVR. After propensity score matching, 128 patients were included in each group. In the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
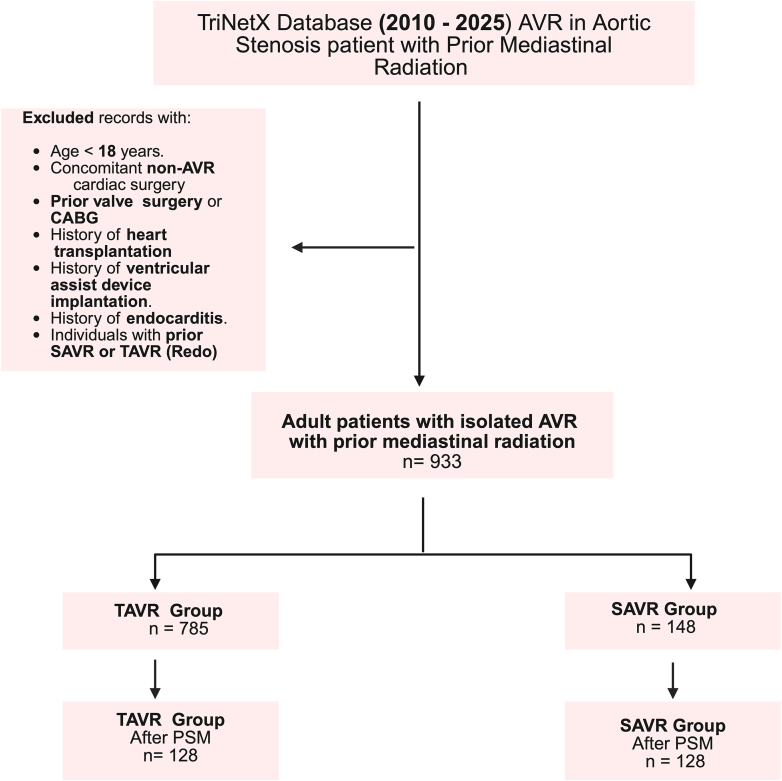 Figure 1
Figure 1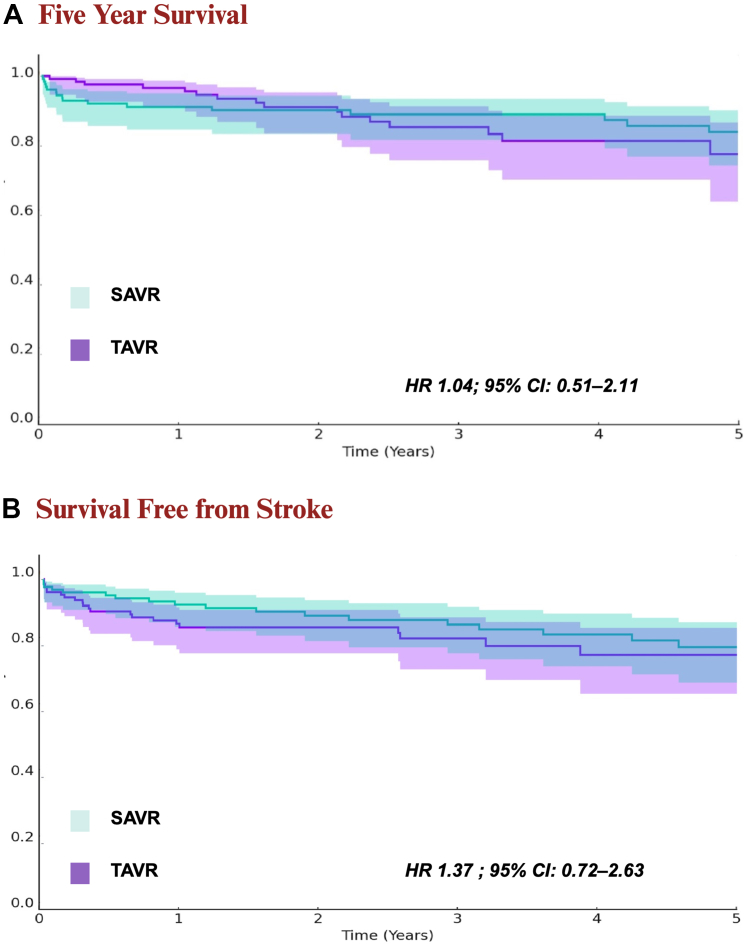 Figure 2
Figure 2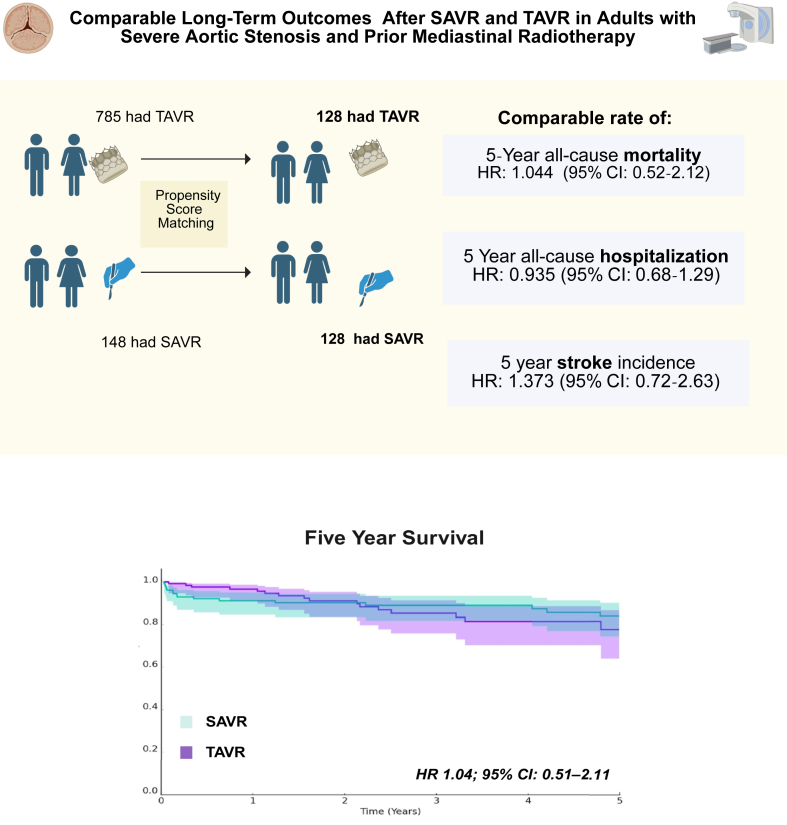 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Cardiac Imaging and Diagnostics · Management of metastatic bone disease
Introduction
Severe aortic valve stenosis may be a late complication of radiation-induced cardiac fibrosis, affecting approximately 25% of patients who have been exposed to mediastinal radiation.1 Patients with severe aortic stenosis and a history of mediastinal radiation exposure may experience significantly higher complications and mortality rates following surgical aortic valve replacement (SAVR) compared with those without prior radiation exposure.2 This elevated risk is likely due to radiation-related fibrosis of surrounding tissues (including pulmonary fibrosis) and contributes to the presence of multiple cardiac lesions, all of which increase morbidity and mortality following cardiac surgery.3
Irrespective of the surgical risk, transcatheter aortic valve replacement (TAVR) provides an alternative to SAVR for patients with symptomatic severe aortic stenosis4, 5, 6; however, patients with prior mediastinal radiation were largely underrepresented in the pivotal TAVR trials.7, 8, 9 Limited data have suggested that TAVR is associated with favorable short-term mortality and morbidity compared with SAVR among these patients.10, 11, 12 However, the long-term outcomes of TAVR vs SAVR in patients with prior mediastinal radiation remain unknown. To address this knowledge gap, we utilized the TriNetX database to assess long-term outcomes in patients with prior mediastinal radiation who underwent isolated transcatheter or surgical AVR.
Materials and methods
Data source and study population
We performed a retrospective, observational analysis using the TriNetX Research Network, which includes electronic health record data from more than 250 million patients across more than 120 healthcare organizations, primarily in the United States.13 Within this database, data from 69 US healthcare organizations were queried. Data were deidentified in accordance with the deidentification standard outlined in section x164.514(a) of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. Because this study used deidentified data, the study was exempt from the requirements of the institutional review board. The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies (Figure 1).14 The TriNetX database was queried using International Classification of Diseases, Tenth Revision Clinical Modification (ICD-10-CM) Procedure Coding System, Current Procedural Terminology (CPT), and RxNorm codes to identify the study cohort. The inclusion criteria included patients >18 years of age who had nonrheumatic aortic valve stenosis and underwent isolated AVR between January 2010 and January 2025, and had a history of prior mediastinal radiation. Prior mediastinal radiation was defined as a history of irradiation for malignant neoplasms of the breast, esophagus, thymus, heart, pleura, mediastinal lymphoma (including Hodgkin’s, non-Hodgkin’s, follicular, nonfollicular, and other lymphoid types), hematological malignancies, or malignant neoplasms of the bronchus and lung. We excluded patients who underwent concomitant non-AVR cardiac procedures, had a history of prior valve replacement (tricuspid valve, pulmonary valve, or mitral valve) or coronary artery bypass grafting, had a history of heart transplantation or ventricular assist device implantation, had a history of endocarditis, or had previously undergone SAVR or TAVR (redo procedures; Supplemental Appendix S1). We used the CPT code for only transfemoral TAVR. These administrative codes have been previously validated to identify patients with cancer conditions and those with prior radiation history.15, 16, 17 We stratified the cohort into 2 groups based on the modality of AVR:TAVR vs SAVR.Figure 1Study cohort and design reported per the Strengthening of the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. AVR, aortic valve replacement; CABG, coronary artery bypass grafting; TAVR, transcatheter aortic valve replacement; SAVR, surgical aortic valve replacement; PSM, propensity score matching.
Study outcomes
The primary outcome was all-cause mortality, whereas the secondary outcomes included all-cause hospitalization and ischemic stroke. Death was handled as a censoring event for nonfatal outcomes. Outcomes were analyzed up to 5 years following the index procedure (TAVR or SAVR).
Statistical analysis
Continuous variables are presented as mean ± SD and were compared using independent-samples t tests. Categorical variables are reported as frequency (percentage) and were compared using the χ^2^ test. To adjust for baseline characteristic differences between the 2 groups, propensity score matching (PSM) was conducted. Covariates were matched 1:1 using the greedy nearest neighbor matching algorithm with a caliper width of 0.1 pooled standardized mean difference (SMD). Any characteristic with an SMD of <0.1 was considered well-matched. The following covariates were included in the PSM: age at index procedure, race, sex, essential hypertension, diabetes mellitus, heart failure, chronic ischemic heart disease, dyslipidemia, history of nicotine dependence, left ventricular ejection fraction, estimated glomerular filtration rate, body mass index, hematocrit, atrial fibrillation and flutter, chronic lower respiratory diseases, carotid artery stenosis or occlusion, peripheral vascular disease, obstructive sleep apnea, use of beta blockers, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, statins, anticoagulants, and aspirin, and malignant neoplasms of the breast, lung, and lymphoid tissue. Adjusted HRs with 95% CIs were calculated for primary and secondary outcomes.
Cox proportional hazards regression model was conducted to evaluate the association between intervention strategy (TAVR vs SAVR) and long-term all-cause mortality, adjusting for relevant clinical covariates. The model included the following covariates based on clinical relevance and data availability: age at index, sex, race (White), left ventricular ejection fraction (LVEF), estimated glomerular filtration rate, hematocrit, and comorbidities including heart failure, diabetes mellitus, chronic kidney disease, chronic ischemic heart disease, peripheral vascular disease, atrial fibrillation, chronic lower respiratory disease, carotid artery stenosis, sleep apnea, history of smoking, and hematocrit. Cancer history included breast cancer, lung cancer, and lymphoid malignancy. Medication used at baseline, including beta blockers, renin-angiotensin system inhibitors, statins, aspirin, and anticoagulants, was incorporated into the model. Laboratory-based stratifications of LVEF, glomerular filtration rate, and hematocrit were done.
The survival analysis was performed by plotting Kaplan-Meier curves with log-rank tests to compare both cohorts. All tests were 2-tailed; a P value of .05 was considered statistically significant without the control of type I error for multiple endpoints. Statistical analyses were performed using the TriNetX online platform with R (Ross Ihaka and Robert Gentleman) for statistical computing. To address the differences in median follow-up time between the groups, time-to-event analyses, including Kaplan-Meier survival curves and Cox proportional hazards models, were employed to account for variable follow-up durations and censoring.
Results
Study population and baseline characteristics
A total of 933 patients (63.2% women) underwent isolated AVR across 69 healthcare organizations and were included in the study. Seven hundred eighty-five (84.1%) underwent TAVR, and 148 (15.8%) underwent SAVR. Before PSM, TAVR patients were significantly older than SAVR patients (76.1 ± 9.2 years vs 65.6 ± 9.8 years) and had more comorbidities, including hypertension (85.9% vs 77.0%), diabetes mellitus (41.3% vs 33.1%), chronic ischemic heart disease (82.2% vs 77.7%), heart failure (62.0% vs 42.6%), atrial fibrillation/flutter (35.4% vs 25.7%), smoking history (47.1% vs 31.8%), peripheral vascular disease (16.9% vs 8.8%), and carotid artery stenosis (27.3% vs 25.0%). Additionally, TAVR patients had a lower mean estimated glomerular filtration rate (65.1 ± 22.4 vs 71.2 ± 22.1) and a higher usage of beta blockers (72.5% vs 64.9%), statins (73.9% vs 62.2%), aspirin (78.7% vs 66.2%), and oral anticoagulants (90.1% vs 75%) (Table 1). Malignant neoplasms of the breast did not differ significantly between the 2 groups, although TAVR patients had a higher prevalence of malignant neoplasms of the lung and bronchus (23.8% vs 11.5%, P = .001) (Table 1). The propensity score matched 256 patients (128 patients in each group) with well-balanced demographics and baseline characteristics (SMD <0.1 for most covariates). The PSM cohort was comprised of 71.09% women and was predominantly White (89.06%) (Table 1). After propensity score matching, nearly all variables achieved standardized mean differences ≤0.10. LVEF and hematocrit exceeded 0.20, but the absolute differences between groups were small and not clinically meaningful. The median follow-up duration was 775.5 days (IQR, 189-1362) for the TAVR group and 1215 days (IQR, 531-1898) for the SAVR group. The missing data for key variables used in propensity score matching were excluded by the TriNetX platform, ensuring complete case analysis.Table 1. Baseline characteristics before and after propensity score matching.VariableBefore PSMAfter PSMTAVR (n = 785)SAVR (n = 148)P valueSMDTAVR (n = 128)SAVR (n = 128)SMDAge, y76.1 ± 9.265.6 ± 9.8<.0011.09767.6 ± 10.267.5 ± 8.70.013Female62.4% (490)67.6% (100).2340.10872.7% (93)69.5% (89)0.069White race84.8% (666)89.9% (133).1100.15288.3% (113)89.8% (115)0.050Hypertension85.9% (674)77.0% (114).0070.22979.7% (102)79.7% (102)<0.001Diabetes mellitus41.3% (324)33.1% (49).0630.17037.5% (48)34.4% (44)0.065Heart failure62.0% (487)42.6% (63)<.0010.39745.3% (58)43.8% (56)0.031Chronic ischemic heart disease82.2% (645)77.7% (115).2000.11277.3% (99)79.7% (102)0.057Breast cancer51.3% (403)54.1% (80).5440.05456.3% (72)57.8% (74)0.032Lung cancer23.8% (187)11.5% (17).0010.3289.4% (12)12.5% (16)0.100Lymphoid malignancy29.8% (234)39.9% (59).0160.21235.9% (46)35.9% (46)<0.001Peripheral vascular disease16.9% (133)8.8% (13).0120.2468.6% (11)9.4% (12)0.027Atrial fibrillation/flutter35.4% (278)25.7% (38).0220.21331.3% (40)28.9% (37)0.051Chronic lower respiratory disease45.6% (358)41.9% (62).4050.07539.1% (50)43% (55)0.079Smoking history47.1% (370)31.8% (47).0010.31936.7% (47)36.7% (47)<0.001Dyslipidemia83.9% (659)77.7% (115).0640.15980.5% (103)78.9% (101)0.039Carotid stenosis27.3% (214)25.0% (37).5690.05124.2% (31)24.2% (31)<0.001Sleep apnea21.5% (169)20.3% (30).7320.03123.4% (30)21.9% (28)0.037BMI, kg/m^2^28.9 ± 6.631.3 ± 7.3<.0010.33531.1 ± 7.030.8 ± 7.30.046Beta-blocking agents72.5% (569)64.9% (96).060.16566.4% (85)65.6% (84)0.016ACE-I/ARBs58.7% (461)53.4% (79).2270.10855.5% (71)53.9% (69)0.031Statins73.9% (580)62.2% (92).0040.25360.2% (77)61.7% (79)0.032Aspirin78.7% (618)66.2% (98).0010.28371.9% (92)67.2% (86)0.102Anticoagulants90.1% (707)75% (111)<.0010.40576.6% (98)79% (102)0.076Left ventricular ejection fraction, %59.7 ± 12.856.9±13.1.3290.21260.3 ± 11.357.6 ± 12.90.216Glomerular filtration rate, mL/min/1.73 m^2^65.1±22.471.2 ± 22.1.0030.27468.4 ±23.469.7 ±20.20.062Hematocrit37.5 ± 5.138.8 ± 5.3.0060.24837.5 ±5.338.8 ±5.20.228Continuous variables are presented as mean ± SD and categorical variables as % (n).BMI, body mass index; PSM, propensity score matching; SAVR, surgical aortic valve replacement; SMD, standardized mean difference; TAVR, transcatheter aortic valve replacement.
Outcomes
For the primary outcome, there was no significant difference in the rate of 5-year mortality between the TAVR and SAVR groups (11.7% vs 12.5%; HR, 1.044; 95% CI, 0.52-2.12; P = .91) (Table 2, Figure 2A). For secondary outcomes, there was no significant difference in the rate of all-cause inpatient nonelective hospitalizations between the 2 groups (TAVR vs SAVR: 56.3% vs 64.1%; HR, 0.94; 95% CI, 0.68-1.29; P = .65) (Table 2). The rate of ischemic stroke/transient ischemic attack was also similar between the 2 groups (TAVR vs SAVR: 15.6% vs 13.3%; HR, 1.373; 95% CI, 0.72-2.63; P = .34) (Table 2, Figure 2B).Table 2. Five-year outcomes before and after propensity score matching.OutcomeBefore PSMAfter PSMTAVR (n = 785)SAVR (n = 148)HR95% CIP valueTAVR (n = 128)SAVR (n = 128)HR95% CIP valueMortality24.5% (192)12.2% (18)2.6961.65-4.38.00111.7% (15)12.5% (16)1.0440.52-2.12.91Inpatient nonelective hospitalization58.5% (459)62.2% (92)1.0150.81-1.27.88956.3% (72)64.1% (82)0.9350.68-1.29.65Cerebral stroke/TIA15.5% (122)14.9% (22)1.2590.79-1.98.32015.6% (20)13.3% (17)1.3730.72-2.63.34HR, hazard ratio; PSM, propensity score matching; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement; TIA, transient ischemic attack.Figure 2Five-year outcomes after propensity score matching. (A) Five-year survival. (B) Survival free from stroke. HR, hazard ratio; TAVR, transcatheter aortic valve replacement; SAVR, surgical aortic valve replacement.
In the Cox proportional hazard regression model analysis, there was no significant association between treatment cohorts (TAVR vs SAVR) and mortality (HR, 1.517; 95% CI, 0.899-2.561; P = .118). Among clinical covariates, history of heart failure was the strongest predictor of mortality with a 2-fold increase in risk (HR, 2.028; 95% CI, 1.435-2.867; P < .001). Similarly, a history of lung cancer caused a roughly 2-fold increase in mortality risk (HR, 1.959; 95% CI, 1.277-3.008; P = .002). Advancing age was also independently associated with higher mortality, as with every additional year of age, risk increases by 2.3% (HR, 1.023 per year; 95% CI, 1.006-1.041; P = .010). Overall, after adjustment for different demographic, clinical, and treatment covariates, heart failure, lung and bronchus cancer, and age were the only independent covariates associated with a change in the risk of mortality in patients undergoing AVR (Table 3).Table 3. Cox proportional hazards model for 5-year mortality.CovariateHazard ratio95% CIP valueCohort (TAVR vs SAVR)1.5170.899-2.561.118Heart failure2.0281.435-2.867<.001Diabetes mellitus0.8960.660-1.216.482Age1.0231.006-1.041.010Peripheral vascular disease0.8680.591-1.275.471Breast cancer0.8690.549-1.375.549Lymphoid malignancy1.1600.777-1.731.469Lung cancer1.9591.277-3.008.002LVEF 0%-30%2.0730.717-5.988.178LVEF 30%-50%1.4560.854-2.484.168LVEF >50%1.3290.966-1.829.080CKD1.0530.726-1.525.786Male sex1.4310.970-2.112.071COPD1.1650.849-1.598.345White race0.7980.522-1.220.298Hypertension1.6310.973-2.732.063Atrial fibrillation1.1380.844-1.536.397Smoking history0.8310.597-1.158.274Dyslipidemia0.9320.595-1.459.758Carotid stenosis0.8160.588-1.134.226Sleep apnea0.9520.672-1.349.782Beta blockers1.1760.802-1.725.406RAAS inhibitor0.8860.650-1.206.441Statin0.9100.620-1.333.627Aspirin1.2390.809-1.896.324Anticoagulant1.8030.918-3.542.087GFR 0-30, mL/min/1.73 m^2^1.4050.948-2.083.090GFR 30-45, mL/min/1.73 m^2^1.1030.728-1.671.645GFR 45-60, mL/min/1.73 m^2^0.8640.594-1.255.442GFR >60, mL/min/1.73 m^2^0.9800.626-1.535.930Hematocrit 0%-25%1.2360.874-1.749.230Hematocrit 25%-35%1.0350.711-1.505.859Hematocrit >35%0.6450.387-1.075.093Chronic ischemic heart disease0.8660.546-1.373.540CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction; RAAS, renin-angiotensin-aldosterone system; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement.
Discussion
To the best of our knowledge, this study is the largest study comparing long-term outcomes of isolated TAVR and SAVR among patients with prior mediastinal radiation. In this observational analysis, we demonstrated that there was no significant difference in 5-year mortality between propensity score-matched patients treated with TAVR or SAVR. Similarly, there were no differences in all-cause inpatient nonelective hospitalizations and ischemic stroke/transient ischemic attack (Central Illustration).Central IllustrationLong-term outcomes after transcatheter aortic valve replacement (TAVR) versus surgical aortic valve replacement (SAVR) in adults with severe aortic stenosis and prior mediastinal radiotherapy****. HR, hazard ratio.
Previous studies suggested that patients with a history of mediastinal radiation therapy are more likely to have severe coronary artery disease, conduction abnormalities, valvular heart disease, pulmonary disease, and peripheral arterial disease.2^,^18 In our study, TAVR patients had a higher prevalence of comorbidities compared with SAVR patients. They were older and had a higher prevalence of hypertension, diabetes, atrial fibrillation, peripheral vascular disease, chronic kidney disease, chronic ischemic heart disease, heart failure, and lung cancer. Together, these findings suggest that patients with prior mediastinal radiation present with greater complexity, and those with the highest burden of comorbidity were more likely to be referred for TAVR.
Long-term occurrence of cardiovascular adverse effects associated with cancer treatments, including radiation-related therapies, has garnered significant interest as cancer survival outcomes have improved in recent years.19 Despite the high prevalence of aortic stenosis in patients with mediastinal radiotherapy,1 there are only a limited number of studies comparing TAVR and SAVR in that patient population, particularly with a focus on long-term outcomes. Our study revealed that the mortality rates for TAVR and SAVR were comparable at 5 years. Similarly, Yazdchi et al20 conducted a nonmatched study on a smaller cohort of 69 TAVR and 117 SAVR patients with aortic stenosis associated with prior mediastinal radiotherapy. Their findings demonstrated that TAVR exhibited a similar survival to SAVR at 48 months postoperatively. Additionally, Donnellan et al21 reported in-hospital, 1-year, and 2-year survival rates of 96%, 91%, and 86% for TAVR, compared with 96%, 86%, and 80% for SAVR. These findings collectively suggest that TAVR and SAVR offer comparable long-term survival outcomes in these patient populations.
Significant valve fibrosis, calcification, and vascular calcification, commonly seen in radiation-associated aortic stenosis, may elevate the risk of embolization.22 This risk could be further amplified with TAVR due to catheter manipulation and transcatheter valve deployment, which can disrupt native valve structures. Despite these concerns, our analysis demonstrated that TAVR was not associated with a higher incidence of stroke compared with SAVR. Although previous studies have established similar rates of short-term perioperative stroke,10, 11, 12 the present study extended our knowledge by showing comparable stroke rates between TAVR and SAVR over a 5-year follow-up period in patients with prior mediastinal radiotherapy. Although the rates of stroke during follow-up in this analysis were higher than prior RCTs of TAVR vs SAVR, our cohort exclusively included patients with prior mediastinal radiation who are at higher risk of stroke compared with the general population.23^,^24
Controversy regarding readmission rates after TAVR in patients with prior mediastinal radiotherapy had been established in the previous studies; Nauffal et al12 showed that there was a comparable rate of 30-day readmission after TAVR or SAVR, and readmission rates of the TAVR group were 10.9% compared with 11.2% for the SAVR group. On the other hand, Zhang et al11 revealed that there was a higher readmission rate in the TAVR group compared with the SAVR group on 30 and 90 days (30 days: TAVR 10.9% vs SAVR 5.5%; 90 days: TAVR 30.9% vs 5.5% SAVR). That may be because the TAVR group had more elderly patients, had higher rates of atrial fibrillation, peripheral arterial disease, congestive heart failure, and chronic lung disease. In addition, our matched analysis confirmed that there was no significant discrepancy in the 5-year rate of readmission.
Due to the lack of a randomized controlled trial directly comparing TAVR and SAVR in patients with mediastinal radiation and symptomatic severe aortic stenosis, this observational comparative study, along with others,10, 11, 12^,^20 offers some insights to address this knowledge gap.
Limitations
This is a nonrandomized, observational study. Although a propensity score–based analysis was used to balance patient characteristics between the 2 groups, selection bias related to treatment assignment and residual confounding cannot be ruled out. The significant imbalance in group sizes (785 patients in the TAVR group vs only 148 in the SAVR group) raises concerns about the representativeness and the robustness of findings related to the SAVR cohort. Although matching led to equal sizes for comparison, the smaller SAVR sample may lack statistical power. Additionally, after matching, the TAVR group was younger and had fewer cases of heart failure, peripheral vascular disease, and lung cancer than it did before matching. This indicates that matching selected a lower-risk subpopulation of the TAVR population, limiting the study’s representativeness and generalizability. Data on complex anatomical features—such as bicuspid aortic valve, calcium scores, or hostile or porcelain aorta, which could complicate procedural management—are also not available in the data set. The study does not provide other relevant clinical data, such as the severity of aortic stenosis (including peak and mean gradients and aortic valve area), presence of other valvular diseases, or coexisting pulmonary hypertension. Unfortunately, given the study design, we could not comment on the outcomes of untreated patients with either TAVR or SAVR. Furthermore, patients with higher comorbidity burdens were more likely to undergo TAVR, and the use of older-generation TAVR devices during the study period may have influenced outcomes. Although the study evaluates 5-year outcomes, it lacks detailed information on the surveillance methods used and does not assess long-term complications or postprocedural quality of life. The use of TriNetX data limits adjustment for clustering, as the platform does not support multilevel modeling or generalized estimating equations, leaving potential residual confounding from site-level variation. The nature of the TriNetX database limited our ability to classify patients based on surgical risk. Nevertheless, matching was performed using variables included in the Society of Thoracic Surgeons risk score. Due to platform limitations, deaths were treated as censoring events rather than competing risks, which may underestimate the true incidence of nonfatal outcomes. Additionally, in our analysis, permanent pacemaker implantation occurred in very few patients below the minimum reportable threshold required by TriNetX. Therefore, we were unable to present these results.
Conclusion
In this multicentral observational study, we found no statistically significant differences in long-term outcomes between TAVR and SAVR in patients with prior mediastinal radiation. However, the study was likely underpowered to detect modest but clinically meaningful differences. Larger prospective studies are needed to better inform clinical decision-making in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu W.Masri A.Popovic Z.B.Long-term survival of patients with radiation heart disease undergoing cardiac surgery: a cohort study Circulation 1272013147614852356911910.1161/CIRCULATIONAHA.113.001435 · doi ↗ · pubmed ↗
- 2Donnellan E.Masri A.Johnston D.R.Longterm outcomes of patients with mediastinal radiation–associated severe aortic stenosis and subsequent surgical aortic valve replacement: a matched cohort study J Am Heart Assoc 62017 e 00539610.1161/JAHA.116.005396 PMC 552409028476874 · doi ↗ · pubmed ↗
- 3Desai M.Y.Karunakaravel K.Wu W.Pulmonary fibrosis on multidetector computed tomography and mortality in patients with radiation-associated cardiac disease undergoing cardiac surgery J Thorac Cardiovasc Surg 14822014475481.e 310.1016/j.jtcvs.2013.08.08724246549 · doi ↗ · pubmed ↗
- 4Leon M.B.Smith C.R.Mack M.J.Transcatheter or surgical aortic-valve replacement in intermediate-risk patients N Engl J Med 3742016160916202704032410.1056/NEJ Moa 1514616 · doi ↗ · pubmed ↗
- 5Leon M.B.Smith C.R.Mack M.Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery N Engl J Med 3632010159716072096124310.1056/NEJ Moa 1008232 · doi ↗ · pubmed ↗
- 6Elgendy I.Y.Mahmoud A.N.Gad M.M.Elbadawi A.Rivero F.Alfonso F.Transcatheter or surgical aortic valve replacement for low surgical risk patients: meta-analysis of randomized trials J Am Coll Cardiol Intv 1220191399140110.1016/j.jcin.2019.04.03731320035 · doi ↗ · pubmed ↗
- 7Popma J.J.Deeb G.M.Yakubov S.J.Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients N Engl J Med 38020191706171510.1056/NEJ Moa 181688530883053 · doi ↗ · pubmed ↗
- 8Reardon M.J.Van Mieghem N.M.Popma J.J.Surgical or transcatheter aortic-valve replacement in intermediate-risk patients N Engl J Med 37620171321133110.1056/NEJ Moa 170045628304219 · doi ↗ · pubmed ↗