Two-week cumulative tendon load estimated from insole sensor contact forces is associated with plantar flexor function in Achilles tendinopathy
Ke Song, Michelle P. Kwon, Andy K. Smith, Ryan T. Pohlig, Karin Grävare Silbernagel, Josh R. Baxter

TL;DR
This study shows that high-level tendon load measured by insole sensors is strongly linked to plantar flexor function in people with Achilles tendinopathy.
Contribution
The study introduces sensor-monitored high-level Achilles tendon load as a potential biomarker for real-world function in Achilles tendinopathy.
Findings
High-level tendon load strongly correlates with heel raise height and fast isokinetic moment.
Self-reported activity strongly correlates with high-level load but not overall load.
Sensor-monitored load shows stronger associations with function than overall load.
Abstract
Tendon loading dictates rehabilitation outcomes in Achilles tendinopathy but is difficult to track in the real world. In this study, we used instrumented insole sensors to monitor Achilles tendon load for two weeks in fifteen individuals with Achilles tendinopathy, who also completed assessments of their plantar flexor strength, dynamic function, and survey-based outcomes. We used insole data to estimate two types of cumulative Achilles tendon load: overall (≥ 0.3×body weight) and high-level load (≥ 3×body weight). We determined Pearson correlations between (1) overall and high-level tendon loads, (2) plantar flexor moment, power, work, (3) heel raise height, repetitions, countermovement jump height, and (4) self-reported symptoms and activity. Overall cumulative tendon load moderately correlated to isometric plantar flexor moment (r = 0.543) and weakly to isokinetic and dynamic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
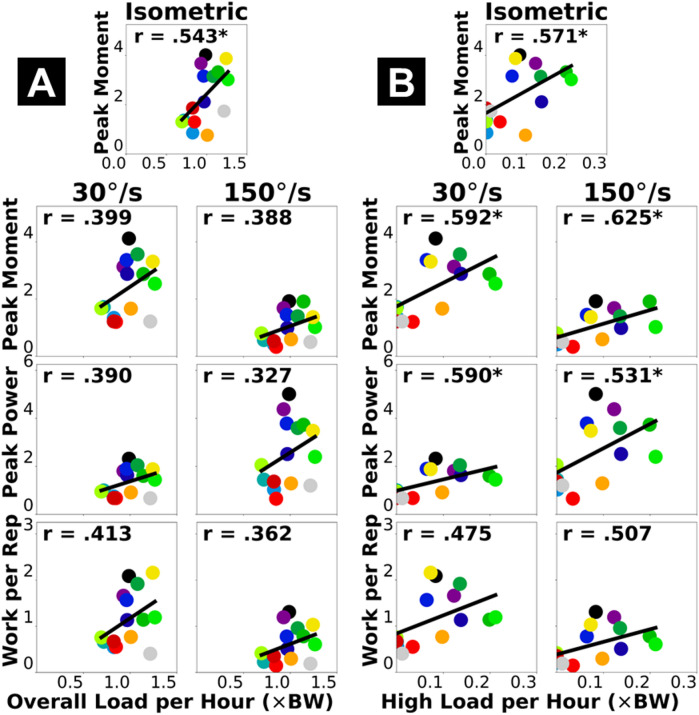 Figure 1
Figure 1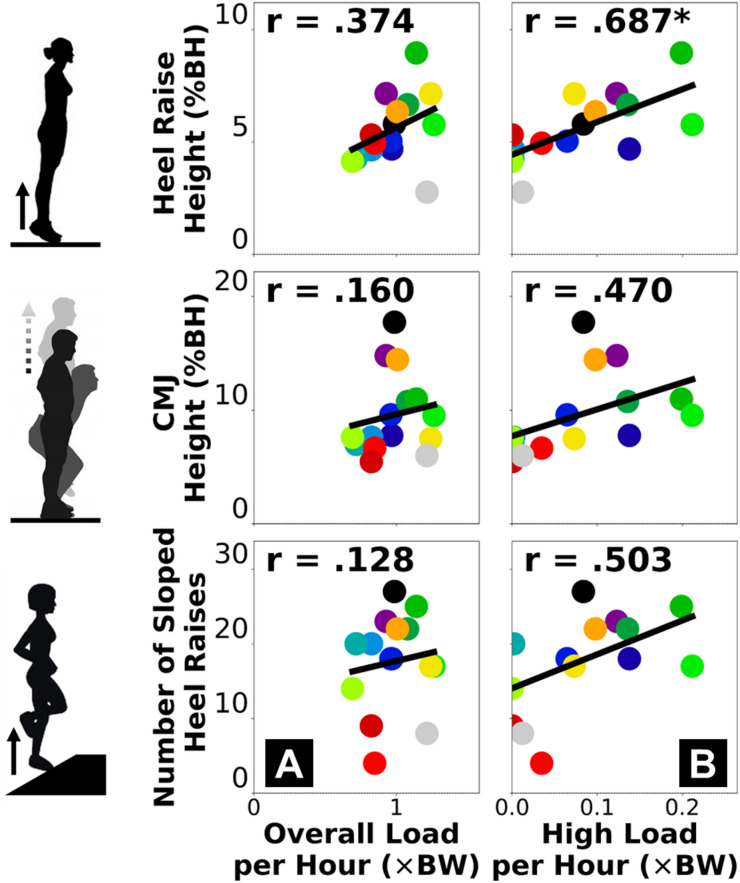 Figure 2
Figure 2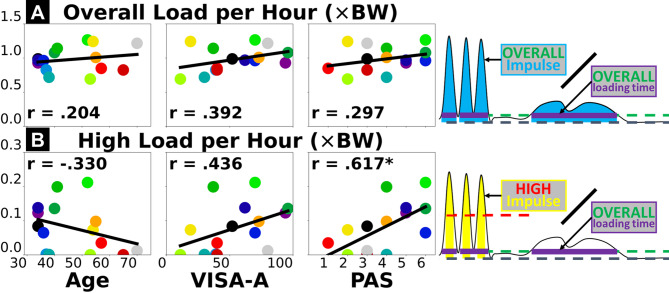 Figure 3
Figure 3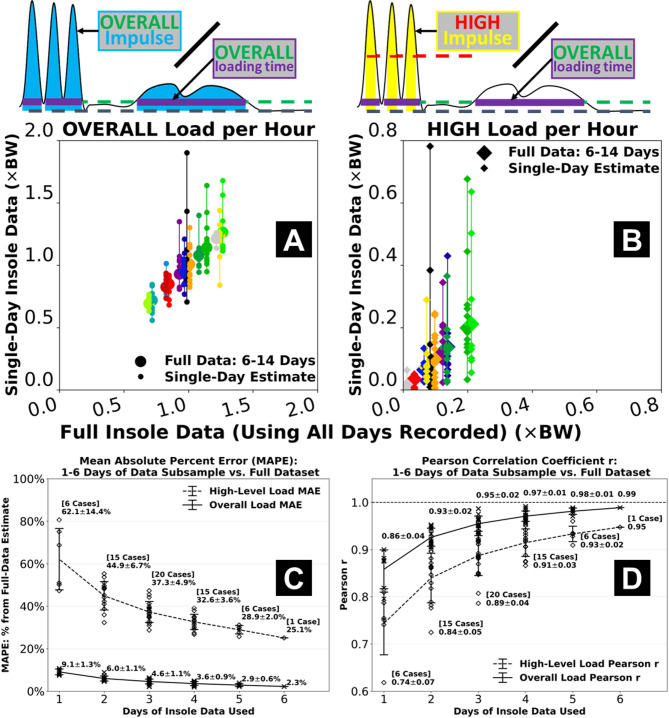 Figure 4
Figure 4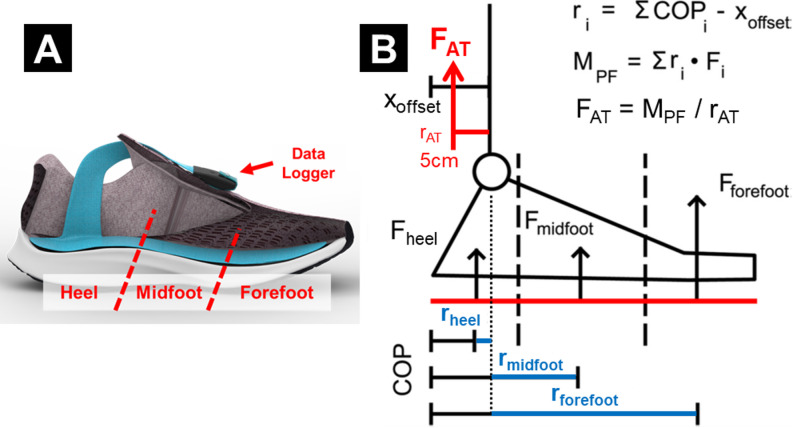 Figure 5
Figure 5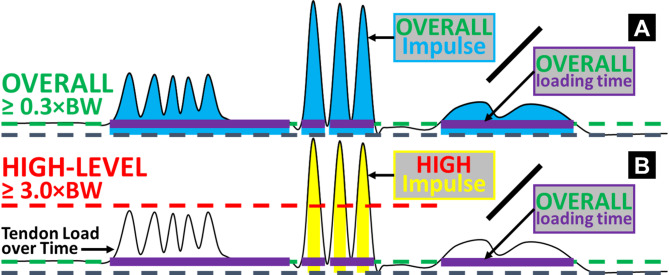 Figure 6
Figure 6- —https://doi.org/10.13039/100000002National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTendon Structure and Treatment · Shoulder Injury and Treatment · Sports injuries and prevention
Introduction
Achilles tendinopathy is a painful and debilitating chronic condition that often impacts physically active individuals^1,2^. Exercise progression to incrementally load the Achilles tendon is the clinical standard for rehabilitation and is effective in alleviating symptoms^3–7^. Progressive loading also promotes Achilles tendon tissue tolerance^7^through structural adaptations including increased stiffness^8–10^, cross-sectional area^8,9^, and reduced tendon strain^10^. However, most rehabilitation programs are designed to progress Achilles tendon load through a prescribed exercise protocol but focus less on modifying the load outside of the exercise sessions, despite the evidence that prolonged underloading and overloading are both detrimental to tendon health^11,12^. This may explain the highly variable treatment outcomes^13^where 35–60% of patients experience persistent pain^14,15^and up to 50% seek alternative treatments, including surgery^15^. Some rehabilitation programs have thought to adjust tendon load incurred during daily living based on patient-reported pain and activity level^3,5^. Yet, self-reported activities are subjective and may not fully capture the actual status of real-world tendon loading. An unmet clinical need for improving treatment efficacy is to monitor Achilles tendon load during daily living and determine how it relates to symptom severity, self-reported activity, and plantar flexor function. Especially, continuous data that track real-world Achilles tendon loading status will provide mechanistic insights into how patient symptoms and function change overtime, which can improve clinician’s ability to customize exercise progression and daily activity modification. This requires quantifying the cumulative effect of Achilles tendon load resulting from all exercises and routine activities, and their associations with clinical outcome measures. However, quantifying the real-world Achilles tendon load over a long duration remains a major technical challenge, which impedes precision rehabilitation and warrants innovation.
Wearable sensing is a rapidly evolving novel approach for quantifying real-world physical activities, movement, and metabolic parameters^16^. Sensors that measure step count, heart rate, body temperature, segment accelerations, energy expenditure, etc. are increasingly common^16–18^. Recent studies have explored using wearable motion sensors for physical activity monitoring in individuals with Achilles tendinopathy^19,20^. However, no sensor-based studies on this population have directly quantified mechanical load as a monitoring biomarker. Our group is using multiple wearable sensor paradigms to monitor Achilles tendon load in the real world^21,22^, including instrumented insoles that directly measure and track plantar contact forces^22–25^. The purpose of our current study was to use insole sensors to monitor cumulative tendon load in individuals with Achilles tendinopathy and determine how cumulative loading is associated with plantar flexor function, symptoms, and self-reported activity. We hypothesized that insole sensor-measured Achilles tendon load would be strongly correlated to plantar flexor function and self-reported activity, while moderately or weakly correlated to symptom severity.
Results
Study participant characteristics and survey measures
Among our 19 initially recruited participants, fifteen (sex: 7 males, 8 females) successfully completed their two-week insole monitoring experiment (Table 1). These 15 participants were heterogeneous in metabolic health and comorbidity statuses, as 8 of them had body-mass index > 30, 3 reported current heart conditions, 1 reported type-II diabetes, and 1 other reported peripheral neuropathy. 8 participants reported symptoms on both legs, while the other 7 reported unilateral symptoms. Achilles tendinopathy severity was highly variable on their symptomatic side (self-reported more symptomatic side if bilateral), as the Victorian Institute of Sports Assessment – Achilles (VISA-A) score ranged from 11 to 96 out of a 100-point scale. Their self-reported activity level was also highly variable, with all values (1–6) on the Physical Activity Scale (PAS) observed.
Table 1. Study participant characteristics (n = 15, sex: 7 males, 8 females) and self-reported survey measures.Age(years old)Height(m)Mass(kg)BMI(kg/m^2^)PAS(1–6 scale)VISA-A(0–100 scale)46.7 ± 12.0(34–70)1.72 ± 0.12(1.55–1.91)95.6 ± 24.9(59.0–140.6)32.9 ± 9.9(20.6–54.8)3.8 ± 1.6(1–6)54.2 ± 26.1(11–96)Data presented as mean ± 1 standard deviation (minimum – maximum values). BMI, body-mass index; PAS, Physical Activity Scale; VISA-A, Victorian Institute of Sports Assessment – Achilles questionnaire.
Cumulative Achilles tendon load: descriptive results from insole sensors
Study participants used the instrumented insole on an average of 10.1 days (standard deviation, SD: 2.2 days, range: 6–14) during their two-week monitoring period. On average, participants spent time loading their Achilles tendon above the overall level for a total of 24.1 h (SD: 14.3 h, range: 10.1–61.6) and accumulated 24.2×Body Weight (BW)×hour of overall Achilles tendon load (SD: 15.7×BW×hour, range: 8.1–62.1). As a subset of this overall load, participants spent time loading their Achilles tendon above the high-level threshold for a total of 0.6 h (SD: 0.7 h, range: 0–2.4) and accumulated 2.3×BW×hour of high-level tendon load (SD: 2.8×BW×hour, range: 0–9.3). These non-normalized cumulative hours and loading impulses are dependent on the total insole wear time by each participant. When divided by the total loading time with the insole (i.e., hours spent above 0.3×BW), participants accumulated 0.98×BW of normalized Achilles tendon load per hour above the overall level (SD: 0.18×BW, range: 0.69–1.27) and 0.08×BW per hour beyond the high level (SD: 0.07×BW, range: 0–0.21).
Fig. 1. Pearson correlations between dynamometer-based plantar flexor functional capacity (vertical axis) and insole-based cumulative Achilles tendon load (horizontal axis): normalized overall load per hour (A) and high-level load per hour (B). Each dot represents a participant. “*” annotates statistical significance of the correlation (p < 0.05). Thick black line represents best fit of linear regression where its goodness of fit corresponds to Pearson’s r value.
Cumulative tendon load vs. plantar flexor functional capacity (dynamometer)
Dynamometer-based measures of plantar flexor functional capacity generally had moderate correlations with the overall cumulative Achilles tendon load, and moderate-to-strong correlations with the high-level tendon load, depending on the testing condition (Fig. 1, Supplementary Fig. S1). Specifically, the overall tendon load per hour was weak-to-moderately and positively correlated to all plantar flexor moment, power, and mechanical work (Pearson r = 0.327–0.543; Fig. 1A). The high-level tendon load per hour had moderate (and relatively stronger) positive correlations to most dynamometer-based plantar flexor functional capacity (r = 0.475–0.592; Fig. 1B). The peak plantar flexor moment during fast isokinetic contraction met our a-priori criteria for a strong correlation (r = 0.625; Fig. 1B, top right).
Cumulative tendon load vs. plantar flexor dynamic function (motion capture)
Motion capture-based measures of plantar flexor dynamic function had weak correlations with the overall cumulative Achilles tendon load (Fig. 2A) and moderate-to-strong correlations with the high-level tendon load (Fig. 2B). Across the three exercises, double-leg heel raise height had the strongest correlations with both insole-based cumulative tendon load measures (Fig. 2, top row), with a strong correlation to the high-level tendon load per hour (r = 0.687). None of the participants completed 30 repetitions of single-leg heel raises on the inclined slope (range: 4–27), and this repetition count did not strongly correlate to the cumulative Achilles tendon loads (Fig. 2, bottom row).
Fig. 2. Pearson correlations between motion capture-based plantar flexor dynamic function (vertical axis) and insole-based cumulative Achilles tendon load (horizontal axis): normalized overall load per hour (A) and high-level load per hour (B). Each dot represents a participant. “*” annotates statistical significance of the correlation (p < 0.05). Thick black line represents best fit of linear regression where its goodness of fit corresponds to Pearson’s r value.
Cumulative tendon load vs. self-reported clinical measures (surveys)
Overall cumulative Achilles tendon load per hour had weak positive correlations with all three self-reported survey measures: age (r = 0.204), severity of Achilles tendinopathy by the VISA-A score (r = 0.392), and current activity level by the PAS score (r = 0.297) (Fig. 3A). Cumulative high-level Achilles tendon load per hour had a weak negative correlation to participant age (r = -0.330), moderate positive correlation to the VISA-A score (r = 0.436), and strong positive correlation to the PAS score (r = 0.617) (Fig. 3B).
Fig. 3. Pearson correlations between insole-based cumulative Achilles tendon load (vertical axis) and survey-based measures of participant characteristics or outcomes (horizontal axis). Insole-based measures include normalized overall load per hour (A) and high-level load per hour (B). Survey-based measures include age (left), severity of Achilles tendinopathy – VISA-A score (center), and self-reported current activity level – PAS score (right). Each dot represents a participant. “*” annotates statistical significance of the correlation (p < 0.05). Thick black line represents best fit of linear regression where its goodness of fit corresponds to Pearson’s r value.
Fig. 4. Effects of using a reduced number of days of insole data compared to using the full two-week dataset. Estimates from a single day of data often tended to under- or over-estimate the overall load (A) and especially the high-level Achilles tendon load per hour (B). Mean absolute percent error for 1 day-based estimate was < 10% from full dataset-based for the overall load, but > 60% for the high-level load which also showed more day-to-day variations (C). Using more days of data gradually reduced error and increased its correlations to the full dataset. When using the first 6 days of data, mean absolute percent error of the high-level load was 25.1% and correlation was r = 0.95 against the full dataset-based estimate (D). Error bars represent ± 1 standard deviation from the mean across all 1, 2, …, or 6 day-based estimates.
Effects of insole data subsampling
Using reduced days of insole data led to increased error in estimated overall cumulative and high-level tendon loads, as their agreement with the full data-based estimates decreased (Fig. 4, Supplementary Table S1, Supplementary Fig. S2, Supplementary Fig. S3). Estimates of the overall tendon load were relatively robust with subsampling, as the mean absolute percent error remained < 10% even when only using 1 day of insole data (Fig. 4A and C). In contrast, using 1 day of data led to misestimated high-level load per hour for some participants on multiple days, resulting in a > 60% mean absolute percent error across the group (Fig. 4B and C). This error was gradually reduced when increasing the insole sensor monitoring days. When using the first 6 days of data from each participant, mean absolute percent error of the high-level tendon load was 25.1% (Fig. 4C) with correlation r = 0.95 against the full dataset-based estimate (Fig. 4D). Additionally, repeatability of overall load estimation was excellent for 3 + days of data (intraclass correlation ICC ≥ 0.92) and moderate among 1-day subsamples (ICC = 0.69), while repeatability of high-level load was poor among 1-day subsamples (ICC = 0.49) and needed 5 + days to be excellent (Supplementary Table S2).
Discussion
The purpose of this study was to use insole sensors to monitor cumulative tendon load in individuals with Achilles tendinopathy and determine how cumulative loading is associated with plantar flexor function, symptoms, and self-reported activity. We found that 6–14 days of Achilles tendon load monitored by the force-sensing insole, especially cumulative high tendon load beyond the level of walking, is moderate-to-strongly correlated to plantar flexor function. Consistent with our hypothesis, sensor-based tendon load estimates demonstrated stronger correlations to plantar flexor function yet weaker correlations to survey-based measures like symptoms and age. Cumulative high-level tendon load is strongly correlated to self-reported activity, which also supports our hypothesis. However, while self-reported activity is generally in agreement with objectively measured tendon load, they do not capture the same biomechanical information. Our new findings support the clinical value and advantage of using wearable sensors to monitor Achilles tendon load in daily living, for quantifying the real-world plantar flexor function in individuals diagnosed with Achilles tendinopathy.
Stronger associations with the high-level Achilles tendon load than the overall tendon load suggest that clinical function assessments for Achilles tendinopathy provide insight into the real-world performance of high loading activities. Cumulative high tendon load beyond the level of walking showed strong associations with both the functional capacity (Fig. 1B) and dynamic function (Fig. 2B) of the plantar flexors. These associations reached our criteria of strong (r ≥ 0.6)^26,27^for peak moment during fast isokinetic contraction (our most dynamic strength testing condition) and double-leg heel raise height. This indicates plantar flexor weakness for performing dynamic movements likely limits high-level tendon loading in the real world. Considering recent clinical findings that functional goals and recovery trajectories vary among patients with Achilles tendinopathy^28,29^, for those who wish to return to sports or plyometric exercises, achieving a good level of cumulative high tendon load in daily living may be a useful clinical goal. Conversely, performing high loading activities regularly may protect patients against plantar flexor functional loss. Patients who have maintained a high tendon load level are unlikely to be impaired by weakness, and they may instead benefit from tendon load management through daily activity modifications for reducing symptoms. As opposed to the high-level load, the overall cumulative tendon load did not strongly associate with plantar flexor function (Figs. 1A and 2A). Isometric moment was the only functional measure moderately correlated to overall tendon load (r = 0.543), while all isokinetic and dynamic measures had weaker correlations (r ≤ 0.413). This means overall tendon loading in daily life at most partially reflects isometric muscle strength but cannot explain plantar flexor dynamic functionality, which indicates a potential disconnect between tendon health status and the real-world overall loading. For example, some (but not all) patients may expose their Achilles tendon to detrimental overloading or underloading in daily living that mismatches their functional recovery progress^11,12^, which could contribute to suboptimal recovery and thus explain the greatly varied treatment outcomes among patients that clinicians observed^13–15^.
Survey-based measures also had stronger associations with the high-level Achilles tendon load compared to the overall tendon load. The correlations between overall tendon load and age, symptoms, and self-reported activity were all weak (Fig. 3A), indicating that overall tendon load attributed to general daily living activities is neither fully explained by older age or a more sedentary lifestyle, nor adequately explains worse symptoms. A possible reason is that walking is the most common daily movement for most individuals, yet those who are of older age or self-perceive as physically inactive do not necessarily walk less. Age was negatively correlated to the high-level tendon load (r = -0.330, Fig. 3B) likely due to older individuals engaging in fewer dynamic activities, but this weak association is insufficient to confirm age as a reliable biomarker for reduced high-level Achilles tendon load either. Finally, weak-to-moderate associations with the VISA-A score indicate that symptoms like pain may not fully explain how Achilles tendon loading status changes in daily living (or vice versa). Confirming the cause-effect relationship between symptoms and tendon loading is beyond the scope of this cross-sectional study and warrants future longitudinal research.
Self-reported activity and standard heel raises both represented high-level tendon load well, yet they did not always suggest plantar flexor functional deficit. For our study participants, the cumulative high-level Achilles tendon load was strongly correlated to self-reported current activity level (Fig. 3B) and the double-leg heel raise height (Fig. 2B). Comparing across exercises, we found real-world tendon loading to be better associated with double-leg heel raise height compared to countermovement jump height and inclined single-leg heel raise repetitions (Fig. 2). This may be partly due to more variable techniques adapted by our heterogeneous group of study participants (Table 1) to perform more dynamic and demanding tasks like jumping. The double-leg heel raises are easier to perform and standardize, which may explain the consistent relationship to real-world tendon loading status in a heterogeneous patient population. Generally, our data supports the clinical usefulness of patient-reported activity surveys for informing exercise progression, and standard heel raises as a reliable rehabilitation exercise to improve planter flexor function^3–7^. However, they only marginally exceeded our criteria for strong correlation (r = 0.617–0.687) and do not fully explain real-world tendon loading. Despite being easier to implement than wearable sensors, a shortcoming of survey-based activity monitoring is that the discrete response options may be interpreted differently across individuals, inducing subjectivity and impeding specificity. For example, 3 of our participants responded the highest activity level (PAS = 6), but their cumulative high-level tendon load was either below, at, or above the group-wise trend in a divergent manner (Fig. 3B, bottom right). In a supplementary analysis, we found that the plantar flexor functional measures had weaker correlations to the PAS score (r = 0.227–0.491, Supplementary Fig. S4 & S5) than to insole-based high-level load (r = 0.470–0.687, Figs. 1B and 2B). This finding indicates that self-reported activity in Achilles tendinopathy patients may mismatch whether they have fully regained plantar flexor function. Insole-monitored cumulative Achilles tendon load provides new objective information on the multi-day loading status of the plantar flexors, therefore shows promise as a useful new biomarker for real-world function in physically active individuals. Knowing the continuous tendon loading status will inform clinicians to refine strategies that better mitigate the real-world impact of loading on Achilles tendinopathy.
To our knowledge, this study is the first to monitor foot contact force and estimate Achilles tendon load over a weeks-long duration. We chose a two-week paradigm to capture as much real-world insole data as we could and explore their “best scenario” associations with clinical measures. This allowed us to evaluate whether insole-based tendon load monitoring is clinically meaningful and worthy of future development. Although the associations with plantar flexor function suggest insole-based measures have promising clinical value, securing the multi-day insole data had been a challenging process for both our study participants and our research team. Practical constraints included but were not limited to shoe type, preference about wearing shoes at home, and concerns about the insole sensor appearance. These constraints all limited our participants’ ability to wear the insole and contributed to the varied actual days (6–14) and hours each day they logged data. In our subsampling analysis, we found that when only using 1 day of insole data, error against the full dataset remained low for the overall tendon load estimate (< 10%) but was higher for the high-level load (> 60%) (Fig. 4C). One day of insole sensor data may thus be sufficient to reliably characterize habitual tendon loading required for daily living mobility. Instead, multi-day insole monitoring may be necessary to ascertain the high-level tendon loading status, including its day-to-day variations, that are unique to sports and dynamic activity. We expect the challenges we experienced to impact most studies that implement day(s)-long insole sensor monitoring. We thus recommend researchers to carefully choose insole monitoring durations based on the population studied and standardize monitoring protocols. These considerations will help researchers expand cohort size and discover clinically relevant loading parameters with a higher level of confidence.
Beyond monitoring duration, researchers should also be aware of several other technical and practical challenges before using instrumented insoles for real-world monitoring in scale. For example, technical factors like data storage capacity and the need to rechange sensors may limit the monitoring duration and add to data inconsistency. Another standing challenge is the technical drawbacks of the instrumented insoles, such as signal noise, nonphysical artifacts, and device malfunctions vulnerable to insole misfit or miscalibration (Supplementary Fig. S7 & S8). Future development work should mitigate these limitations by improving sensor storage capacity, battery life, and technical robustness. Combined with wear time variability, we had to assume that the total loading time with the insole that we captured were representative of wearers’ typical activity and Achilles tendon loading status. If a study participant would only wear the insole whenever they exercise, we would overestimate their cumulative tendon load per hour on those days (Fig. 4). Conversely, if the insole monitoring day for a runner coincided with their resting day of the week, we would underestimate their habitual high-level tendon load. We urge our fellow researchers to continue exploring better strategies to reduce participant burden and improve study protocol adherence, for capturing more consistent and more representative insole data. Researchers should also explore the utility of other wearable sensors that have established good feasibility for continuous monitoring, including inertial measurement units^16,19–21^, and identify how sensor-based measures of motion (body acceleration, velocity, position, orientation, etc.) associate with relevant mechanical biomarkers (e.g., Achilles tendon load) and clinical outcome measures.
Our findings should be considered with several limitations. First, while dividing by the total loading time partly addressed the variability in wear time and study protocol adherence, our normalized measures of cumulative loading may be difficult to contextualize or implement as a clinical measure. We elaborated our considerations and recommendations for future work in the previous paragraphs. Second, because the 0.3×BW baseline cutoff removed all transient unloaded periods including the swing phases of walking and running, our definition of the total loading time does not readily represent full active time of the insole wearer. Past studies have developed epoch-based algorithms to determine total active time wearing motion sensors^30^, which can be adapted for evaluating insole sensor wear time and adherence to the monitoring protocol. Third, we made a simplifying assumption that Achilles tendon is the primary force contributor to plantar flexor moment. Omitting small plantar flexor muscles could lead to slight overestimation of the Achilles tendon load. However, triceps surae account for > 75% of plantar flexor muscle forces^31^while moment arm of the Achilles tendon is more than double of all other plantar flexors^32^. In combination, we approximate Achilles tendon load to account for at least 85–90% of the plantar flexor moment. Fourth, we assumed a standardized 5 cm Achilles tendon moment arm^33^for algorithm simplicity. Individual differences in tendon moment arm could influence the tendon load estimate, especially on our participants of heterogeneous body size (Table 1). However, prior studies found Achilles tendon moment arm to vary < 10% across individuals^32^and suggested it does not substantially alter Achilles load estimation versus detailed musculoskeletal models^33^. Fifth, we did not record pain during or after the in-lab functional assessments. In the recent clinician consensus^34^, two of the core outcome measures for Achilles tendinopathy are pain during and after functional activities, which should be included in future studies. Sixth, the interaction between mechanical loading and tendon structure in Achilles tendinopathy is clinically recognized^3,7–10,28,29^, but the relationships between plantar flexor muscle-tendon structure and cumulative Achilles tendon load remain unknown. Our ultrasound-based studies to investigate this question are ongoing.
Another important limitation was our small sample size mainly owing to the technical and practical challenges with insole monitoring. This had limited our ability to stratify patients based on pain bilaterality, severity, body size, comorbidities, psychosocial statuses, or our new insole-based measures. These factors were heterogeneous across our participants (Table 1) and could influence both real-world tendon loading and clinical outcomes. However, because our goal was to determine associations between loading and clinical outcomes, rather than their cause-effect relationships or the relative importance between loading and patient intrinsic factors, we do not consider these factors to induce bias in testing our hypothesis. Recent clinical studies have identified homogeneous subgroups within Achilles tendinopathy patients who likely need distinctive intervention strategies^28,29^. The stronger associations we observed in high-level tendon load indicate that cumulative Achilles tendon load may be of higher importance to the activity-dominant patient subgroup^28,29^, but this requires confirmation in a larger cohort. Our larger study is enrolling more patients for insole monitoring, which will enable stratified subgroup analyses to gain deeper insights. The current study takes a groundbreaking step by providing a first-of-kind biomechanical dataset that confirmed the clinical value and advantage of real-world wearable sensor monitoring. Our findings will serve as valuable guidance to better implement larger future studies.
In conclusion, cumulative Achilles tendon load monitored by instrumented insole through 6–14 days is moderate-to-strongly associated with plantar flexor function in individuals with Achilles tendinopathy. Stronger associations with the high-level Achilles tendon load than the overall load suggest that clinical function assessments for Achilles tendinopathy provide insight into the real-world performance of high loading activities. In contrast, the disconnect between overall tendon loading and plantar flexor function may explain the variability in recovery outcomes. Self-reported activity and standard heel raises represent high-level tendon load well, yet they do not always suggest plantar flexor functional deficit. Sensor-monitored Achilles tendon load shows promise as a useful new biomarker for real-world plantar flexor function in physically active individuals. Considering the associations between cumulative tendon loads and clinical measures, yet the standing challenges with using insole sensors, we advocate for further research and development to improve the practicality of insole monitoring paradigms and upscale analyses on real-world data. This will lead to a better understanding on the roles of tendon loading in real-world functional performance in individuals with Achilles tendinopathy.
Methods
Study participants
We recruited 19 adults with clinically confirmed diagnosis of Achilles tendinopathy from the University of Pennsylvania orthopaedic clinic and our local community. A recent study^35^found significant correlations between lower limb function (drop jump height) and Achilles tendon load in the lab based on 19 individuals with Achilles tendinopathy, which matched our enrollment size. Our eligibility criteria were between 18 and 70 years of age, no prior Achilles tendon rupture, no other musculoskeletal injuries in the past six months, no use of nicotine or steroid medication, and not pregnant. A board-certified physical therapist (A.K.S.) confirmed the diagnosis of either midportion or insertional Achilles tendinopathy using medical records, tendon tenderness upon palpation, and positive Arc sign and Royal London Hospital tests^36^. Our study was approved by the Institutional Review Board at the University of Pennsylvania (IRB Protocol #850424) and all participants provided written informed consent before starting the experiments. We performed all research activities in this study in accordance with the Declaration of Helsinki and relevant human participant research regulations and guidelines.
In-lab experiments: self-reported outcomes and plantar flexor function
Participants completed digital questionnaires in the REDCap database system (version 13, REDCap Project, Nashville, TN)^37,38^. These questionnaires surveyed participant age, sex, body height and mass, and the symptomatic side (self-reported more symptomatic side if bilateral). Participants reported the severity of their Achilles tendinopathy specific to the (more) symptomatic tendon using the 8-item Victorian Institute of Sports Assessment – Achilles (VISA-A) questionnaire^39^, which is scored 0–100 with 100 indicating no symptom or disability. Participants also reported their perceived current physical activity level using the clinically validated Physical Activity Scale (PAS)^3,40^, a single question scored 1–6 with 6 indicating regular intensive exercises several times a week and 1 indicating hardly any physical activity.
We assessed two types of plantar flexor function: capacity and dynamic function. We first quantified functional capacity of the plantar flexors via isometric and isokinetic strength testing. Participants were positioned lying prone on a treatment plinth adjacent to an isokinetic dynamometer (VAC System 4 Pro, Biodex Medical Systems, Shirley, NY) with knees extended straight, following our published experimental protocol^41^. Each participant performed three maximal voluntary contraction trials on their (more) symptomatic side, with three repetitions each: (1) isometric at neutral ankle position, (2) slow isokinetic (30°/s), and (3) fast isokinetic (150°/s). We quantified 7 measures of plantar flexor functional capacity, each normalized by body height times weight: peak moment during all 3 contraction types (unit: %H×W); peak power during slow and fast isokinetic contractions, by moment times plantarflexion speed (unit: %H×W×rad/s); mechanical work per slow and fast isokinetic contraction, by the integral of power over time (unit: %H×W×rad). We averaged each functional capacity measure across the 3 contraction repetitions.
We next quantified plantar flexor dynamic function using motion capture. Each participant performed three exercises commonly used in Achilles tendinopathy clinical assessment or treatment^3–7,35^in the following order: 10 double-leg heel raises, 5 single-leg countermovement jumps, then consecutive single-leg heel raises on a 25° inclined slope until 30 repetitions or self-determined physical exhaustion when they were allowed to stop voluntarily. We allowed participants to perform each exercise at self-selected pace to assess the habitual status of their dynamic muscle function. We recorded videos of each exercise using 8 synchronized high-resolution cameras (2.1-megapixel Optitrack Prime Color, NaturalPoint Inc., Corvallis, OR), from which we quantified the shank and foot positions using a markerless motion tracking algorithm (Theia3D v2023.1.0.3160, Theia Markerless Inc., Kingston, ON, Canada)^42,43^. We calculated three clinically relevant kinematic measures of the plantar flexor dynamic function on the (more) symptomatic side^3–7,35^: double-leg heel raise height, single-leg countermovement jump height, and total repetitions of single-leg heel raises on the 25° slope. We normalized heel raise height and countermovement jump height by body height (unit: %BH) to account for participant body size differences^44–46^, then averaged them across movement repetitions.
At-home experiment: instrumented insole monitoring of Achilles tendon load
We used an instrumented force-sensing insole (Loadsol Pro 2 HMF, Novel GmbH, Munich, Germany) to monitor Achilles tendon load for up to two weeks. Each insole has 3 plantar force sensor pads (heel, midfoot, forefoot) embedded within its flexible surface. They are wire-connected to a miniature data logger that can be mounted on shoelaces and continuously log plantar contact forces with a battery life of ~ 25 h (Fig. 5A). These instrumented insoles use a smartphone application to begin and stop data acquisition and store them on the data logger.
Fig. 5. Instrumented insole for Achilles tendon load monitoring. (A) Insole device embedded with 3 plantar force sensors, shown here fit into a typical athletic shoe. (This diagram is created with copyright permission from Novel GmbH.) (B) Our validated algorithm to estimate Achilles tendon load from the 3 sensor forces. We assumed each force to be perpendicular to the sole and applied at constant center of pressure (COP). We measured the moment arms of each force (r_i_) relative to the ankle joint, computed plantarflexion moment (M_PF_) by the sum of 3 force-by-moment arm products, then estimated Achilles tendon load (F_AT_) by dividing the moment by an assumed tendon moment arm (r_AT_ = 5 cm).
We fit one insole into each participant’s own shoe under the (more) symptomatic foot. We trained participants to initialize the insole each morning, by setting the sensor force to zero when standing on the opposite foot, with a provided controller smartphone for data collection over the following two weeks. We asked participants to wear the insole as much as possible throughout the day and recharge the sensors overnight with a provided cable. We also asked participants to move the insole into any shoe they change into (unless it is infeasible) and re-initialize immediately after shoe change. This means there may be one or multiple data recordings per day of insole wearing, depending on the shoe changes. Over the two-week span, we sent daily text messages to their smartphone reminding them of their insole monitoring experiment. We provided a prepaid return mailing box, which the participants used to mail the instrumented insole back to us at the end of the two-week period. All sensor recordings were logged at 20 Hz and transferred from the data logger to our database via the smartphone. A recent study found that sampling insole sensor data at 20 Hz only induces < 3% error in peak plantar force compared to 100 Hz, while increasing real-world data capturing capacity by five times^47^.
Cumulative Achilles tendon load Estimation
The data quality of each insole recording was numerically and graphically verified before downstream processing. Specifically, we ensured that sensor force stayed zero whenever unloaded by detecting and removing nonphysical baseline signal drifts (Supplementary Fig. S7). We also screened for and removed erroneous recordings possibly caused by incorrect sensor initialization or insole misfit in the shoe (Supplementary Fig. S8 & Supplementary Table S3). This verification process was necessary for removing nonphysical artifacts that would cause incorrect estimation of the Achilles tendon load. Notably, we had to exclude 3 of our 19 initially recruited participants from data analysis because most of their recordings were erroneous. We additionally excluded 1 participant who did not follow our full-day insole monitoring protocol (and instead recorded only 1–3 h each day), leaving data from 15 participants remaining for analysis.
Achilles tendon load was estimated from sensor-measured plantar contact forces using our validated physics-based algorithm^23^. Briefly, we computed the net moment of plantar force using the 3 insole sensor forces and the size-specific dimensions of each sensor relative to the ankle joint (Fig. 5B). Our published study^23^showed that this simple algorithm estimates ankle moment with strong agreement (> 96.4%) against standard in-lab motion capture. We divided this plantarflexion moment by a 5 cm tendon moment arm^33^for a proxy estimate of the Achilles tendon load. This approach assumed that Achilles tendon is the primary force contributor to plantar flexor moment^31,32^, and its < 10% moment arm variation from the ~5 cm average^32^does not substantially affect tendon load estimation^33^. We normalized this estimated Achilles tendon load by body weight (unit: ×BW) to compare across study participants.
We developed two new measures to quantify the cumulative effect of insole-based Achilles tendon load: the overall load and the high-level load (Fig. 6). First, we selected two loading magnitude thresholds to delineate a general overall level and a representative high level of tendon loading, according to our published database on Achilles tendon load during exercises^7^. Specifically, we defined 0.3 times bodyweight (0.3×BW) as the overall tendon loading threshold (Fig. 6A), because this is the load experienced during the lowest-loading Achilles tendon exercise: seated heel raises^7^. The 0.3×BW threshold thus represents a clinically meaningful baseline tendon load. We defined time above 0.3×BW as each participant’s total loading time with the insole, which excluded all periods of inactivity, insole non-wear, and sensor noises below the baseline (Supplementary Fig. S9). Similarly, we defined 3 times bodyweight (3.0×BW) as the high-level tendon loading threshold (Fig. 6B), because this is approximately the peak Achilles tendon load during walking^7,48^. The 3.0×BW threshold represents a boundary beyond daily living mobility tasks – which is primarily walking – such that cumulative loading above this level results predominantly from dynamic exercises and thus is uniquely relevant to physically active individuals. We then summed magnitude-stratified tendon load impulses across the entire monitoring duration (all days combined) using numerical integration (unit: ×BW×hour): cumulative overall tendon load equals all impulses whenever loading exceeded 0.3×BW combined, and cumulative high-level load equals all impulses whenever loading exceeded 3.0×BW combined. These cumulative loads represent the combined effect of loading magnitude and frequency. Because loading above 3.0×BW is always also above 0.3×BW, the high-level cumulative tendon load is a subset of the overall load.
Fig. 6. Diagrams illustrating the definitions of the two cumulative Achilles tendon loads, above overall and high-level thresholds. The waveform in each diagram exemplifies insole-based Achilles tendon load (vertical axis) as a function of time (horizontal axis). (A) We defined an overall threshold of 0.3×BW to represent loading incurred from any daily living activity that loads the Achilles tendon. This excluded inactivity periods and whenever the sensor was recording but not worn (e.g., right end of the diagram). We defined overall cumulative time above 0.3×BW (purple bars) as the total loading time with the insole. We summed impulses when loading was above this overall level (blue areas) and divided it by the total loading time for the overall tendon load accumulated per hour. (B) Similarly, we defined a high-level threshold of 3.0×BW to quantify loading incurred beyond walking and thus primarily resulted from dynamic physical activities. We summed impulses when loading was above this high level (yellow areas) and divided it by the total loading time (not high-level cumulative time) for the high-level tendon load accumulated per hour.
These two measures of the cumulative overall and high-level tendon load were not readily proportional to the full amounts of real-world loading, because they were still dependent on insole wear time. Namely, the total time a study participant is able or willing to wear the insole does not exactly correspond to the time when that individual is physically active and loading their Achilles tendon. Practical considerations like the type of shoes worn, preference about at-home wearing, bedtime variability, and concerns about aesthetics are some reasons participants may have chosen not to wear the insole during parts of the two-week period. To account for these sources of variability, we divided the cumulative overall and high-level loads by the total time spent above the overall load level, i.e., participant’s total loading time with the insole, all days combined (Fig. 6). This yielded the normalized overall and high-level loads accumulated per hour (unit: ×BW). We used these two normalized measures of cumulative Achilles tendon loading on each of the 15 participants for statistical analysis.
Statistical analysis
We computed Pearson correlations between insole-based cumulative Achilles tendon loads (overall and high-level) with dynamometer-based plantar flexor functional capacity, motion capture-based dynamic function, and survey-based clinical outcome measures (Table 2; n = 15 for each correlation test). We tested two measures of insole-based cumulative Achilles tendon load: (1) normalized overall load per hour and (2) normalized high-level load per hour. We tested seven measures of plantar flexor functional capacity: (1–3) peak moment during isometric, slow (30°/s) isokinetic, fast (150°/s) isokinetic contractions, (4–5) peak power during slow and fast isokinetic contractions, (6–7) mechanical work per slow and fast isokinetic contraction. We tested three measures of plantar flexor dynamic function: (1) double-leg heel raise height on the (more) symptomatic side, (2) single-leg countermovement jump height, (3) repetitions of single-leg heel raises on the inclined slope. We tested three survey-based measures: (1) age, (2) VISA-A score on the (more) symptomatic side, (3) current Physical Activity Scale. We defined the strengths of Pearson correlation according to literature^26,27^: |r| ≥ 0.6 as strong, 0.4–0.6 as moderate, and < 0.4 as weak. We additionally determined whether the correlation strength is statistically significant (α = 0.05) only as an ancillary metric, as we consider the descriptive strengths of correlations (weak, moderate, or strong) as our primary statistical results.
Table 2. Measurement categories for statistical analysis (technique used), the specific measures tested, and their units.CategoryMeasuresUnit Achilles tendon
cumulative loading
( Insole sensors ) (1) Overall tendon load (≥ 0.3×BW) normalized per hour ×BW(2) High-level tendon load (≥ 3.0×BW) normalized per hour
Plantar flexor
functional capacity
( Dynamometer testing ) (1–3) Peak plantar flexor moment(isometric, 30°/s, 150°/s)%H×W(4–5) Peak plantar flexor power(30°/s, 150°/s)%H×W×rad/s(6–7) Mechanical work per contraction(30°/s, 150°/s)%H×W×rad Plantar flexor
dynamic function
( Motion capture ) (1) Double-leg heel raise height(more symptomatic side)%BH(2) Single-leg countermovement jump height(3) Single-leg heel raise repetitions on 25° slope– Self-reported outcomes
and characteristics
( Survey questionnaires ) (1) AgeYears(2) VISA-A score (more symptomatic side)–(3) PAS score (current level)–×, times; BW/W, Body Weight; BH/H, Body Height; °, degree; s, second; rad, radius; VISA-A, Victorian Institute of Sports Assessment – Achilles questionnaire; PAS, Physical Activity Scale.
Insole data subsampling analysis
We performed an ancillary analysis to determine the minimal amount of insole data needed to reliably represent habitual two-week Achilles tendon loading. This analysis is important due to the practical challenges regarding using insole sensors, and useful for establishing best practices that future studies can leverage to balance data fidelity with participant burden. We iteratively quantified the difference between our full two-week insole dataset and extracted data subsamples with a reduced number of monitoring days. Specifically, using overall and high-level cumulative tendon loads estimated from the full two-week dataset as reference, we computed the mean absolute percent error (percent difference from full dataset-based)^21,49,50^and Pearson correlations when estimating from gradually reduced days of insole data: 6 (the first six days recorded by each participant), 5 (omit day-1, …, omit day-6), 4, 3, 2, or 1 day (day-1 only, … day-6 only). We also tested the repeatability of estimating overall and high-level loads within a specific subsample size choice, by intraclass correlations (ICC)^51^among estimates from all single days or all multi-day combinations. We chose to use these descriptive statistics rather than inferential testing, because our goal was to describe the agreement between insole monitoring strategies and not to draw inferences on how day-to-day variations affect cumulative loading. We hypothesized that cumulative tendon loads based on 6-day insole data would remain close to full dataset-based estimates, whereas using 1 day of data would lead to larger differences.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Campbell, M. J. Correlation and Regression. in Statistics at Square One (ed. Campbell, M. J.) 169 (John Wiley & Sons, Inc., Hoboken, NJ, USA, 2012).
- 2Evans, J. D. Straightforward Statistics for the Behavioral Sciences (Brooks/Cole Publishing Co., 1996).
- 3Hullfish, T. J., O’Connor, K. M. & Baxter, J. R. Medial gastrocnemius muscle remodeling correlates with reduced plantarflexor kinetics 14 weeks following Achilles tendon rupture. J. Appl. Physiol. (1985) 127, 1005–1011. 10.1152/japplphysiol.00255.2019 (2019).10.1152/japplphysiol.00255.201931589091 · doi ↗ · pubmed ↗