The quality of life of parents of children with disabilities in Saudi Arabia: a systematic review
Abdullah Ahmed Alghamdi, Mohammad S. Alzahrani, Atiah H. Almalki, Majed A. Algarni

TL;DR
This systematic review explores the quality of life of parents and caregivers of children with disabilities in Saudi Arabia, finding significant challenges linked to employment, income, and access to support.
Contribution
The study provides the first systematic review of quality of life for caregivers of children with disabilities in Saudi Arabia, highlighting key demographic and socioeconomic factors.
Findings
Caregivers with lower income, unemployment, and limited education report poorer quality of life.
Mothers and caregivers of children with severe disabilities experience the lowest quality of life.
Physical, social, and environmental domains of quality of life are most affected among caregivers.
Abstract
The quality of life (QoL) of parents and caregivers of children with disabilities in Saudi Arabia is examined in this systematic review. Fourteen cross-sectional studies published between 2020 and 2024 are included, encompassing 1,841 caregivers, of whom 60.2% are mothers, 23.1% fathers, and 18.4% other caregivers, caring for 1,460 children with disabilities. QoL is primarily assessed using the WHOQOL-BREF in 10 studies, followed by the SF-36 in two studies and the Beach Center Family Quality of Life Scale in one study. Autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), cerebral palsy (CP), and Down syndrome (DS) are the most commonly reported conditions. Negative QoL outcomes are reported in at least one domain in 9 of the 10 WHOQOL-BREF studies. The physical domain is most frequently affected (50% of studies), followed by the social and environmental…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
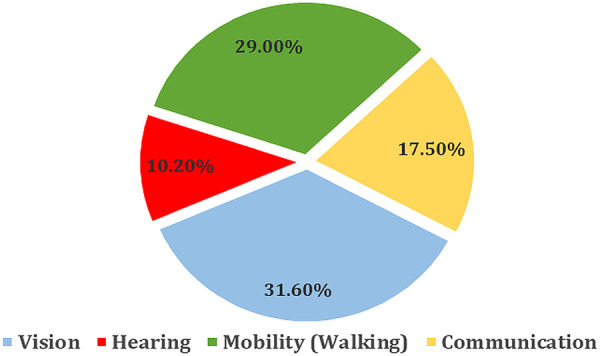 Figure 1
Figure 1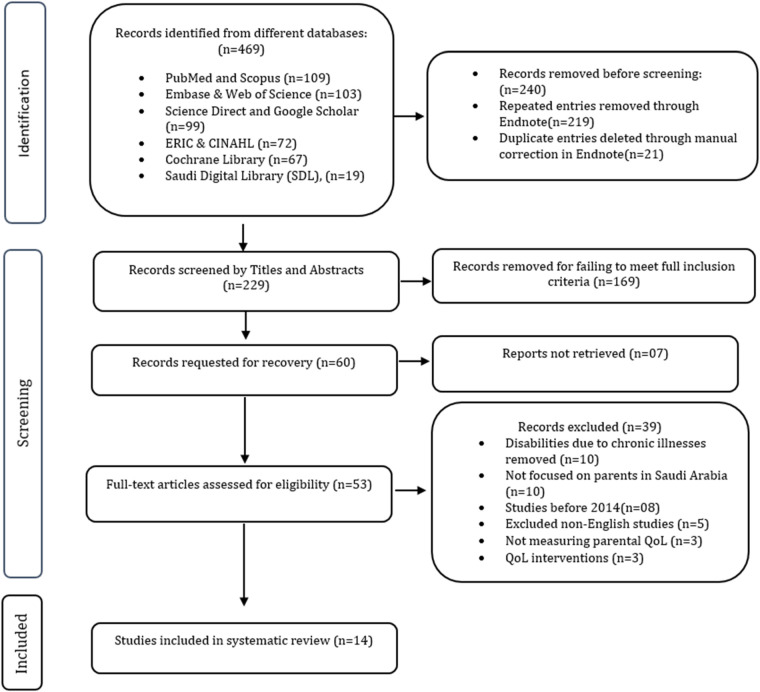 Figure 2
Figure 2| No. | Research question | Primary focus/description |
|---|---|---|
| 1 | How does the quality of life of parents or caregivers vary across different sociodemographic factors? | Examines the influence of gender, employment status, education level, marital status, and income on caregiver quality of life to identify disparities and vulnerable groups. |
| 2 | How do different types and severities of disabilities affect the quality of life of parents? | Assesses the impact of autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), cerebral palsy (CP), and Down syndrome (DS), as well as the relationship between disability severity and caregiver burden. |
| 3 | Are there differences in QoL outcomes between mothers and other caregivers such as fathers or extended family members? | Compares quality of life outcomes across caregiver roles to identify gender related caregiving burdens and differences in coping mechanisms. |
| 4 | Which quality of life domains are most affected including physical, psychological, social, and environmental domains? | Identifies the domains of caregivers' lives that are most impacted to inform targeted support and resource allocation. |
| 5 | How do social and governmental support systems affect the quality of life of parents of children with disabilities? | Evaluates the role of rehabilitation services, financial support, and societal interventions in improving caregiver well-being and reducing caregiving burden. |
| References | Study objective | QOL measures | Disease/condition | Findings/results |
|---|---|---|---|---|
| Alnahdi et al. ( | Family QOL of caregivers in Saudi Arabia | Beach Center Family Quality of Life Scale | ASD, intellectual disabilities, and others. | Caregivers of individuals with ASD reported lower satisfaction, especially in emotional and material well-being. Fathers reported lower satisfaction with family interaction and parenting. Gaps in emotional and material support were highlighted. |
| Al-Janabi et al. ( | To identify independent demographic and social predictors of parents' quality of life so support can be directed to those most in need. | QOL and social support were measured using a structured self-administered questionnaire assessing multiple domains of QoL (e.g., health perception, physical functioning, mental and social functioning). | ASD | Parents experienced lower QoL, especially in mental and social domains. Factors associated with poorer QoL included being a mother, having a chronic condition, having a female child or a child with comorbidities. Marital satisfaction was linked to better QoL in most areas. Multiple regression was significant for all domains except role functioning ( |
| Manee et al. ( | QOL of Arab mothers caring for children with disabilities in Kuwait | WHOQOL-BREF | Autism, CP, DS, developmental delay | Mothers of children with disabilities had significantly lower QOL across all domains compared to those with typical children. The nuclear family was the primary support source, while formal support systems were largely unavailable. |
| Romaniuk et al. ( | Family QOL for children with ASC, ADHC, or both conditions | Family QOL Scale | Autism, ADHD | Families of children with both conditions reported lower emotional well-being than those with ASC alone. Highlighted the need for further research into dual-condition challenges. |
| Alhammad et al. ( | Impact of walking ability on QOL in children with DS in Saudi Arabia | Pediatric QOL Inventory | DS | Children with DS walked shorter distances and had lower QOL in physical, social, and school domains. Early interventions to improve walking ability were recommended. |
| Asdaq et al. ( | Relationship between depression, QOL, and COVID-19 challenges | WHOQOL-BREF | Disabilities during COVID-19 | Depression higher in unvaccinated individuals. Vaccination and physical activity linked to better QOL. Most participants reported satisfactory overall QOL but low satisfaction in physical and psychological health. |
| Asiri et al. ( | To summarize the overall QoL of caregivers of children with disabilities in Saudi Arabia and identify factors affecting caregivers' well-being. | Most studies used WHOQOL-BREF, SF-36, or similar tools to measure caregivers' physical, psychological, social, and environmental QoL | Children with various disabilities (e.g., CP, ASD, DS, learning disabilities) cared for by family caregivers in Saudi Arabia. | Caregivers of disabled children had reduced QoL in multiple domains, especially physical, psychological, and social relationships. Factors such as gender, age, and low income were found to negatively impact caregiver QoL. |
| Ref. | Study DESIGN | Mothers/fathers | Employment (full/part-time) | Type of disability | Age (years) | Age of child with disability (years) | QoL measure | Support from services |
|
|---|---|---|---|---|---|---|---|---|---|
| Subke et al. ( | Cross-sectional study | 58.5% were mothers, 41.5% were fathers. | 56.5% of parents were employed | ASD. | Parents' ages ranged from 23 to 45 years, with a mean age of 34.46 ± 4.7 years. | Children aged between 2 and 14 years, all clinically diagnosed with ASD at least 3 months before the study. | WHOQOL-BREF | N/A | N/A |
| Alhefdhi et al. ( | Cross-sectional | Mothers: 66% Fathers: 34% | Teachers: 32% | ADHD | Majority were young to middle-aged adults. | 1–5 years: 62% | WHOQOL-BREF (Arabic version) | Limited support from schools; workshops attended by 54%. | ADHD-related psychological burden; discrimination. |
| Housewives: 12% | 6–10 years: 8% | ||||||||
| Businesspeople: 8% | 11–15 years: 3% | ||||||||
| Engineers: 3%% | 16–18 years: 27% | ||||||||
| Unemployed: 5 | |||||||||
| Tedla et al. ( | Cross-sectional | Mothers: 111 Fathers: 1 Grandparents/Staff: 20 | The study did not explicitly categorize employment as full-time or part-time. However, it mentioned that the majority of caregivers were mothers (111 out of 132 participants) | Cerebral Palsy (CP) | Caregiver age: 41.53 ± 6.78 | 2–18 years | PedsQL 3.0 CP Module | Rehabilitation and special education services. | N/A |
| Tedla et al. ( | Cross-sectional cohort study | All caregivers were women, primarily mothers (85.84%), with 14.16% female maids. | N/A | Cerebral palsy (various types). | Mean caregiver age: 40.38 years (SD ± 7.09). | Mean age of children with CP: 7.55 years (SD ± 3.04), children aged between 2 and 12 years. | WHOQOL-BREF (Arabic version) | 55.7% received financial support from the government; 44.3% reported excellent external support. | Not specified |
| Asdaq et al. ( | Cross-sectional study | Not specified | 34.2% employed; remaining 65.8% were unemployed or inactive. | Physical (35.1%), sensory (24.3%), intellectual, and developmental disabilities. | Majority are over 36 years old. |
| WHOQOL-BREF | 73.9% had access to telehealth services. | 75.7% had a concomitant medical condition. |
| Alasiri et al. ( | Cross-sectional | Predominantly mothers (59.8%), Fathers accounted for 33.3%, while other relatives (siblings or others) made up a small proportion (6.9%). | Unemployed: 31.4% | ASD | Adults: Majority 30–49 years | Children: 1–14 years | Beach Center Family QoL Scale | Services included speech therapy, behavioral therapy, special education | Severity of ASD noted (Level 1–3); No other comorbidities explicitly listed |
| Government sector (full-time/part-time): 40.2% | |||||||||
| Private sector (full-time/part-time): 17.6% | |||||||||
| Students: 2.0% | |||||||||
| Retired: 8.8% | |||||||||
| Zahra et al. ( | Cross-sectional study | Not specified. | Not specified. | Physical disabilities, including stroke and amputations. | Not specified | Participants aged 15 years and older. | WHOQOL-BREF | Rehabilitation services from Rehabilitation Hospital, Madinah. | Chronic diseases were included in the analysis as influencing PA levels. |
| Algadeeb et al. ( | Cross-sectional study | Mothers (46.6%) and fathers (49.5%) comprised the majority of caregivers. | Employed caregivers were the largest group (64.1%), followed by homemakers (26.2%). | ADHD | Caregivers' ages ranged from 14 to 57 years, with a mean age of 36.83 years. | Most children were aged 7–10 years (37.9%), followed by 4–6 years (34.0%). | WHOQOL-BREF | Majority received help from spouses (66%), and some relied on extended family or specialists. | No specific comorbidities were emphasized in the study. |
| AlAhmari et al. ( | Cross-sectional | 261 caregivers of children with DS | Not specified in detail, general demographic focus on education and income | Down syndrome | Majority above 40 (62.8%); some between 20 and 40 (36%) | 0–14 years | WHOQOL-BREF | Limited, with gaps in healthcare access and social integration | Excluded children with additional health issues |
| Alenezi, S et al. ( | Cross-sectional study | 93 mothers (59.6%) and 63 fathers (40.4% | 62.8% employed | ADHD | Mean: 40.9 | Mean: 10.03 years | WHOQOL-Brief | Neurodevelopmental centers | Learning difficulties (80.9%), autism (28.2%), separation anxiety (3.6%), Asperger's (3.6%) |
| Alenazi et al. ( | Cross-sectional study | Majority were mothers (80.9%), with fathers comprising 19.1% | Most caregivers were unemployed (69.1%), while 30.9% were employed | ASD | Parents' age groups: <40 years (54.8%), ≥40 years (45.2%) | <7 years (32.1%), 7–10 years (42.9%), >10 years (25.0%) | Short-form 36 (SF-36) health survey | Services from the developmental abnormalities clinic and Maternal and Children's Hospital in Arar City | N/A |
| Sulaimani et al. ( | Analytical cross-sectional study | Mothers ( | Employed ( | Physical disabilities (57.1%), Down syndrome (10.2%), Autism (6.1%) | 26–35 years (24.7%), 36–45 years (56.5%), 46–55 years (10.6%), 56+ (8.2%) | 1–5 years (15.6%), 6–10 years (40.0%), 11–18 years (44.4%) | RAND SF-36 (Short Form Health Survey) | Services from rehabilitation centers such as KFMC and Alawael Center | Presence of multiple disabilities noted (e.g., children with severe disabilities or comorbid conditions) |
| Al Awaji et al. ( | Comparative Cross-Sectional | Mothers only | 30.1% of MCD employed (lower than 55.9% in CON) | Autism spectrum disorder (24% of disabilities reported among MCD) | Mothers of Children with Disabilities (MCD): Most ≥36 years | ≤18 years | WHOQOL-BREF | Saudi government offers support through rehabilitation centers and annual funds for children with disabilities, though access was limited during a lockdown. | Common comorbidities reported for children with disabilities include Down syndrome (19%), physical impairments (23%), ADHD (7.5%), and sensory impairments (2%). |
| Alhazmi et al. ( | a cross-sectional study | 51% of fathers and 49% of mothers participated as primary caregivers | Employment status positively impacted the caregivers' quality of life, mainly through financial stability, but specific employment statistics were not provided | Among 54 children diagnosed with ASD by developmental pediatricians, 75.9% were males (41 children) and 24.1% were females (13 children). | The majority of parents in the study were aged 31–40 years (44.4%), followed by 41–50 years (38.9%), with smaller proportions aged 20–30 years (10.2%) and over 50 years (6.5%) | Children aged 1–14 years included in the study | WHOQOL-BREF | The study does not specify government support but suggests that financial stability, possibly through subsidies, improves the caregivers' quality of life | Attention-Deficit/Hyperactivity Disorder (ADHD), Aggression, Defiance, Destructive behaviors, Self-harm behaviors |
| Quality rating | Percentage of studies | Studies included | Observations |
|---|---|---|---|
| High (Good) | 71.43% | Tedla et al. ( | Studies were rated as high quality based on strong methodology, appropriate sampling strategies, robust data analysis, validated measurement tools, ethical considerations, relevance to QoL, and practical implications. All studies consistently received “Good” ratings in both review rounds (R1 and R2). Control groups were well defined and appropriately matched with disability groups. |
| Moderate | 28.57% | Alhefdhi et al. ( | Studies were rated as moderate quality due to some limitations in methodology, sampling procedures, or data analysis. However, all studies clearly stated their research objectives and provided strong rationales for the research. |
| Inter-rater Reliability | — | — | Two reviewers independently assessed all studies. Inter-rater agreement was strong, with Cohen's Kappa ( |
| SF | WHOQOL-BREF | BCFQoL Scale | PedsQL 3.0 CP Module | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. | Study Setting/Recruitment | Compared Groups | QoL Measure | VT | SF | RE | MH | PF | RP | BP | GH | PHY | PSY | SOC | ENV | FI | PP | EW | PMW | DRS | DA | SA | MB | PH | FA | EA | SC |
| ( | 132 CP children aged 2–18 recruited from hospitals and rehabilitation centers in SA. | Compared CP children based on mobility (GMFCS), age (2–18 years), and schooling (normal vs. special). | PedsQL 3.0 CP Module | ||||||||||||||||||||||||
| ( | SA; King Abdulaziz Medical City and online selection | Families of children with ASD | BC Family QoL Scale | ||||||||||||||||||||||||
| Disabled from Rehabilitation Hospital; non-disabled online selection in SA |
Individuals with physical disabilities ( Individuals without disabilities ( | WHOQOL-BREF |
|
|
| ||||||||||||||||||||||
| ( | Participants recruited from disability centers, hospitals, clinics, charity events, and health camps in SA | Individuals with disabilities, grouped by depression status, vaccination status, and disability severity. | WHOQOL-BREF | ||||||||||||||||||||||||
| ( | Data was collected at hospitals and disability centers over one year in SA. | Caregivers of children with CP, focusing on caregivers' demographics and child-related factors (e.g., mobility, education). | WHOQOL-BREF instrument, Arabic version | ||||||||||||||||||||||||
| ( | 100 parents of ADHD children recruited via social media and hospital records in SA | mothers vs. fathers | WHOQOL-BREF (Arabic version) | ||||||||||||||||||||||||
| ( | Conducted at the Developmental and Behavioral Disorders Center, Al-Ahsa; participants recruited via online surveys. | Caregivers of children with ADHD, focusing on sociodemographic variations such as gender, marital status, and employment. | WHOQOL-BREF | ||||||||||||||||||||||||
| ( | Tertiary care hospital in Riyadh; convenience sampling of Down syndrome caregivers. | Not explicitly grouped; all respondents were caregivers of children with Down syndrome | WHOQOL-BREF | ||||||||||||||||||||||||
| . ( | Conducted in SA, cross-sectional design. Recruitment through online surveys sent via neurodevelopmental centers. | Parents of children with ADHD, compared by income level, coping strategies (adaptive vs. maladaptive), gender, and employment status. | WHOQOL-BREF | ||||||||||||||||||||||||
| Conducted at King Saud Medical City, Riyadh; recruited parents of children with ASD (1–14 years). | The study analyzed intra-group differences in ASD parents based on socio-demographics. | WHOQOL-BREF | |||||||||||||||||||||||||
| ( | SA, during COVID-19 lockdown. Recruitment via online surveys (WhatsApp, Twitter, Facebook). | MCD vs. CON | WHOQOL-BREF | ||||||||||||||||||||||||
| ( | Conducted in Jeddah, at the Saudi National Center for Developmental and Behavioral Disorders, involving 200 parents of children with ASD. | Compared groups based on demographics: gender (male vs. female), employment (employed vs. unemployed), education level, and housing type. | WHOQOL-BREF | ||||||||||||||||||||||||
| ( | Conducted in Arar City, Saudi Arabia, at Maternal and Children's Hospital (Jan–Mar 2019). | Caregivers with impaired quality of life (63.1%) versus those without impairment. | Short-form 36 (SF-36) health survey with scores below 50 indicating poor QOL. | ||||||||||||||||||||||||
| ( | Rehabilitation centers in SA (Riyadh, Makkah); recruitment via social media and centers. | Mothers vs. other caregivers; Educated vs. non-educated caregivers. | RAND 36-Arabic version). | ||||||||||||||||||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily and Disability Support Research · Disability Rights and Representation · Parental Involvement in Education
Introduction
1
It has been shown that understanding disabilities among children is critical for public health surveillance, child welfare promotion, and the development of an inclusive society, which also provides a framework for analyzing how the needs of vulnerable populations evolve in relation to social, health, and environmental factors (1, 2). In Saudi Arabia, a nation that blends traditional and modern values, there has been a growing focus on examining disabilities in children under 18, as the country's unique cultural and social context is leading towards the need for more context-sensitive evidence (3, 4). In 2022, it was shown that a national survey in Saudi Arabia revealed that 1.8% of the population had disabilities, which can be employed to understand the prevalence and distribution of disability in the population. It was shown that 41.5% of children experienced a single disability, while 58.5% had multiple disabilities, which may increase the demand for integrated services. Vision impairments (31.6%), mobility issues (29%), communication difficulties (17.5%), and hearing impairments (10.2%) (see Figure 1) are the most prevalent, which could thus be used to prioritize healthcare and social support initiatives. The primary causes included illnesses (39.2%), congenital factors (26.9%), aging (16.1%), and traffic accidents (4.7%), which could thus be used to inform prevention strategies and interventions based on more than aggregate population statistics (5).
Percentage distribution of disabilities in children aged 2–4 years by type and severity (5).
Age, gender, socioeconomic status, and family structure are factors that are associated with how children and their families handle disabilities, thereby influencing both coping mechanisms and access to resources (6). Despite progress in addressing childhood disabilities in Saudi Arabia, challenges like unequal service access remain (7). This study is the first to explore the prevalence of disabilities among Saudi children, their coping strategies, and how social and personal factors influence their QoL, providing insights for evidence-based policies and targeted support (7–9).
Although caregiver and parental QoL have been examined internationally (10–15), the Saudi evidence base remains uneven and difficult to compare (6, 8, 14, 16). Most Saudi studies focus on one disability group at a time [e.g., autism or cerebral palsy (CP)], use cross-sectional designs, and rely on samples drawn from single settings or regions, which limits generalizability and prevents a clear national picture of parental QoL (1, 4, 8). In addition, findings are reported using different QoL instruments (e.g., WHOQOL-BREF, SF-36, Beach Center Family QoL) (13, 14), creating methodological heterogeneity that makes it hard to synthesize results consistently across conditions and caregiver groups. A Saudi-specific systematic review has been published (2023) (3), but the field has continued to develop, with newer studies (including 2024, 2025) extending evidence on family QoL and caregiver outcomes (6, 8, 14, 16). Furthermore, research guidance shows that using systematic methods, registered protocols, and careful quality checks helps reduce bias and produce more reliable conclusions (17–19). Therefore, an updated synthesis is needed to (i) integrate the expanding Saudi evidence across disability categories (1–4, 6, 8), (ii) summarize the most consistent determinants of poorer parental QoL (e.g., socioeconomic disadvantage and caregiver gender), and (iii) interpret these findings within Saudi Arabia's service and policy environment, where access to rehabilitation and family support is a key practical issue (5, 8). Accordingly, this systematic review updates and consolidates Saudi evidence on the QoL of parents/caregivers of children with disabilities and identifies the most consistent factors associated with poorer outcomes to inform targeted support and service planning.
Objectives and research questions
1.1
This systematic review seeks to evaluate the QoL of parents of children with disabilities in Saudi Arabia, which is especially important as it may be used to inform evidence-based interventions and policy enhancements. The objectives of this systematic review are structured around the research questions outlined in Table 1.
Literature review
2
There has been a growing recognition that ASD is a chronic neurodevelopmental condition, which can be used to explain difficulties in social interaction, communication, and repetitive behaviors or restricted interests. In Saudi Arabia, it was shown that approximately 1 in 40 children aged 2–4 years is diagnosed with ASD (20, 21). ASD varies in severity, with differing requirements for communication, social skills, and behavioral support, which is leading towards more context-specific interventions. Many children with ASD also have co-existing challenges, such as cognitive delays, language difficulties, and anxiety, which could be used to understand the daily functional limitations and support needs of these children (22).
Alnahdi et al. (23) conducted a study that looked at family quality of life among caregivers in Saudi Arabia, which examined those caring for individuals with ASD, intellectual and other disabilities, as well as those without disabilities (23). Using the Arabic version of the Beach Center Family Quality of Life Scale, the study assessed domains including family interaction (FI), parenting practices (PP), emotional well-being (EW), physical and material well-being (PMW), and disability-related support (DRS), which could be employed to identify areas where support is most required. Significantly higher satisfaction was reported by caregivers of individuals without disabilities, particularly in emotional well-being (EW) and physical and material well-being (PMW) (23). Lower satisfaction was generally reported by fathers compared to mothers, especially in family interaction (FI) and parenting practices. EW was the most affected domain, highlighting the need for improved emotional support. Caregiving for individuals with ASD remains particularly challenging, and tailored societal and policy support is essential to reduce caregiver burden (23) (see Table 2).
The study by Al-Janabi et al. (24) examined the QoL of 248 parents of children with ASD to identify key factors affecting their well-being. The results showed that parents experience lower QoL due to psychological, financial, and social challenges. Mothers, parents with chronic conditions, and parents of female children or children with comorbidities reported significantly lower scores in health perception, mental health, and social functioning. Marital satisfaction was positively associated with most QoL domains. The authors suggest, and this is supported by several other studies, that these high-risk parent groups should be prioritized for support and interventions to improve family functioning and social support (24–27).
Emam et al. (28) studied parents of children with disabilities in Oman, Saudi Arabia, and Qatar and found that parenting stress was higher in Oman and Qatar. Parents with less support from family and friends reported lower life satisfaction. Social support was shown to buffer stress caused by parental distress, difficult child behavior, and poor parent-child interactions, thereby improving overall well-being. Fahad Manee et al. (29) compared the QoL of mothers in Kuwait who cared for children with disabilities (ASD, CP, DS, or developmental delay) with mothers of children without disabilities. Using the Arabic WHOQOL-BREF (30), it was shown that mothers of children with disabilities had significantly lower scores in all domains: physical (11.4 vs. 14.5), psychological (11.6 vs. 14.6), social (12.8 vs. 16.4), and environmental (12.4 vs. 14.8), with p < 0.001. These mothers relied mainly on their nuclear families for support because formal services were limited. It is noteworthy that occupational therapists play a key role in improving caregiver integration and access to services, which can enhance family well-being (29).
Romaniuk et al. (31) reported comparable overall family quality of life among mothers of children with ASD, ADHD, or both; however, emotional well-being was lower in mothers of children with ASD and ADHD comorbidity, indicating greater caregiving challenges. Alhammad et al. (32) found that Saudi children with Down syndrome had reduced physical, social, and school quality of life linked to impaired walking ability, despite relatively higher emotional well-being, underscoring the value of early mobility interventions (see Table 2). Additionally, migraine was shown to substantially impair daily functioning and emotional quality of life among women in Saudi Arabia, with over half experiencing severe disability, highlighting the need for improved clinical management of both disability and quality of life outcomes (33–36).
The study by Asiri et al. (37) conducted a review to examine the QoL of caregivers of children with disabilities in Saudi Arabia. The authors performed a comprehensive search of electronic databases and gray literature, which initially identified 233 studies. After applying inclusion criteria, 12 studies specifically focused on the QoL of caregivers of children with disabilities in the Saudi context. The review found that caregivers of children with disabilities have lower QoL, especially in physical, psychological, and social areas, with gender, age, and low income increasing their vulnerability. Additionally, a study comparing movement and QoL in 67 children (29 with DS, 38 typically developing) found no major differences in activity levels, though typically developing children had higher overall QoL (38). In children with DS, moderate physical activity was modestly linked to better school functioning, thereby suggesting that promoting movement can be used to improve overall outcomes.
It is evident from these studies that parental and caregiver QoL is influenced by multiple factors, including the type and severity of the child's disability, comorbid conditions, socioeconomic status, coping strategies, social and family support, mobility, and other health or environmental factors (14, 16, 18, 23, 26–28, 31, 39). EW, physical health, social participation, and access to support services were consistently identified as the most affected domains. It has been shown that adaptive coping, strong social support, early intervention programs, and policy measures to improve family resources are essential to enhance the QoL of parents and caregivers of children with disabilities in Saudi Arabia (1, 2, 8, 14, 23). These findings provide the foundation for effective planning of interventions and policies, which can alleviate multidimensional burdens and promote inclusive, supportive care systems (1, 2, 8, 14, 23).
Methodology
3
Inclusion and exclusion criteria
3.1
This review included quantitative studies that met specific inclusion and exclusion criteria. Studies were included if they focused on the QoL of parents or primary caregivers of children with disabilities in Saudi Arabia. Various disability conditions were considered, including attention-deficit/hyperactivity disorder (ADHD), cerebral palsy (CP), autism spectrum disorder (ASD), physical and sensory disabilities, intellectual and developmental disabilities, and Down syndrome (DS).
The age range of parents included in the studies was 23 years to over 57 years, while caregivers ranged from 14 to 57 years. Children included in the studies ranged in age from infancy to 18 years. Only studies that assessed QoL using validated instruments were included. These instruments comprised the WHOQOL-BREF (including its Arabic version), PedsQL 3.0 CP Module, the Beach Center Family QoL Scale, SF-36, and RAND SF-36.
Eligible studies were required to compare parental QoL across different demographic and child-related factors. Such factors included parent gender, employment status, education, housing, and type of disability. Comparisons were also made between mothers and fathers, caregivers of children with CP, ADHD, or ASD, and families with children with or without disabilities. In addition, studies examining income level, coping strategies, marital status, and experiences of discrimination were considered.
Exclusion criteria were applied to ensure the reliability of findings. Studies involving children with comorbid chronic illnesses were excluded, as these conditions could confound QoL outcomes. Intervention-based studies that evaluated the effects of treatments or programs on parental QoL were also excluded. Furthermore, only studies published in English between January 2020 and December 2024 were included to maintain consistency in language and time frame.
Search procedures
3.2
An initial search of the Cochrane Database of Systematic Reviews and PROSPERO was conducted in order to identify any existing or registered systematic reviews on the QoL of parents of children with disabilities in Saudi Arabia (17). Following this, a comprehensive literature search was carried out across multiple electronic databases, including PubMed, Scopus, Embase, Web of Science, CINAHL, ERIC, the Cochrane Library, Google Scholar, the Saudi Digital Library, and NARIC. All databases were searched using the same time limits and core eligibility filters, restricting results to studies published between January 2020 and December 2024, written in English, and involving human participants. This systematic approach was applied in order to understand the most recent evidence and to be able to capture all relevant studies within a defined time frame. It has been shown that using multiple databases, as well as being thorough in search methods, increases the likelihood that all eligible studies are identified (18).
A structured search strategy was developed, combining controlled vocabulary such as MeSH terms where applicable and free-text keywords. Boolean operators “AND” and “OR” were applied to combine search terms. The search string focused on parental and caregiver populations, different types of disabilities including autism spectrum disorder, ADHD, cerebral palsy (CP), Down syndrome (DS), and other physical disabilities, QoL outcomes, and Saudi-specific studies. Database-specific filters were applied in order to improve precision. In PubMed, filters for publication date, English language, human participants, and study type (observational and cross-sectional studies) were applied. In Scopus and Web of Science, searches were limited to peer-reviewed journal articles within health, social science, and psychology subject areas published between 2020 and 2024. Embase searches were restricted to human studies, English language, and observational study designs. CINAHL and ERIC were filtered for caregiver or parent populations, quality-of-life outcomes, English language, and the specified publication period. The Cochrane Library was searched in order to confirm the absence of prior Saudi-specific syntheses. Google Scholar was used as a supplementary source, and the first 200 results sorted by relevance were screened. In addition, the Saudi Digital Library and NARIC were searched for peer-reviewed articles matching the same keywords and publication period.
During the screening stage, additional inclusion and exclusion criteria were applied based on parental employment status (full-time, part-time, unemployed), parental and child age, and type of disability, in line with the predefined eligibility criteria. Studies examining the caregiving role and its association with parental QoL across disability types were included to inform caregiver well-being, policy, and practice. Most eligible studies were published between 2020 and 2024, with publications grouped into early (2020–2021), mid (2022–2023), and recent (2024) periods, demonstrating a clear upward trend in research activity. Reference lists were also manually screened to ensure comprehensive study identification.
Methodological quality assessment
3.3
The methodological quality of the reviewed studies was carefully assessed to ensure that the review findings are reliable and valid. A systematic evaluation process was employed to enhance transparency and maintain methodological rigor. The PRISMA 2020 guidelines (Page et al. 40) informed the assessment, as they provide a clear outline of how to report and assess the possibility of bias, supporting a consistent and reproducible review process. It is the method, which considers the quality of every study and its adherence to general methodological principles, that is used due to the necessity of reliable evidence (40).
The quality of the studies was checked with the help of predefined criteria, which is a systematic process that is currently being employed in order to make the review transparent and credible. These criteria were designed to include study design and methods, sampling strategy and sample size, validity and reliability of QoL measurement tools, appropriate application of data analysis approaches, consideration of potential confounding factors, ethical approval, clear reporting of results, and relevance to parental QoL in Saudi Arabia, allowing for a consistent assessment (19). Studies were rated as Good (high quality), Moderate (with some limitations), or Low (with major weaknesses). To reduce assessment bias, all included studies were evaluated independently by two reviewers, a process aimed at ensuring consistency and reliability. Cohen's Kappa was used to measure agreement between the reviewers, as it helps show how consistent the study quality ratings were beyond chance.
Results
4
Study selection
4.1
The Figure 2 illustrates the process of selecting studies for the systematic review. Initially, 469 records were identified from multiple databases. Before screening, 240 duplicate or repeated records were removed, leaving 229 records to be screened by title and abstract, of which 169 were excluded for not meeting the inclusion criteria. Next, 60 full-text articles were requested for review, but 7 could not be retrieved. Out of 53 full-text articles assessed for eligibility, 39 were excluded due to reasons such as disabilities caused by chronic illnesses, studies not focused on parents in Saudi Arabia, studies published before 2014, non-English articles, studies not measuring parental QoL, or those involving QoL interventions. Ultimately, 14 studies were included in the systematic review.
PRISMA diagram.
Demographic and clinical characteristics of study participants
4.2
The analysis included a total of 1,841 participants, comprising 1,090 mothers (60.18%), 418 fathers (23.08%), and 333 caregivers (18.39%), highlighting the diverse distribution of key demographic groups across the studies (41–54) (see Table 3). The age range for mothers was primarily from their early 20s to over 50 years, with most studies reporting an average age between 30 and 45 years. Similarly, the fathers' ages range from 20 to over 50 years, with most fathers being between 31 and 50 years old. The total number of children with disabilities across these studies is 1460, with common disabilities including ASD, ADHD, CP, and other physical disabilities such as stroke and amputations. The children in these studies generally range from 1 to 18 years old, with the majority falling between 1 and 5 years and 6–10 years. The studies reporting 539 people (46.4%) were employed, while 623 people (53.6%) were unemployed across the studies. Notably, the studies by Zahra et al. (47), Tedla et al. (44), Subke et al. (41), AlAhmari et al. (49), and Alhazmi et al. (54) did not explicitly mention either the employment status of caregivers or support received by families. The QoL measures used across the studies include WHOQOL-BREF, PedsQL 3.0, and RAND SF-36, among others. A variety of support from services was reported, including rehabilitation services, telehealth, special education, and government financial support, although some caregivers faced challenges related to limited access and discrimination. Comorbidities such as learning difficulties, autism, ADHD, and physical impairments were often noted in children with disabilities (see Table 2).
Measurement of QOL
4.3
The reviewed studies used different tools to measure QoL across several areas of life. The most common tool was the WHOQOL-BREF, used in 10 studies, which looks at physical, psychological, social, and environmental health. Determinants like employment, education, income, and coping strategies had a big impact on these areas. For instance, Subke et al. (41) and Tedla et al. (43) found that parents who were employed and had higher education reported better QOL, especially in physical and psychological aspects. Another tool, the Beach Center Family QOL Scale, used by Alasiri et al. (46), focused on how the family functions, including family interactions, parenting, and emotional well-being. The PedsQL 3.0 CP Module, applied in Tedla et al. (43), looked specifically at children with cerebral palsy, showing differences in mobility and age-related health outcomes. The SF-36 survey, used by Alenazi et al. (51) and Sulaimani et al. (52), measured physical functioning, role limitations, energy, emotional well-being, and pain, highlighting how caregiving and sociodemographic factors affect parents' lives. Overall, all these tools showed a similar picture: parents' quality of life is strongly influenced by caregiving duties and sociodemographic factors, with physical, psychological, and social areas being the most affected.
Quality appraisal
4.4
As part of the quality appraisal, several quality criteria were applied to systematically evaluate each study, and the results are summarized in Table 4.
Results from comparative studies
4.5
The findings below summarize the domain-specific QoL outcomes across the included studies, highlighting both positive and negative effects identified using different validated assessment instruments among caregivers and children with disabilities in Saudi Arabia (Table 5).
-
WHOQOL-BREF
-
Used in 10 of the 14 studies, making it the most frequently applied QoL instrument.
-
Nine studies reported negative outcomes in at least one domain.
-
The Physical Health (PHY) domain was most affected, with negative outcomes reported in 5 studies (50%), particularly among mothers.
-
Social Health (SOC) and Environmental Health (ENV) domains were negatively affected in 4 studies each (40%).
-
The Psychological Health (PSY) domain showed negative outcomes in 3 studies (30%).
-
SF-36 Health Survey
-
Applied in two studies: Sulaimani et al. (52) and Alenazi et al. (51).
-
Sulaimani et al. (52) reported positive outcomes in Role Emotional (RE), Mental Health (MH), Vitality/Energy-Fatigue (VT), and Social Functioning (SF).
-
In the same study, negative outcomes were observed in Bodily Pain (BP), General Health (GH), and Role Physical (RP), with no change in Physical Functioning (PF).
-
Alenazi et al. (51) reported negative outcomes in seven domains, with Bodily Pain (BP) being the only domain showing improvement.
-
Beach Center Family Quality of Life (BCFQoL) Scale
-
Positive outcomes were reported in Family Interaction (FI) and Parenting Practices (PP).
-
Negative associations were observed in Emotional Well-Being (EW), Physical/Material Well-Being (PMW), and Disability-Related Support (DRS).
-
PedsQL 3.0 Cerebral Palsy (CP) Module
-
Positive, age-related associations were found in Daily Activities (DA), School Activities (SA), and Speech/Communication (SC).
-
Negative outcomes were consistently reported in Mobility and Balance (MB), Pain/Discomfort (PH), Fatigue (FA), and Eating Activities (EA) across age groups.
Findings
5
Questions 1 and 2: results from the comparative studies
5.1
How does caregiver QOL vary by sociodemographic factors (e.g., gender, employment, education, marital status, income)?How do different disability types and severity levels affect caregiver burden and QOL?
A systematic review was conducted to summarize findings on the QoL of caregivers of children with disabilities in Saudi Arabia. It has been observed that caregiver QOL is influenced by sociodemographic factors, such as gender, employment, education, marital status, and income, as well as by the type and severity of the child's disability (see Table 5). For example:
- Alhefdhi et al. (42) found lower QOL among single and unemployed mothers. Marital status, occupation, and number of children were significant predictors. The environmental domain was most negatively affected, particularly in mothers facing economic or social challenges (p < 0.05).
- Sulaimani et al. (52) reported that educated caregivers had higher emotional well-being (53.57 vs. 33.33; p = 0.027). Caregivers of children with severe disabilities had lower bodily pain scores (58.33 vs. 80.00; p = 0.047). General health was also lower in those caring for more than one disabled child.
- Subke et al. (41) showed that employed parents had higher QOL in physical (p = 0.002), psychological (p = 0.008), and social domains (p < 0.001). Higher education and homeownership were associated with better psychological well-being (p < 0.001 and p = 0.035, respectively). Age of parent or child had no significant impact.
- Tedla et al. (44) assessed 106 female caregivers of children with CP, with an average QOL score of 66.38/100. Physical health was most affected (62.45), followed by psychological (65.44), social (72.83), and environmental domains (64.69). Significant predictors of higher QOL included child mobility (p < 0.001), caregiver education (p < 0.001), and school attendance. Socioeconomic factors, like income and housing, also contributed.
- Algadeeb et al. (48) examined caregivers of children with ADHD and reported that all QOL domains were negatively impacted, especially environmental (mean = 60.68). Most caregivers experienced moderate to high burden (86.4%), with divorced caregivers facing the highest stress (p = 0.024). Psychological and social QOL varied significantly by marital status and age (p = 0.012 and p = 0.024). Family dysfunction was common (87.4%).
Question 3: are there differences in QoL outcomes for mothers compared to other caregivers, such as fathers or extended family members?
5.2
This section examines whether QoL outcomes differ between mothers and other caregivers, including fathers and extended family members, based on evidence from the included comparative studies. Overall, most studies indicate that mothers experience poorer QoL outcomes than other caregivers.
- Ten studies using the WHOQOL-BREF reported consistent differences in QoL outcomes between mothers and other caregivers, with mothers generally reporting lower scores across multiple domains.
- For example, Subke et al. (41) conducted a cross-sectional study in Jeddah involving 200 parents of children with (ASD), where mothers accounted for 58.5% of participants and were mainly aged between 23 and 45 years. The study found that male parents reported significantly better social relationship scores than female parents, indicating lower social QoL among mothers (p = 0.002).
- Similarly, Algadeeb et al. (48) reported that mothers of children with ADHD consistently scored lower than fathers across all WHOQOL-BREF domains. Mothers had lower physical health scores (57.51 ± 20.14 vs. 62.32 ± 20.71), psychological health scores (57.12 ± 16.24 vs. 61.60 ± 13.13), and social relationship scores (57.64 ± 24.06 vs. 63.89 ± 22.83), with the largest difference observed in the social domain.
- Additionally, Alenezi et al. (50) confirmed these gender-based disparities by showing that mothers had significantly lower overall QoL scores than fathers (49.3 ± 11.8 vs. 55.6 ± 12.2; p = 0.031). The psychological health domain showed the greatest disparity, with mothers scoring 44.7 ± 10.5 compared to 50.3 ± 11.2 for fathers (p = 0.024), and this domain was strongly associated with overall QoL (r = 0.859, p < 0.01).
- In contrast, Alhefdhi et al. (42) reported no statistically significant differences in QoL between mothers and fathers (p = 0.833). Although mothers showed slightly higher physical and psychological scores and fathers had marginally higher environmental scores, these differences did not reach statistical significance.
- Furthermore, using the SF-36 questionnaire, Sulaimani et al. (52) observed notable emotional well-being differences among caregivers. Mothers scored lower (mean ± SD: 60.33 ± 20.31) compared to siblings such as brothers (mean ± SD: 74.00 ± 8.49; p = 0.023), highlighting the heightened emotional burden experienced by mothers as primary caregivers. These findings are consistent with broader literature indicating that mothers, as the primary caregivers, often face greater emotional and caregiving burdens than other family members. Their responsibilities typically encompass daily care management, coordinating medical appointments, and providing emotional support, all while balancing household and occupational roles. The cumulative effect of these duties likely contributes to the consistently lower emotional well-being scores observed among mothers (55–59).
Research 4: which quality of life domains (e.g., physical, psychological, social, environmental) are affected most?
5.3
To answer the fourth research question, the results show that QoL affects caregivers in different ways across several areas. Physical health was one of the most challenging areas, especially for caregivers looking after children with severe disabilities or limited mobility. Many caregivers reported feeling physically exhausted and experiencing health problems due to the constant demands of caregiving [Tedla et al. (43), Sulaimani et al. 52]. Psychological well-being was also strongly affected, with caregivers reporting high levels of stress, anxiety, and depression. Mothers and caregivers who relied on poor coping strategies were particularly vulnerable and reported lower psychological QoL [Alenezi et al. (50), Subke et al. 41]. Social relationships were another area of difficulty, as many caregivers felt isolated and disconnected from others. However, those who took part in support groups reported better social QoL because these groups helped them feel more connected and less alone [Alhazmi et al. (54), Al Awaji et al. 53]. Environmental QoL was closely linked to practical factors such as housing, safety, and access to services. Caregivers with better financial stability and access to resources tended to report better outcomes in this area (Alhazmi et al. (54), Zahra et al. (47). Overall, these findings show that caregivers face different challenges across multiple areas of quality of life, rather than in just one single domain (see Table 5).
Research question 5: how do social and governmental support systems (such as rehabilitation services and financial aid) affect the QoL of parents of children with disabilities in Saudi Arabia?
5.4
Social and governmental support systems, such as rehabilitation services and financial aid, significantly enhance the QoL for parents of children with disabilities in Saudi Arabia. Parents who received access to rehabilitation services reported better QoL. For example, Tedla et al. (43) noted that caregivers of children with CP benefited from rehabilitation and special education services, which contributed positively to their QoL. Financial support was shown to significantly alleviate stress. In Tedla et al. (44), 55.7% of caregivers received government financial support, which correlated with improved QoL measures. Alhazmi et al. (54) also highlighted the role of financial stability, often enabled by employment or subsidies, in improving caregivers' QoL across multiple domains. Although the Saudi government provides funds and access to rehabilitation centers [Al Awaji et al. (53)], gaps remain in the accessibility and availability of services, particularly during lockdowns or crises, reducing the potential benefits for caregivers. AlAhmari et al. (49) emphasized limited healthcare access and social integration gaps, negatively impacting caregivers' QoL. Speech and behavioral therapy, as noted by Alasiri et al. (46), were crucial for parents of children with autism, leading to enhanced family satisfaction.
Discussion
6
It is noteworthy that, in this systematic review, the QoL of parents and caregivers of children with disabilities in Saudi Arabia has been shown to be influenced by a combination of sociodemographic, contextual, and structural factors (14, 23, 24, 26, 31, 41, 52). There has been a growing interest in caregiver well-being, particularly in relation to long-term caregiving responsibilities; therefore, the available evidence was reviewed and summarized in order to understand how these factors are associated with caregiver QoL and to what extent such associations are evident. Across the included studies, higher levels of employment, income, and educational attainment were found to be consistently associated with better QoL outcomes (24, 26, 37, 48, 49, 54). In addition, differences across physical, psychological, social, and environmental QoL domains were observed to be associated with caregiver gender and marital status. These patterns have also been reported in international literature, in which socioeconomic position has been identified as a key determinant of caregiver well-being and the unequal distribution of caregiving burden across populations has been highlighted (10, 13, 27–29).
The reduction in parental QoL that has been reported is associated with the continuous and demanding role of caring for a child with long-term health or developmental conditions (26, 28, 29, 41, 52). Emotional, physical, and financial strain is often experienced by caregivers, which can build up over time and thereby lead to chronic stress. Studies have shown that mothers, who are more often the primary caregivers, are particularly vulnerable and more likely to report higher psychological distress (14, 23, 26, 31, 53). This is particularly significant, as increased anxiety, depression, and parent–child strain has been recorded in families of children with special needs in comparison with families of typically developing children (55, 56). Despite these challenges, caregiving experiences are not only variable but also affected by the availability of social support and access to services, which can be used to reduce negative outcomes. However, social stigma and discrimination have been reported among families of children with intellectual disabilities or autism, with cultural norms shaping how stress is experienced and expressed, thereby further impacting QoL outcomes (57, 58). In the context of these findings, it becomes clear that caregiving stress is caused not only by the child's condition but also by social and environmental factors, which must be addressed for better parental well-being. More recently, it has been suggested that programs offering social, emotional, and educational support could thus help improve parental QoL (10, 14, 28, 52).
Related to that, international evidence has provided important comparative perspectives, which can be used to contextualize the Saudi findings (10, 27–30). This body of research has examined caregiver QoL across different sociocultural and economic settings and has assessed how it is shaped in response to variations in support systems (10, 13, 27–29). For example, in the study by Xia et al. (59), which examined caregivers of children with disabilities in China, anxiety and depression were reported in 33.6% and 36.1% of caregivers, respectively. It was shown that mental health-related QoL was improved through psychological and financial support; however, physical QoL was not significantly affected. Rehabilitation services and financial assistance were identified as the most needed forms of support, particularly among parents and grandparents. Similarly, in the study by Scheibner et al. (60), parenting stress among German caregivers was analysed, and significantly higher stress levels were reported among mothers and single parents compared with fathers and two-parent families. Stress was shown to be highest during children's early school years and was associated with employment type, as part-time employment was linked to higher stress levels compared with unemployment or full-time employment. In the Malaysian context, QoL among caregivers was assessed by Ismail et al. (61), and it was found that low-income families and those caring for children with comorbidities or feeding difficulties were the most adversely affected. While psychological well-being (68.98) and social relationships (75.15) were reported to score relatively higher, environmental support (64.61) was more limited, indicating that financial strain and restricted resources contributed to poorer QoL. Taken together, these studies have demonstrated that targeted and context-specific support systems are essential for reducing caregiver burden and improving QoL outcomes (61).
Child-related factors have also been shown to play an important role in affecting caregiver QoL, especially depending on the type and severity of the child's disability. This association has been supported by several previous studies (6, 15, 16, 21, 22, 25, 31, 43, 44, 46). In a review by Isa et al. (62), which looked at caregivers of children with ASD, ADHD, and CP, it was shown that ASD is associated with very high caregiving demands. Children with ASD were reported to need constant supervision and special support, thereby increasing emotional strain and the effort of caregiving. As a result, sleep problems, financial pressure, and social isolation were often reported by caregivers. These challenges were further increased by the need to manage behavioural and social difficulties related to ASD, making daily caregiving especially demanding. Caring for children with ADHD was also shown to lower caregiver QoL, as hyperactivity, impulsivity, and attention difficulties must be managed continuously at home and school, which can cause ongoing stress, tiredness, and family conflicts (63, 64). In addition, children with physical disabilities were found to depend heavily on caregivers for moving around, personal care, and medical support, which can be physically tiring. The extra time and cost for therapy sessions, medications, special education, and assistive devices were shown to further increase caregiver strain and lower overall QoL (62). This is particularly significant, as these challenges must be addressed to improve caregiver well-being. In the context of these findings, it becomes clear that child-related characteristics are not only a key cause of caregiver stress but also show areas where support programs could be used to improve QoL (62).
These findings matter for Saudi Vision 2030, which focuses on improving health and social care (1, 2, 5, 7, 8). While most programs target children, supporting caregivers is essential for better care outcomes (14, 23, 31, 44, 52). As noted by Alharbi et al. (65), Vision 2030 includes grants, subsidies, universal healthcare, and education reforms, which are designed to reduce psychological, economic, and social burdens on families. However, gaps in service availability and poor coordination across health, education, and social sectors must be addressed to improve caregiver QoL fairly across the country. Following this, practical strategies could be used, such as adding caregiver well-being checks in paediatric and rehabilitation services, expanding community rehabilitation programs, improving financial support, and increasing peer-support as well as respite care. In this context, it becomes clear that supporting caregivers is particularly significant, enabling better outcomes for both children and families and helping achieve the goals of Vision 2030 (65).
Strengths and limitations
6.1
The strengths of this study include its systematic and comprehensive approach, following PRISMA guidelines to synthesize evidence from multiple Saudi-based studies published between 2020 and 2024, which enhances methodological rigor and transparency (40). The inclusion of diverse childhood disabilities and the use of validated QoL instruments allow for meaningful comparisons across different caregiver groups and life domains. Additionally, by focusing specifically on the Saudi context, this review fills an important research gap and provides culturally relevant insights (1, 3, 65), while identifying key vulnerable groups and highlighting the role of support services, making the findings highly relevant for healthcare policy, family support planning, and future research (8, 14, 52).
Despite these strengths, several limitations must be addressed for proper interpretation of the findings. Most importantly, cross-sectional designs were employed in all included studies, which restricts causal relationships between caregiving factors and parental QoL from being inferred (16, 27, 62). It is straightforward that assessment of how caregiver QoL evolves over time or in response to changes in disability severity, service access, or policy interventions is prevented by the lack of longitudinal evidence, which must be addressed in future research (30, 55). When these changes are considered, it becomes evident that causal links cannot be established.
QoL outcomes were predominantly based on self-reported measures, which can be influenced by recall bias, response bias, and social desirability effects (55, 56). Cultural norms within Saudi society may further affect how psychological distress or social challenges are reported by caregivers, which may have led to under- or overestimation of certain QoL domains. This is particularly significant, as uncertainty in the reported outcomes could thereby be increased (59).
A clear gender imbalance was observed, with mothers comprising the majority of participants, which is one challenge in the included studies. While real-world caregiving patterns are reflected, generalizable findings for fathers and other caregivers are not always obtained, thereby restricting deeper gender-comparative analyses (31, 60). Following this, it becomes apparent that gender differences in caregiver QoL should be explored in future research in order to understand the full scope of caregiving experiences and to what extent these experiences vary by caregiver type (23, 28).
Methodological heterogeneity, which included differences in QoL instruments, reporting formats, and domain-level analyses, limited direct comparability and precluded quantitative meta-analysis (27, 30, 40). Convenience sampling from single regions or clinical settings was used in several studies, which reduced national representativeness and limited insights into rural or underserved populations. It was shown that observed patterns of caregiver QoL could thereby be influenced, which must be considered when interpreting the results. Finally, some studies lacked detailed diagnoses or comorbidity data, which may have affected caregiver QoL and should be addressed in future research (16, 43, 44).
Challenges and future directions
6.2
The QoL of parents caring for children with disabilities in Saudi Arabia is affected by several ongoing challenges. Services are not evenly distributed, with families in urban areas having better access than those in rural regions, especially for specialized therapies such as speech and language services (23, 66). Financial support often does not fully cover the high cost of care and long-term therapy, which places added stress on families. There is also a shortage of trained professionals and specialized centers, making it harder for families to receive consistent and high-quality support (65, 66). Cultural attitudes toward disability can further increase emotional strain and limit social participation for caregivers. Looking ahead, future efforts should focus on improving access to services across all regions, expanding training programs to build a skilled workforce, and strengthening community-based rehabilitation services to better support families and improve caregiver QoL.
Conclusion
7
This review shows that taking care of a child with a disability lowers the QoL of parents and caregivers in Saudi Arabia. It was found that physical, mental, social, and environmental well-being are all affected. Mothers are the most affected because they are the main caregivers and often have lower scores than fathers. More than half of caregivers do not have a job, and poor quality of life is linked to unemployment, low income, less education, and little support. Caring for children with severe or multiple disabilities increases stress and burden. Physical health is the most affected, followed by social and environmental life, and mental stress is common. Some support services exist, but they are not always enough or easy to access. This shows that social and financial problems make life harder for caregivers. It is important to provide more financial help, better access to rehabilitation and mental health services, and special support for mothers and disadvantaged families to improve caregivers' quality of life in Saudi Arabia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malik S Shrahili M Khan SU. The transformation to reduce the disability prevalence rates in Saudi Arabia: a theoretical analysis. J Disabil Res. (2024) 3(3):20240024. 10.57197/JDR-2024-0024 · doi ↗
- 2Yousef L Almatroodi N Al Angari D Al Shehri R Alshammari S. Disability inclusion assessment in primary healthcare centers in eastern Saudi Arabia: a way forward. J Med Life. (2023) 16(12):1813. 10.25122/jml-2023-038538585520 PMC 10994619 · doi ↗ · pubmed ↗
- 3Alghadier M Albesher RA Basoudan R. Bibliometric analysis of scientific research on children’s disability in Saudi Arabia. J Disabil Res. (2024) 3(6):20240068. 10.57197/JDR-2024-0068 · doi ↗
- 4Almalki NS Arrushaid OM Farah Bakhiet S Alkathiri S. Examining the current practices of the individualized family services plan with young children with disabilities in Saudi Arabia. Int J Dev Disabil. (2023) 69(2):163–78. 10.1080/20473869.2021.193684937025331 PMC 10071896 · doi ↗ · pubmed ↗
- 5General Authority for Statistics, Kingdom of Saudi Arabia. General Authority for Statistics (2025). Available online at: https://www.stats.gov.sa/ (Accessed January 15, 2025).
- 6Alarifi S Denne L Hastings RP. Challenging behaviour and its correlates in preschool-aged children with an intellectual disability in Saudi Arabia. J Intellect Disabil Res. (2024) 68(3):264–76. 10.1111/jir.1310938052235 · doi ↗ · pubmed ↗
- 7Abed MG Abed LG Shackelford TK. A qualitative, small-sample study of employment challenges for people with disabilities in Saudi Arabia. Healthcare (Basel). (2024) 12(3):346.38338230 10.3390/healthcare 12030346 PMC 10855392 · doi ↗ · pubmed ↗
- 8Medabesh AM Malik NN Shafi M Rashid J. Strategies for facilitating social integration of children with disabilities in Saudi Arabia. J Disabil Res. (2024) 3(7):20240089. 10.57197/JDR-2024-0089 · doi ↗