Dietary patterns and associated factors among type 2 diabetes mellitus patients attending Wolaita Sodo university comprehensive specialized hospitals, South Ethiopia
Amanuel Kora Moliso, Haileyesus Worku Fankasho, Wondimagegn Paulos Kumma

TL;DR
This study explores the dietary habits of type 2 diabetes patients in Ethiopia and finds that occupation and health conditions influence their food choices.
Contribution
The study identifies two distinct dietary patterns among T2DM patients and links them to occupational status and comorbidities in a low-resource setting.
Findings
A mixed dietary pattern, including raw meat and soft drinks, is associated with being a daily laborer.
A traditional dietary pattern is inversely linked to the presence of comorbid conditions.
Occupational status and comorbidity burden are significant determinants of dietary behavior in T2DM patients.
Abstract
A controlled diet is essential for delaying disease progression and achieving optimal glycemic control among individuals with type 2 diabetes mellitus (T2DM); however, inappropriate dietary practices remain common in low-resource settings. This hospital-based cross-sectional study examined dietary patterns and associated factors among adults with T2DM attending Wolaita Sodo University Comprehensive Specialized Hospital, Southern Ethiopia. A total of 416 participants were selected using systematic random sampling. Data were collected using a structured questionnaire, including a one-week food frequency questionnaire, socio-demographic and lifestyle characteristics, nutrition knowledge, and fasting blood sugar measurements. Dietary patterns were identified using factor analysis, and multiple linear regression models were applied to assess associated factors. Two major dietary patterns…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
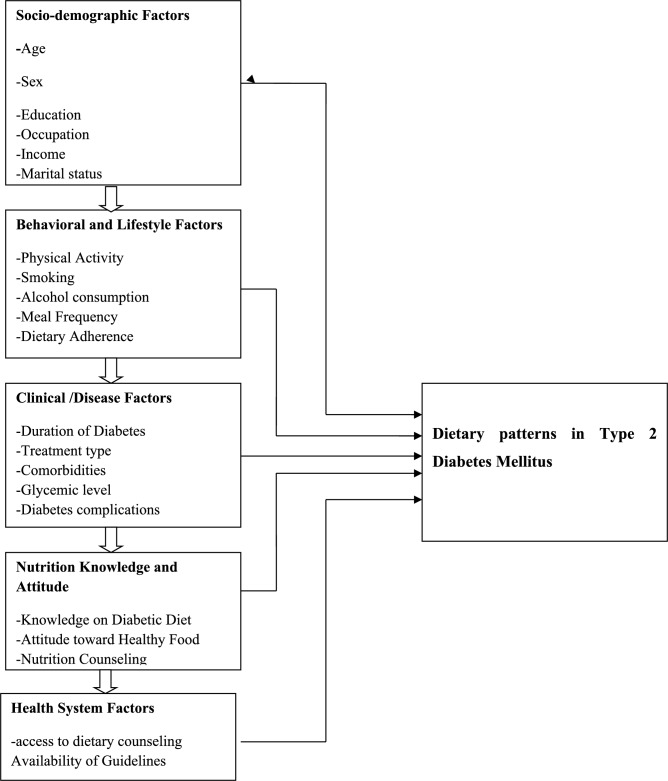 Figure 1
Figure 1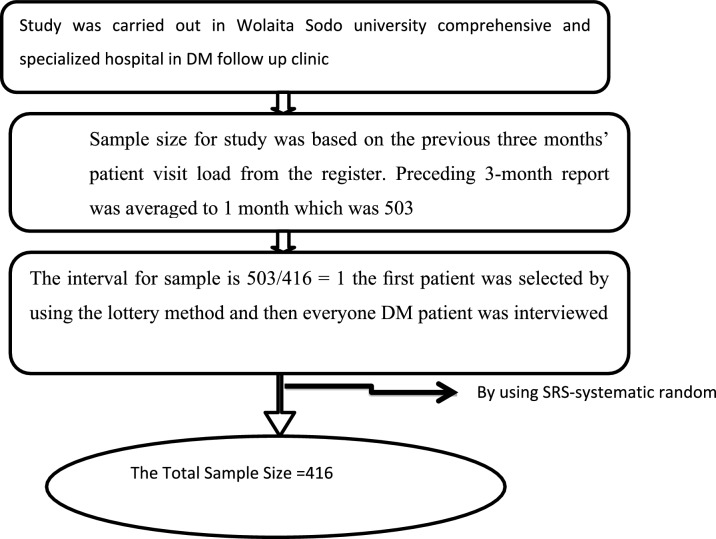 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Dietary Effects on Health · Diabetes, Cardiovascular Risks, and Lipoproteins
Introduction
Background
Type 2 diabetes mellitus (T2DM) is a major global public health challenge, accounting for the majority of diabetes cases worldwide and contributing substantially to morbidity, mortality, and health care costs. According to recent global estimates, the prevalence of diabetes has risen dramatically over the past few decades, driven by population aging, urbanization, unhealthy dietary patterns, and sedentary lifestyles. Low- and middle-income countries now bear a disproportionate share of this burden, with rapid increases in prevalence occurring alongside limited health system capacity to manage chronic non-communicable diseases effectively^1–3^.
Dietary intake plays a central role in the prevention and management of T2DM. Appropriate dietary practices are essential for maintaining glycemic control, preventing acute and chronic complications, and improving overall quality of life among people living with diabetes. Clinical and public health guidelines increasingly emphasize whole dietary patterns rather than individual nutrients, as people consume foods in combinations that may interact synergistically to influence metabolic health. Consequently, dietary pattern analysis has emerged as a valuable approach for understanding habitual dietary behaviors and their relationships with health outcomes^4–6^.
Evidence from high-income countries has consistently demonstrated that dietary patterns rich in whole grains, fruits, vegetables, legumes, and lean protein sources are associated with improved glycemic control and reduced cardio metabolic risk, whereas patterns characterized by high intakes of refined carbohydrates, saturated fats, sugary beverages, and processed foods are linked to poorer metabolic outcomes. However, dietary behaviors are strongly shaped by cultural, socioeconomic, occupational, and environmental contexts, limiting the generalizability of findings across different populations. Understanding locally specific dietary patterns is therefore critical for designing effective, culturally appropriate nutrition interventions^7,8^.
In sub-Saharan Africa, the burden of T2DM is increasing rapidly due to ongoing epidemiological and nutritional transitions. Traditional diets based on whole grains, legumes, and minimally processed foods are increasingly being replaced or supplemented by energy-dense, nutrient-poor foods. This shift is occurring alongside persistent food insecurity, poverty, and limited access to nutrition education, creating complex dietary environments for individuals with chronic diseases such as diabetes. Despite these challenges, evidence on dietary patterns and their determinants among people with T2DM in the region remains limited^9–11^.
Ethiopia is experiencing a growing burden of T2DM, particularly in urban and peri-urban areas. While national strategies emphasize lifestyle modification as a cornerstone of diabetes management, dietary counseling is often generalized and not sufficiently tailored to local food habits, cultural preferences, or socioeconomic realities. Many patients face difficulties in selecting appropriate foods, adhering to recommended meal plans, and balancing traditional dietary practices with clinical advice. In addition, nutrition knowledge, occupational status, comorbid conditions, and lifestyle factors may substantially influence dietary choices, yet these relationships are not well documented in the Ethiopian context^12,13^.
Previous studies in Ethiopia have largely focused on individual dietary components, glycemic control, or adherence to recommended diets, with limited attention given to empirically derive dietary patterns. Moreover, few studies have applied robust statistical methods, such as factor analysis, to identify prevailing dietary patterns among patients with T2DM and examine their associated factors. Existing evidence is further constrained by geographical concentration in selected urban centers, limiting insight into dietary behaviors in diverse settings.
Wolaita Zone, located in Southern Ethiopia, is characterized by unique cultural food practices and staple diets, including cereal- and enset-based foods. Wolaita Sodo University Comprehensive Specialized Hospital serves as a major referral center for diabetes care in the region, providing an important opportunity to investigate dietary behaviors among a heterogeneous patient population. However, to date, there is a paucity of evidence describing dietary patterns and their determinants among patients with T2DM attending this facility? The absence of such context-specific data hampers the development of targeted nutrition education and dietary counseling strategies tailored to the needs of patients in this setting.
Identifying prevailing dietary patterns and understanding the socio-demographic, clinical, and lifestyle factors associated with these patterns are essential for informing effective diabetes management strategies. Such evidence can support health professionals in delivering culturally appropriate dietary advice and guide policymakers in integrating nutrition-sensitive approaches into diabetes care programs.
Therefore, this study aimed to identify dietary patterns and examine their associated factors among adults with type 2 diabetes mellitus attending Wolaita Sodo University Comprehensive Specialized Hospital, Wolaita Zone*,* and Southern Ethiopia. By applying dietary pattern analysis, this study seeks to address existing evidence gaps and contribute locally relevant data to support improved nutritional management of T2DM in resource-limited settings.
Conceptual framework of dietary pattern and associated factors among type 2 diabetes mellitus patients
Clinical and Behavioral Factors Associated with Dietary Patterns (Fig. 1).Fig. 1. Conceptual frame work of dietary patterns and associated factors among type 2 diabetes mellitus patients^10,14–17^.
Methods and materials
Study setting
The study was conducted among adults with type 2 diabetes mellitus (T2DM) attending the diabetes follow-up clinic at Wolaita Sodo University Comprehensive Specialized Hospital (WSUCSH), located in Wolaita Sodo City, Wolaita Zone, and Southern Ethiopia. The hospital was established in 1927 by the Sudan Interior Mission and has evolved from a primary hospital to a general hospital, and subsequently to a teaching and referral hospital. In September 2021, the Ethiopian Ministry of Health officially upgraded it to a comprehensive specialized hospital.
WSUCSH serves as a major referral center for the region, providing outpatient, inpatient, and emergency services to more than 600,000 patients annually, with over 50,000 admissions per year. The hospital employs approximately 902 healthcare professionals across various disciplines, including nurses, physicians, laboratory technologists, pharmacists, anesthetists, radiologists, ophthalmic nurses, and environmental health professionals. The diabetes clinic is one of the five major outpatient departments, and on average, approximately 503 adults with T2DM attend the follow-up clinic each month.
Study design and period
An institution-based cross-sectional study was conducted among adults with T2DM attending the diabetes follow-up clinic at WSUCSH. Data collection was carried out from March 2023 to April 2024.
Population
Source population
All adults diagnosed with type 2 diabetes mellitus and registered for follow-up care at the outpatient diabetes clinic of WSUCSH constituted the source population.
Study population
The study population comprised systematically selected adults with T2DM who attended the diabetes follow-up clinic at WSUCSH during the data collection period**.**
Inclusion and exclusion criteria
Inclusion criteria
Adults aged 18 years and above with a confirmed diagnosis of type 2 diabetes mellitus who had at least one follow-up visit prior to the data collection period were eligible for inclusion.
Exclusion criteria
A patient who was critically ill or required immediate medical intervention at the time of data collection was excluded from the study.
Sample size determination
The sample size was determined using the single population proportion formula:
where n is the required sample size, Z is the standard normal value at 95% confidence level (1.96), p is the estimated proportion, and d is the margin of error (0.05).
For the primary objective, the proportion of dietary pattern prevalence (p = 44.1%) was taken from a previous study conducted in Addis Ababa among patients with T2DM. Based on this assumption, the calculated sample size was 379. After adding a 10% allowance for non-response, the final sample size was set at 416 participants.
For the secondary objective, sample size estimation was also checked using factors significantly associated with dietary patterns reported in previous studies, such as monthly income and educational status. The largest calculated sample size (n = 374) was smaller than the sample size obtained for the primary objective; therefore, the final sample size of 416 was considered adequate to address both objectives (Table 1).Table 1. Sample size determination for the second specific objective based on factors associated with dietary patterns among patients with type 2 diabetes mellitus.Relevant factorAOR95%CIP = proportionSample sizeMonthly income^18^2.3(1.2,4.6)72.7%305Educational status^14^2.65(1.62,4.32)58.2%374
Sampling procedure
The average monthly flow of adults with T2DM attending the diabetes follow-up clinic during the three months preceding data collection was obtained from hospital records (470, 490, and 550 patients, respectively), yielding an average monthly attendance of approximately 503 patients.
Systematic random sampling was employed to select study participants. The sampling interval (k) was determined by dividing the total estimated number of patients expected during the data collection period by the required sample size. Because the average monthly patient flow was comparable to the required sample size, eligible patients were recruited consecutively until the target sample size was achieved. On each clinic day, the first participant was selected using a simple random method, and all eligible patients were then approached sequentially until the required number was obtained (Fig. 2).Fig. 2. Shows Diagrammatic presentation of the sampling procedure of dietary patterns and associated factor among type 2 diabetes mellitus patients.
Data collection tools and procedures
Data were collected using a structured interviewer-administered questionnaire consisting of socio-demographic characteristics, clinical and lifestyle factors, nutrition knowledge, and dietary intake assessment. Dietary intake was assessed using a semi-quantitative food frequency questionnaire (FFQ) containing 27 food items commonly consumed in the study area. Participants were asked to report the frequency of consumption of each food item over the previous one week. The FFQ was adapted from previous studies conducted in similar settings and contextualized to local dietary habits.
Questionnaire translation and quality assurance
The questionnaire was initially prepared in English and then translated into Amharic by a bilingual public health professional. A separate bilingual expert independently back-translated the Amharic version into English to ensure consistency and conceptual equivalence. Discrepancies were resolved through discussion among the research team. A pretest was conducted on 5% of the sample size at a nearby hospital not included in the study, and necessary modifications were made accordingly. Data collectors and supervisors received training prior to data collection, and daily supervision was conducted to ensure data completeness and consistency.
Statistical analysis
Data were entered into EpiData version 4.6 and exported to SPSS version 26 for analysis. Descriptive statistics were used to summarize participant characteristics. Dietary patterns were identified using principal component analysis (PCA). The suitability of the data for PCA was assessed using the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. Factors with eigenvalues greater than 1.0 were retained, and varimax rotation was applied to improve interpretability. Food items with factor loadings ≥ 0.30 were considered significant contributors to each dietary pattern. Dietary patterns were named based on the food items with the highest factor loadings.
Factor scores for each dietary pattern were calculated and used as dependent variables in multiple linear regression models to identify associated factors. Variables with a p-value < 0.25 in bivariable analysis were entered into the multivariable models. Statistical significance was declared at p < 0.05 and results were reported using standardized regression coefficients (β) with 95% confidence intervals.
Study variables
Dependent variable
Dietary patterns: The dietary patterns in our study were named after the food items or groups with the highest loadings in factor analysis.
Independent variables
- Socio-demographic: Age, sex, marital status, wealth index, respondents’ residence, educational status and respondent’s occupations.
- Knowledge related factors: nutritional knowledge, doctor advice.
- Health and health related factors: member of association, comorbidity, family history and FBS.
- Life style factors: regular physical activity, smoking.
Operational definitions
- Dietary pattern: quantities, proportions, variety or combination of different foods and beverages in diets and the frequency with which they are habitually consumed.
- Good Controlled Glycemia -Fasting blood sugar ≥ 70 mg\dl and ≤ 130 mg mg\dl.
- Poorly controlled Glycemia -Fasting blood sugar > 130 mg\dl and ≤ 70 mg\dl.
- High level dietary Knowledge – Study participants who had scored above mean score knowledge questions asked.
- Low level dietary Knowledge-Study participants who had score less than mean score from knowledge questions asked.
- Comorbidities: the presence of one or more additional disease.
- Mixed dietary pattern: comprised animal-source foods with added sugars refined carbohydrates and consumption of carrot, dinich tibes, key sir, mucho, kik wote, kocho kita and kidney beans.
- A traditional dietary pattern: was characterized by the consumption of carrot, Dinich tibes, key sir, mucho, kik wote, kocho kita and kidney beans.
Ethical consideration
The ethical approval letter was obtained from Wolaita Sodo University College of Medicine and Health Science Institution of Review Board (IRB). An official supporting letter was obtained from the Department of Public health. Before data collection, informed consent was obtained from each study participant. All respondents were informed about the objective of the study and confidentiality was maintained at each step of data collection and processing. The respondents were informed that the information obtained in this study was used only for research purposes. Data collection facilitators were trained strongly on how to keep participants’ confidentiality. Also, an explanation about the rights of participants including their full right to not participate at all or withdraw at any time was provided.
All ethical procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki for research involving human subjects. This ethical framework ensured the protection of participants’ rights, dignity, and well-being, and fostered mutual trust and cooperation throughout the research process.
Result
Socio-demographic characteristics of study participants
A total of 416 adults with type 2 diabetes mellitus participated in the study. Of these, 252 (60.5%) were male and 164 (39.5%) were female. Slightly more than half of the participants resided in urban areas (54.3%), while 45.7% were from rural settings. The mean age of participants was 47.4 years (SD ± 12.45).
Regarding marital status, 196 (47.1%) were married, 118 (28.5%) were single, 62 (15.0%) were widowed, and 37 (8.9%) were divorced. In terms of educational attainment, 102 (24.4%) had completed primary education, 137 (33.0%) had attended secondary school, 101 (24.2%) had college-level education or above, and 76 (17.9%) had no formal education.
Occupationally, 69 (16.7%) were government employees, 99 (23.9%) worked in private organizations, 109 (26.1%) were farmers, 69 (16.5%) were merchants, 59 (14.1%) were students, 25 (6.0%) were daily laborers, and 26 (6.2%) were housewives.
Health profile of participants
Among the study participants, 153 (36.8%) reported a family history of diabetes mellitus, and 150 (36.1%) had at least one comorbid condition. Regarding diabetes management, 137 (33.0%) were using oral hypoglycemic agents, 99 (23.7%) were on insulin therapy, and only 109 (26.3%) reported using dietary modification as a primary method for glycemic control. More than half of the participants (54.3%) indicated that they had changed their dietary habits after being diagnosed with diabetes.
Dietary knowledge of participants
Overall, 153 (36.8%) participants demonstrated a low level of dietary knowledge, while 263 (63.2%) had a high level of knowledge regarding recommended dietary practices for diabetes management.
Regarding lifestyle modification, 172 (41.1%) identified dietary modification as a means of glycemic control, 139 (33.3%) mentioned physical exercise, and 104 (24.2%) reported no knowledge of lifestyle modification strategies. Only 95 (22.7%) correctly identified carbohydrates as the food group that raises blood glucose levels most rapidly, while 112 (26.8%) were unable to identify any specific food group.
Misconceptions were common: 212 (50.7%) believed that skipping meals could help control blood glucose levels. Although 219 (52.4%) correctly identified consuming whole fruits as preferable to fruit juice, only 73 (17.5%) correctly identified that half of the plate should consist of fruits and vegetables (Table 2).Table 2. Summaries detailed dietary knowledge responses od adults with type 2 diabetes mellitus attending wolaita Sodo Sodo University comprehensive specialized Hospital ,southern Ethiopia 2024.VariablesResponsesYes%Life style modificationExercise13933.3Dietary modification17241.1I don’t know10424.2Which of food groups raises blood glucose relatively faster?Carbohydrates9522.7Fiber13031Fat10023.9Protein276.5Which of the following should you do to control your blood glucose?Eating foods prepared only of barely9723.2To eat from different cereal13632.5To take food small or no sugar12730.4To skip breakfast and dinner5613.5Which one is source of carbohydrate?Barley, tef, bread, rice13131.3Meat,egg,milk,yoghurt11226.8Don’t know11226.8Which type food group should a person with DM advised to eat most of the time?Milk, yogurt, cheese9727.3Fat, oils ,sweets13833Vegetable and fruit11828.2Meat,fish,poultry6315.1Which food helps to achieve good glycemic control? (Multiple answers are possible)Eating fruits daily10324.6Avoiding cereals15034.9Eating fiber10324.6I don’t know246Which one is good to control blood glucose on a person with diabetesJuices19546,7Eating fruits without juicing21952.4On person with diabetes what proportion of the plate should be vegetable and fruit?1/27317.51/36315.11/47016.7I don’t know20849.6Do you believe that skipping meal can help you control your blood glucose level?Yes I do believe so21250.7No I don’t believe so20348.6How many servings of fruits and vegetables do you think you have to eat on daily bases?Once11928.52–4 times17441.6I don’t now12229.3Which fat do experts say is most important for people to cut down on?Liquid oils15136.1Fats and butter16940.4Not sure9422.5According to the food pyramid Which foods do you think you have to cut down a lotFruits and vegetables9222Milk and milk products13432.1Sweets9623Which one is healthyButter13532.3Olive oil18243.5Don’t know9723.2How many regular meals do you think you have to eat dailyOne meal10726.7Two meals15737.6Three meals10429.4Don’t know4811.5How many Snacks do you think you have to eat dailyOne snackThree Snacks14334.2Two snacks10124.2Don’t know5412.9
Dietary patterns identified by principal component analysis
Principal component analysis identified two major dietary patterns that together explained 20.7% of the total variance in food consumption. The Kaiser Meyer Olkin measure and Bartlett’s test confirmed the suitability of the data for factor analysis.
The mixed dietary pattern, accounting for 10.6% of the variance, was characterized by high consumption of raw meat, kitifo (raw beef with butter and chili), boiled beef, eggs, yogurt, sugar-sweetened beverages (Coca-Cola and Sprite), tea, and baked false banana.
The traditional dietary pattern, explaining 10.1% of the variance, was characterized by higher intake of bread, potatoes, carrots, beetroot, false banana porridge (mucho), broad bean sauce, kidney beans, and local alcoholic beverages (tella) (Table 3).Table 3. Factor loadings for each food item are presented in Table 3.Dietary patternFood items/groupsTraditional patternMixed patternUniquenessbread0.41490.21590.78Macaroni0.18690.35160.84False banana baked0.17140.45570.76Potato roasted0.472− 0.020.77Carrot0.41720.07380.82Keyisir(beetroot)0.57480.00380.66Mucho(false bannanaporridge)0.51900.01690.73Selata0.29310.13320.89Broad been sauce0.41940.08080.81Kidney benes0.5431− 0.02690.70Papaya0.24520.23200.88Orange0.29250.19790.87Pineapple0.26470.34110.81Raw meat− 0.01100.54830.69beef meat sauce0.070.370.85beef meat boiled0.30.310.80(Kitifo)Beef, raw + butter + birds eye chili− 0.0350.60.62Yoghurt0.30080.31870.62Egg0.20620.480.72Coca-Cola− 0.09800.550.68Sprite0.20060.320.85Tea0.190.250.89Tela(local alcoholic beverages0.28610.24170.85Factor loadings ≥ 0.30 were considered significant.
Distribution of dietary pattern scores
Participants were categorized into tertiles (T1–T3) based on dietary pattern scores. A higher proportion of males was observed in the highest tertile of the traditional dietary pattern, whereas females were more frequently represented in the lowest tertile of the mixed dietary pattern. Participants residing in rural areas were more commonly represented in the middle tertile of the traditional dietary pattern (Table 3).
Educational status showed variation across tertiles: participants with college-level education or higher were more frequently represented in the lower tertile of the traditional dietary pattern, while those with primary education were more commonly observed in the middle tertile of the mixed dietary pattern (Table 4).Table 4. Distribution of dietary pattern tertile by selected socio-demographic and clinical characteristics among adults with type 2 diabetes mellitus, 2024.Variables N = 416Dietary patternsTraditional patternMixed patternT1T2T3T1T2T3− Sexn (%)n (%)n (%)n (%)n (%)n (%) Female57(35.4)57(35.4)47(29.2)63(39.1)47(29.2)51(31.7) Male80(31.9)80(31.9)91(36.3)74(29.5)90(35.9)87(34.7)Age 27–3412(25.5)19(40.4)16(34)14(29.8)17(36.2)16(34) 35–4453(34.6)50(32.7)50(32.7)48(31.4)53(34.6)52(34) 45–5429(28.7)36(35.6)36(35.6)36(35.6)31(30.7)34(33.7) 55–8243(38.7)32(28.8)36(32.4)39(35.1)36(32.4)36(32.4)Residence Urban65(34.6)56(29.8)67(35.6)61(32.4)58(30.9)69(36.7) Rural72(32.1)81(36.2)71(31.7)76(33.9)79(35.3)69(30.8)Educational status Primary36(35.3)31(30.4)35(34.3)28(27.5)38(37.3)36(35.3) High school37(27.4)54(40)44(32.6)49(36.3)46(34.1)40(29.6) College and above38(38)27(27)35(35)32(32)34(34)34(34) No education26(34.7)25(33.3)24(32)28(37.3)19(25.3)28(37.3)Wealth index Poor41(29.9)42(30.7)54(39.4)42(30.7)55(40.1)40(29.2) Middle46(33.6)45(32.8)46(33.6)47(34.3)38(27.7)52(38) Rich50(36.8)49(36)37(27.2)46(33.8)44(32.4)46(33.8)Other comorbidity diseases Yes46(30.7)41(27.3)63(42)42(28)50(33.3)58(38.7) No91(34.7)96(36.6)75(28.4)95(36.3)87(33.2)80(30.5)DM association member Yes67(30.7)80(36.7)71(32.6)59(30.4)61(31.4)74(38.1) No67(30.7)80(36.7)71(32.6)78(35.8)76(34.9)64(29.4)Doctor advice Yes77(33.3)79(34.2)75(32.5)70(30.3)75(32.5)86(37.2) No60(33.1)58(32.0)63(34.8)67(37)62(34.3)52(28.7)Physical activity Yes70(33.2)74(35.1)67(31.8)66(31.3)69(32.776(36) No67(33.3)63(31.3)71(35.3)71(35.3)68(33.8)62(30.8)Knowledge on recommended diet High level57(37.5)40(26.3)55(36.2)15(45.5)11(33.3)7(21.2) Low level80(30.8)97(37.3)83(31.9)35(37.2)12(25.5)7(14.9)
Factors associated with dietary patterns
Variables with a p-value < 0.25 in bivariable linear regression were entered into multivariable linear regression models to identify independent factors associated with each dietary pattern.
Traditional dietary pattern
In the multivariable model, the presence of comorbid conditions was inversely associated with adherence to the traditional dietary pattern (adjusted β = − 0.45; 95% CI − 0.77, − 0.13; p < 0.01). Older age was positively associated with the traditional dietary pattern among participants aged 45–54 years (adjusted β = 0.52; 95% CI 0.01, 1.03; p = 0.04) and 55–82 years (adjusted β = 0.56; 95% CI 0.06, 1.08; p = 0.03) (Table 5).Table 5. The detailed results of the regression analysis are presented in Table 5.Variables N = 416Traditional patternCrudeβ (95% CI)Adjusted β (95% CI) Sex− 0.078(− 0.27,0.12)0.09(− 0.23,0.4) Residence0.048(− 0.26,0.36)0.037(− 0.27,0.35)Age 35–44− 0.19(− 0.52,0.13)0.02(− 0.25,0.7) 45–54− 0.069(− 0.4,0.27)0.5(0.010,1.028) 55–82− 0.11(− 0.45, 0.23)0.56(0.058,1.075)Marital status Married− 0.06(− 0.29,0.167)− 0.004(− 0.37,0.36) Widowed− 0.17(− 0.46,0.10)− 0.08(− 0.57,0.4) Divorced− 0.2(− 0.37,0.33)− 0.24(− 79,0.3) Did you have other comorbidity diseases (no)0.2(0.038,0.438)− 0.45(− 0.77,.− 13) Physical exercise(no)0.057(− 0.136,0.25)0.18(− 0.12,0.49) Are you a member of diabetic associations? (no)0.4(− 0.14,0.23)− 0.2(− 0.56,0.06) Knowledge level− 0.3(− 0.6,0.02)− 0.30(− 0.09,0.8)Wealth index Middle0.16(− 0.21,0.53)0.18(− 0.18,0.55) Rich− 0.126(− 0.36,0.11)− 0.24(− 0.6,0.13)Variables with p < 0.25 in bivariable analysis were entered into the multivariable linear regression model. Statistical significance declared at p < 0.05.
Mixed dietary pattern
Occupational status was significantly associated with the mixed dietary pattern. Being a daily laborer was positively associated with higher adherence to the mixed dietary pattern (adjusted β = 0.10; 95% CI 0.03, 0.18; p = 0.01). No significant associations were observed with sex, residence, educational status, comorbidity status, or dietary knowledge after adjustment.
Factor loadings of food items for identified dietary patterns among adults with type 2 diabetes mellitus at Wolaita Sodo University Comprehensive Specialized Hospital, Southern Ethiopia, 2024 (Table 6).Table 6. Presents the multivariable regression results for the mixed dietary pattern.Variables N = 416Mixed patternCrude β (95% CI)Adjusted β (95% CI)Sex− 0.3(− 76,0.07)− 0.2(− 6,0.2)Residence− 0.17(− 0.37,0.01)− 0.138(− 0.59,0.3)Age0.035(− 0.29,0.36)− 0.2(− 0.9,0.49)35–44− 0.07(− 0.42,0.27)− 0.5(− 1.2,0.2)45–54− 0.07(.− 41,0.265)− 0.35(− 1.0,0.38)55–82− 0.07(.− 41,0.265)− 0.35(− 1.0,0.38)Occupations0.6(− 0.15,1.07)1.2(0.3,0.2)Daily laborer− 0.13(− 0.43,0.17)0.09(− 0.57,0.77)Private organization− 0.16(− 0.46,0.135)− 0.2(− 0.8 , 0.4)Farmer− 0.02(− 0.35,0.3)0.5(− 0.18,0.1.27)Merchant0.29(− 0.23,0.8)− 0.1(− 0.1,0.9)Student0.2(− 0.20,0.69)0.58(− 0.3,1.4)House wife0.2(− 0.20,0.69)0.58(− 0.3,1.4)Educational status0.07(− 0.14,0.3)− 0.26(− 0.89,0.37)Primary− 0.1(− 0.38,0.12)0.08(− 0.56,0.7)high school− 0.01(− 0.29,0.26)− 0.3(− 0.97,0.3)College and above− 0.01(− 0.29,0.26)− 0.3(− 0.97,0.3)Did you have other comorbidity diseases(no)− 0.19(− 0.39,0.0089)− 0.3(− 0.75,0.1)Do you have Family history of diabetes(yes)− 0.19(− 0.39,0.0089)− 0.3(− 0.75,0.1)Have you made a Complete change of your dietary habit when you know you are diabetic(no)0.02(− 0.17,0.2)− 0.27(− 0.69,0.15)Does your doctor give you advice about dietary pattern to be followed (no)− 0.16(− 0.35,0.03)− 0.3(− 0.7,0.12)Knowledge level(low level)− 0.008(− 0.2,0.19)− 0.37(− 0.09,0.8)Adjusted β coefficients are from multivariable linear regression analysis; p < 0.05 considered statistically significant.
Descriptions of dietary patterns among patients who are on follow up in Wolaita Sodo comprehensive specialized hospital 2024.
Majority of female participant resided in lowest tertile of the mixed dietary pattern while majority of male participant reside in highest tertile of traditional dietary pattern.
Participants with the highest tertile of the mixed dietary patterns tended to reside equally in urban and rural area, while those with the middle tertile of traditional dietary pattern resided more in the rural area.
Majority Participants, who completed primary education, reside on middle tertile of mixed dietary pattern while majority of participants, who completed High school education, resided in meddle tertile of traditional dietary pattern and participants who completed college and above education reside in lowest tertile of traditional dietary pattern. Participants, who have no education resided equally in both lowest and highest tertile of mixed dietary patterns (Table 4).
Discussion
This study explored dietary patterns and associated factors among adults with type 2 diabetes mellitus (T2DM) attending Wolaita Sodo University Comprehensive Specialized Hospital. Using principal component analysis (PCA), two major dietary patterns—traditional and mixed—were identified, together explaining 20.7% of the total variance in food intake.
Dietary patterns among type 2 diabetes patients
The traditional dietary pattern was characterized by consumption of bread, root vegetables, legumes, false banana–based foods, and local beverages such as tela. This pattern aligns with previous studies from Ethiopia and sub-Saharan Africa, where staple, plant-based foods remain predominant in adults’ diets^16^. Globally, similar plant-based patterns have been associated with better glycemic control and reduced cardiovascular risk^18,19^.
The mixed dietary pattern, which included raw and boiled meat, eggs, dairy products, sugar-sweetened beverages, and refined carbohydrates, resembles “Westernized” or diversified dietary patterns observed in urban populations worldwide^20,21^ . This reflects dietary transition due to urbanization, increased food availability, and exposure to processed foods. Similar findings have been reported among patients with T2DM in other African countries, including Kenya^14^ and urban Ethiopia^22^.
Factors associated with dietary patterns
In this study, age was positively associated with adherence to the traditional dietary pattern, particularly among participants aged 45–82 years. This finding is consistent with global and regional evidence showing older adults often maintain culturally ingrained eating habits, whereas younger individuals tend to adopt more Westernized diets^9,23^.
Participants with other comorbidities were less likely to follow the traditional dietary pattern, suggesting that health conditions may prompt dietary modifications away from staple foods^21,24^.
For the mixed dietary pattern, occupational status was a significant factor. Daily laborers were more likely to adhere to this pattern, possibly due to the need for high-energy, convenient foods and limited time for meal preparation. This aligns with previous studies linking informal employment and high-energy food consumption among adults with diabetes in Ethiopia and other low- and middle-income countries^25,26^.
Interestingly, dietary knowledge was not significantly associated with either dietary pattern after adjustment, indicating that awareness alone may not translate into practice due to economic constraints, cultural preferences, and limited access to diabetes-specific nutrition counseling. Similar patterns have been observed in Ethiopia^14,27^.
Comparison with local studies
The current findings confirm previous Ethiopian studies showing mixed adherence to dietary recommendations among adults with T2DM. For instance, studies from Addis Ababa and Jimma reported that patients often combine traditional staples with high-fat or sugar-rich foods, similar to the mixed pattern identified in this study^16,24^. This highlights persistent gaps in dietary counseling and behavioral adoption of recommended diets.
Implications for practice
The coexistence of traditional and mixed dietary patterns underscores the need for context-specific nutrition interventions. Encouraging the consumption of plant-based traditional foods while moderating animal-source foods, added sugars, and processed products may improve glycemic control. Targeted interventions for daily laborers and other at-risk occupational groups are warranted. Integrating dietitians into chronic care, strengthening education programs, and promoting affordable local foods may enhance adherence to healthier dietary patterns^2,28^.
Strengths and limitations
Strengths of this study include the use of PCA to identify dietary patterns and a relatively large, representative sample. Limitations include the cross-sectional design, which prevents causal inference, and reliance on self-reported dietary intake, which may be subject to recall bias. Despite these limitations, the findings provide valuable insight into dietary behaviors among T2DM patients in a resource-limited setting.
Conclusion
This study identified two major dietary patterns among adults with type 2 diabetes mellitus in Wolaita Sodo, Southern Ethiopia: a traditional pattern and a mixed pattern, together explaining 20.7% of the total variance in dietary intake. The traditional pattern was positively associated with older age and inversely associated with comorbid conditions, while the mixed pattern was more common among daily laborers.
These findings highlight that dietary behavior among T2DM patients is influenced by socio demographic, occupational, and health factors, and not solely by knowledge. Nutrition interventions should therefore be context-specific, culturally appropriate, and targeted to high-risk groups. Encouraging the maintenance of beneficial traditional foods while moderating sugar and animal-source food intake may improve glycemic control and overall health outcomes in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO/FAO. Diet, nutrition and the prevention of chronic diseases. WHO Technical Report Series 916. Geneva 2003.12768890 · pubmed ↗
- 2Food and Agriculture Organization of the United Nations. The State of Food Security and Nutrition in the World 2022: Repurposing food and agricultural policies to make healthy diets more affordable (Rome, FAO, 2022). 10.4060/cc 0639 en.