Outcomes of Fluoroscopy-Free Percutaneous Intrafocal Pinning for Adult Distal Radius Fractures in a Resource-Limited Setting in South Kivu, Democratic Republic of the Congo
Rodrigue Mupenda Mwenibamba, Daniel S Nteranya, Christian B Wabene, Alexandre N Nakashenyi, Eben Ezer Genda, Fabrice Kibukila, Didier M Kasilembo, Desire A Munyali, Severin M Kavatsura, Zacharie T Kibendelwa, Uwonda Akinja, Tshimbila Kabangu

TL;DR
This study shows that a technique for fixing wrist fractures without X-ray imaging works well in a low-resource area of the Democratic Republic of the Congo.
Contribution
The study demonstrates the effectiveness of fluoroscopy-free treatment for wrist fractures in resource-limited settings.
Findings
Most patients had excellent or good outcomes in terms of anatomy, radiology, and function.
Complications were rare and included infections, pin migration, and nerve injuries.
Longer rehabilitation and hospitalization were linked to worse outcomes.
Abstract
Purpose: To assess the anatomical, radiological, and functional outcomes of fluoroscopy-free percutaneous intrafocal pinning for distal radius fractures in adults in resource-constrained settings of South Kivu, Democratic Republic of Congo. Methods: In a prospective, multicenter, interventional study, 101 adults with distal radius fractures were treated from January 2018 to December 2023 across four hospitals. Fractures were reduced using external maneuvers and stabilized with three-pin percutaneous intrafocal pinning without fluoroscopy. Outcomes were evaluated using the Grumillier Criteria and modified Castaing classification, with a minimum six-month follow-up. Data analysis with R software (R Foundation for Statistical Computing, Vienna, Austria) included descriptive statistics, principal component analysis, and factorial analysis. Results: Patients had a mean age of 36.41 ± 12.61…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
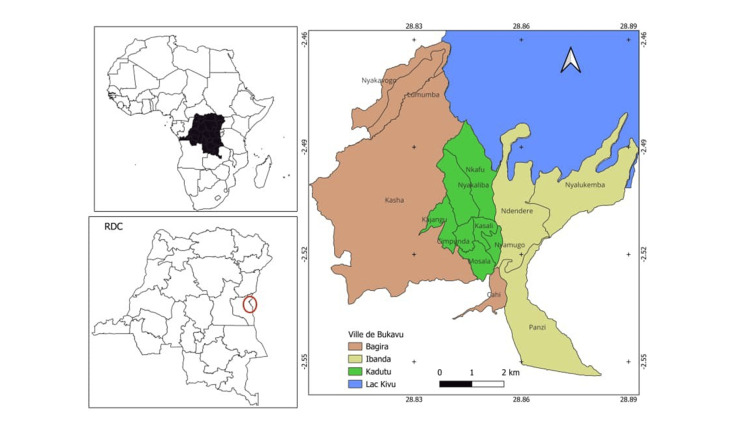 Figure 1
Figure 1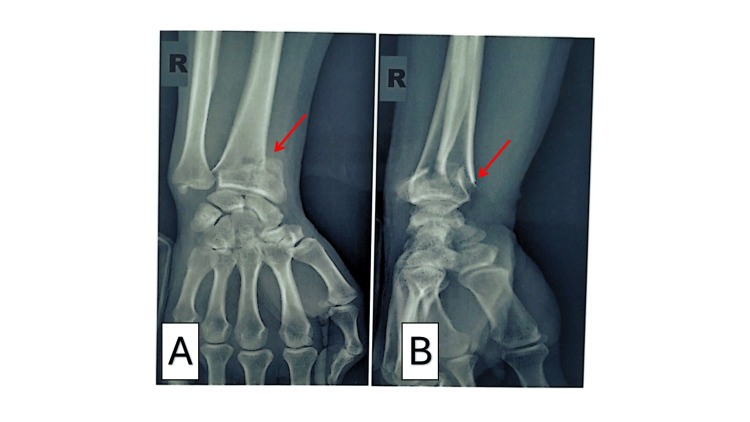 Figure 2
Figure 2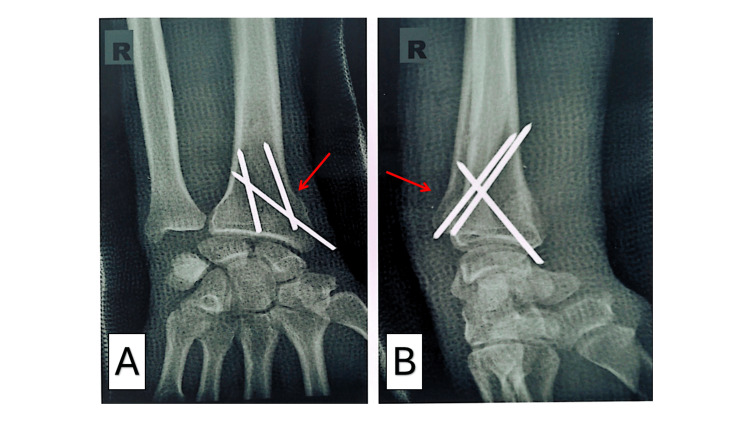 Figure 3
Figure 3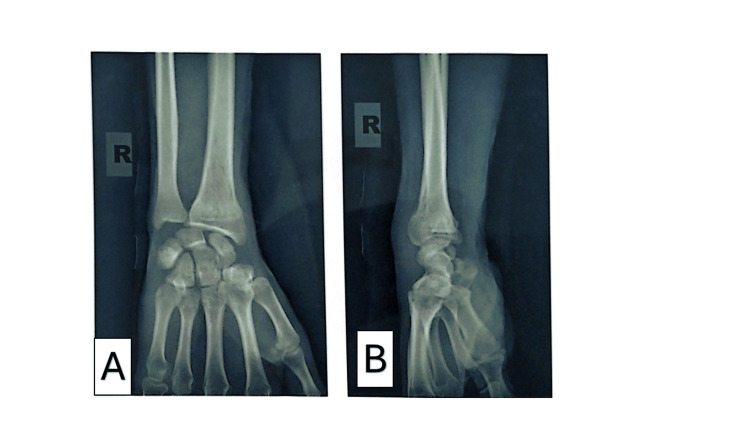 Figure 4
Figure 4| Characteristic | Value |
| Age (years) | |
| Minimum | 18 |
| Maximum | 70 |
| Mean ± SD | 36.41 ± 12.61 |
| Age range (years) | n (%) |
| 18-27 | 31 (30.69) |
| 28-37 | 23 (22.77) |
| 38-47 | 27 (26.73) |
| 48-57 | 13 (12.87) |
| 58-67 | 6 (5.94) |
| 68-77 | 1 (0.99) |
| Gender | |
| Male | 69 (68.32) |
| Female | 32 (31.68) |
| Profession | |
| Civil servant | 37 (36.63) |
| Student | 13 (12.87) |
| Retailer | 12 (11.88) |
| Teacher | 9 (8.91) |
| Housekeeper | 9 (8.91) |
| Bricklayer | 4 (3.96) |
| Player | 4 (3.96) |
| Sports | 4 (3.96) |
| Driver | 3 (2.97) |
| Motorcyclist | 1 (0.99) |
| ANR agent | 1 (0.99) |
| None | 4 (3.96) |
| Origin | |
| Urban | 79 (78.22) |
| Rural | 20 (19.80) |
| Foreign | 2 (1.98) |
| Characteristic | Category | n (%) |
| Mechanism of injury | Road traffic accident | 36 (35.64) |
| Fall from height | 32 (31.68) | |
| Sports injury | 16 (15.84) | |
| Fall from high place | 6 (5.94) | |
| Domestic injury | 3 (2.97) | |
| Occupational injury | 3 (2.97) | |
| Slip | 3 (2.97) | |
| Assault | 1 (0.99) | |
| Other traffic injury | 1 (0.99) | |
| Affected side | Right | 54 (53.47) |
| Left | 46 (45.54) | |
| Bilateral | 1 (0.99) | |
| Medical history | None | 84 (83.17) |
| Diabetes mellitus | 6 (5.94) | |
| Osteoporosis | 3 (2.97) | |
| Hypertension | 2 (1.98) | |
| Osteoporosis and hypertension | 2 (1.98) | |
| Osteoporosis, hypertension, sickle cell disease | 2 (1.98) | |
| Menopause | 1 (0.99) | |
| Osteoporosis, diabetes, hypertension | 1 (0.99) | |
| Castaing classification | Type I | 93 (92.08) |
| Type II | 3 (2.97) | |
| Type III | 1 (0.99) | |
| Type IV | 3 (2.97) | |
| Type VIII | 1 (0.99) |
| Characteristic | Category | n (%) |
| Preoperative delay (days) | 1 | 69 (68.32) |
| 2 | 30 (29.70) | |
| 3 | 2 (1.98) | |
| Mean ± SD | 1.34 ± 0.52 | |
| Range | 1-3 | |
| Surgical technique | External reduction | 101 (100.00) |
| Arm tourniquet | 101 (100.00) | |
| Percutaneous intrafocal pinning | 101 (100.00) | |
| Number of pins: Three | 101 (100.00) | |
| Image intensifier: None | 101 (100.00) | |
| Postoperative immobilization | Immobilization: Yes | 101 (100.00) |
| Type: Antebrachio-palmar cast | 101 (100.00) | |
| Type: Brachio-antebrachio-palmar cast | 0 (0.00) | |
| Postoperative radiographic results | Excellent | 49 (48.51) |
| Very good | 35 (34.65) | |
| Good | 13 (12.87) | |
| Fair | 3 (2.97) | |
| Poor (required surgical revision) | 1 (0.99) |
| Characteristic | Category | n (%) or Value |
| Length of hospital stay (days) | 1 | 1 (0.99) |
| 2 | 6 (5.94) | |
| 3 | 49 (48.51) | |
| 4 | 19 (18.81) | |
| 5 | 19 (18.81) | |
| 6 | 6 (5.94) | |
| 7 | 1 (0.99) | |
| Mean ± SD | 3.70 ± 1.12 | |
| Range | 1-7 | |
| Time to consolidation (days) | 44 | 3 (2.97) |
| 45 | 74 (73.27) | |
| 46 | 6 (5.94) | |
| 47 | 1 (0.99) | |
| 48 | 3 (2.97) | |
| 49 | 1 (0.99) | |
| 50 | 3 (2.97) | |
| 60 | 10 (9.90) | |
| Mean ± SD | 46.82 ± 4.67 | |
| Range | 44-60 | |
| Time to removal of pins and cast (days) | Mean ± SD | 50.67 ± 6.01 |
| Range | 45-60 | |
| Last postoperative follow-up (months) | 9 | 7 (6.93) |
| 10 | 1 (0.99) | |
| 12 | 9 (8.91) | |
| 16 | 4 (3.96) | |
| 18 | 9 (8.91) | |
| 20 | 1 (0.99) | |
| 22 | 2 (1.98) | |
| 24 | 18 (17.82) | |
| 28 | 6 (5.94) | |
| 30 | 8 (7.92) | |
| 32 | 9 (8.91) | |
| 36 | 11 (10.89) | |
| 39 | 1 (0.99) | |
| 46 | 4 (3.96) | |
| 48 | 8 (7.92) | |
| 49 | 1 (0.99) | |
| 50 | 1 (0.99) | |
| 53 | 1 (0.99) | |
| Mean ± SD | 27.27 ± 11.85 | |
| Range | 9-53 |
| Characteristic | Category | n (%) or Value |
| Postoperative complications | Superficial infection | 3 (2.97) |
| Pin migration | 2 (1.98) | |
| Complex regional pain syndrome | 2 (1.98) | |
| Malunion | 3 (2.97) | |
| Twisted pin | 1 (0.99) | |
| Radial sensory nerve injury | 1 (0.99) | |
| Extensor pollicis longus tendon injury | 1 (0.99) | |
| Wounds | 0 (0.00) | |
| Delayed consolidation | 0 (0.00) | |
| Nonunion | 0 (0.00) | |
| Osteoarthritis | 0 (0.00) | |
| Rehabilitation sessions | 10 | 1 (0.99) |
| 13 | 1 (0.99) | |
| 14 | 3 (2.97) | |
| 15 | 24 (23.76) | |
| 16 | 15 (14.85) | |
| 17 | 8 (7.92) | |
| 18 | 18 (17.82) | |
| 19 | 3 (2.97) | |
| 20 | 17 (16.83) | |
| 21 | 2 (1.98) | |
| 22 | 3 (2.97) | |
| 25 | 4 (3.96) | |
| 30 | 2 (1.98) | |
| Mean ± SD | 17.72 ± 3.22 | |
| Range | 10–30 | |
| Removal of pins and cast (days) | 45 | 26 (25.74) |
| 46 | 8 (7.92) | |
| 47 | 4 (3.96) | |
| 48 | 17 (16.83) | |
| 49 | 4 (3.96) | |
| 50 | 15 (14.85) | |
| 52 | 1 (0.99) | |
| 55 | 1 (0.99) | |
| 59 | 1 (0.99) | |
| 60 | 24 (23.76) | |
| Mean ± SD | 50.67 ± 6.01 | |
| Range | 45–60 | |
| Outcome scores | ||
| Subjective score | Very good | 85 (84.16) |
| Good | 10 (9.90) | |
| Fair | 6 (5.94) | |
| Objective score | Very good | 78 (77.23) |
| Good | 17 (16.83) | |
| Fair | 4 (3.96) | |
| Poor | 2 (1.98) | |
| Radiological score (Castaing) | Very good | 76 (75.25) |
| Good | 20 (19.80) | |
| Fair | 5 (4.95) | |
| Socio-professional reintegration | Yes | 91 (90.10) |
| No | 1 (0.99) | |
| Unemployed/retired | 9 (8.91) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Elbow and Forearm Trauma Treatment · Facial Trauma and Fracture Management
Introduction
Distal radius fractures are among the most common injuries seen in emergency departments [1,2] and consume considerable healthcare resources [3]. Their management is challenging due to marked anatomical and clinical variability and the absence of a universally superior treatment method [4,5]. Current guidelines recommend surgical treatment for young, active patients and for fractures that, after closed reduction, still show >3 mm radial shortening, >10° dorsal tilt, or >2 mm intra-articular step-off [6,7]. In higher-demand patients meeting these criteria, surgery yields better radiological and functional outcomes than conservative management [8]. The two most common surgical options are percutaneous K-wire fixation and volar locking plate (VLP) osteosynthesis. Both techniques provide satisfactory long-term results; VLP offers faster short-term recovery and superior anatomical restoration, whereas functional outcomes become comparable after one year [9]. Intrafocal (Kapandji) pinning, first described in 1987 [10], is a minimally invasive and cost-effective K-wire technique that provides three-point buttressing inside the fracture site, prevents secondary displacement, and eliminates the need for prolonged immobilization [11]. It is traditionally performed under fluoroscopic control to ensure accurate reduction and safe implant positioning. However, intraoperative radiation exposure, even with modern mini C-arms, carries documented risks of malignancy, chronic radiation dermatitis, and cataracts for patients and surgical staff [12-14]. In many low- and middle-income countries, particularly in sub-Saharan Africa, fluoroscopy remains unavailable in most trauma centers [15]. Consequently, distal radius fractures are frequently treated non-operatively or with “blind” Kapandji-type pinning. The Democratic Republic of Congo is no exception. We therefore conducted a single-arm prospective interventional cohort without a comparator to evaluate the anatomical, radiological, and functional outcomes of fluoroscopy-free percutaneous intrafocal (Kapandji) pinning in adults with distal radius fractures in order to determine its safety and effectiveness in resource-constrained environments.
Materials and methods
Study design
This is a single-arm prospective interventional multicenter cohort study without a comparator that analyzed 101 consecutive cases of distal radius fractures in adults treated with fluoroscopy-free percutaneous intrafocal pinning, conducted from January 1, 2018, to December 31, 2023.
Patient recruitment
The study included patients treated at Cliniques Universitaires de Bukavu, Skyborne Hospital, Clinique Saint-Luc Mbaki, and Centre Hospitalier Medicure in South Kivu, Democratic Republic of Congo (Figure 1).
Map of Bukavu town highlighting the area covered by the studyBukavu town comprises three health zones: Bagira, Ibanda, and Kadutu. These zones are highlighted on the map using different colors.Image Credit: The image was created by the author using QGIS software (version 3.40.12; https://qgis.org/project/overview/).
Inclusion criteria comprised patients aged ≥17 years with distal radius fractures managed by percutaneous intrafocal pinning without an image intensifier, complete medical records, and a minimum follow-up of six months for clinical and radiological evaluation. Patients with incomplete records or follow-up less than six months were excluded.
Data collection and outcome assessment
Data were collected using a standardized form, extracting information from medical records, consultation registries, hospital databases, and operative reports. Fractures were classified using the modified Castaing classification as described by Kapandji. Postoperative outcomes were evaluated using the Grumillier criteria (subjective, objective, and radiological), as reported by the Groupe d’Étude de la Chirurgie Orthopédique (GECO) group.
Sample size
The study employed a consecutive sampling method, enrolling all eligible patients presenting to the emergency department of Cliniques Universitaires de Bukavu, Skyborne Hospital, Clinique Saint-Luc Mbaki, and Centre Hospitalier Medicure in South Kivu, between January 1, 2018, and December 31, 2023, resulting in a sample size of 101 participants, determined based on the study period and inclusion criteria.
Statistical analysis
Data were entered into Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and analyzed using R software (version 4.4.3, R Foundation for Statistical Computing, Vienna, Austria). Statistical analyses included descriptive statistics (mean, standard deviation, minimum, maximum) for frequency and outcome distribution. Contingency tables were examined using principal component analysis (PCA) and mixed-data factorial analysis to explore relationships between variables.
Surgical technique
The procedure was performed under general or locoregional anesthesia with the patient in dorsal decubitus and the upper limb positioned on an arm table, with or without a pneumatic tourniquet. No image intensifier was used. Fracture reduction was achieved through external maneuvers, including axial thumb traction, wrist flexion, and ulnar tilt. The fracture site was identified by digital palpation of the fragments using the operator’s thumb. Reduction quality was assessed by restoration of the bi-styloid line, radial anatomical axis, and correction of epiphyseal fragment deformity. Three percutaneous pins (18/10 or 20/10 mm, 30 cm long, cut into three segments) were inserted intrafocally: a dorsolateral pin along the second radius axis, a lateral pin along the first radius axis, and a dorsomedial pin along the third radius axis. Anatomical landmarks guided pin placement, with the lateral radial edge used for the lateral pin and the axes of the second and third for the dorsolateral and dorsomedial pins, respectively. Pins were cut flush and buried subcutaneously.
Postoperatively, an antebrachio-palmar cast was applied for 45 days. Pin removal occurred at 45 days. Patients initiated self-rehabilitation on postoperative day 1, performing isometric contractions of wrist and finger extensors/flexors and active finger mobilization. Physiotherapist-guided rehabilitation commenced after cast and pin removal to optimize functional recovery.
Ethical considerations
This study was approved by the Medical Ethics Committee of the Official University of Bukavu, Bukavu, Democratic Republic of Congo (Approval No. UOB/CEM/037/2023). Written informed consent was obtained from all participants for both treatment and the use of their data in this research, in accordance with the Declaration of Helsinki and institutional ethical guidelines.
Results
The cohort included 101 patients with a mean age of 36.41 ± 12.61 years (range: 18-70 years). Males accounted for 68.32% (n = 69). Civil servants were the most affected occupational group (n = 37, 36.63%), followed by students (n = 13, 12.87%) and shopkeepers (n = 12, 11.88%). Urban residents comprised 78.22% (n = 79) of cases, with 19.80% (n = 20) from rural areas (Table 1).
Clinical and radiological characteristics
Comorbidities were diabetes (n = 6, 5.94%) and osteoporosis (n = 3, 2.97%); 83.17% (n = 84) had no relevant medical history. Primary injury mechanisms were road traffic accidents (n = 36, 35.64%) and falls from height onto the hand (n = 32, 31.68%). The right wrist was involved in 53.47% (n = 54) and the left in 45.54% (n = 46). Per the modified Castaing classification, type I fractures (Figure 2) dominated (n = 93, 92.08%), followed by types 2 and 4 (n = 3 each, 2.97%) (Table 2).
Anteroposterior (A) and lateral (B) radiographs of the forearm showing a distal radial fracture in a 33-year-old male patient following a fallA (anteroposterior view) and B (lateral view) demonstrate plain radiographs of the wrist. There is a compaction/impaction fracture of the distal radius characterized by cortical buckling and increased radiopacity (sclerosis) at the metaphyseal region, best appreciated on the lateral projection (Figure B, red arrow). Subtle disruption of the dorsal cortical margin with mild dorsal angulation of the distal fragment is noted, consistent with a compression-type distal radius fracture (Colles’ type pattern). No intra-articular extension seen; an associated ulnar styloid fracture is evident in the provided views.
Perioperative details
All fractures underwent fluoroscopy-free percutaneous intrafocal pinning with three pins inserted via mini-incisions (posterolateral, lateral, and posteromedial, aligned with the second, first, and third ray axes, respectively) following reduction by external maneuvers (Figure 3). One patient required reintervention. The mean preoperative delay was 1.34 ± 0.52 days (range: 1-3 days), with 68.32% (n = 69) treated within 24 hours. General anesthesia and an arm tourniquet were universal, with patients positioned in dorsal decubitus. Postoperative radiographs (Figure 4) showed excellent alignment in 48.51% (n = 49), very good in 34.65% (n = 35), and good in 12.87% (n = 13). All patients received an antebrachio-palmar cast for 45 days (Table 3).
Postoperative anteroposterior (A) and lateral (B) radiographs showing reduction and osteosynthesis of the distal radius fracture using three pins placed with a freehand techniqueA (anteroposterior view) and B (lateral view) show postoperative plain radiographs of the wrist following closed reduction and percutaneous pinning of a distal radius compression fracture. The original injury was an extra-articular compaction/impaction fracture with dorsal cortical buckling and mild dorsal angulation of the distal fragment (Colles’ type pattern). Post-reduction alignment is restored with anatomical radial height, inclination, and near-neutral tilt. Fracture stability is achieved using three smooth percutaneous Kirschner wires (K-wires):Two parallel radial styloid pins were inserted from the dorsal-ulnar aspect of the styloid, engaging the opposite intact cortex (clearly visible in Figure A).One dorsoulnar pin crosses the fracture site obliquely, providing three-point fixation and buttressing the dorsal comminution (best seen in Figure B).The pins maintain fracture reduction without loss of position. No intra-articular penetration is observed. The configuration effectively neutralizes compressive and bending forces, ensuring stable fixation during healing.
Radiograph of the same patient demonstrating a well-consolidated fracture 47 days after removal of the Kirschner wires (K-wires)A (anteroposterior view) and B (lateral view) are follow-up plain radiographs of the wrist obtained after removal of percutaneous K-wires, approximately seven weeks following closed reduction and pinning of an extra-articular distal radius compression fracture (Colles’ type). The fracture is fully consolidated with complete bony union across the metaphyseal region. Previous impaction and dorsal cortical buckling have remodeled, showing restoration of normal trabecular architecture and smooth cortical contours. Radial height, radial inclination, and volar tilt are anatomically restored with no residual angulation or displacement. The pin tracks are barely visible and show no signs of infection or osteolysis. There is no evidence of post-traumatic arthritis or secondary displacement. The radiographs confirm solid healing and excellent functional outcome.
Postoperative outcomes and complications
Mean hospital stay was 3.70 ± 1.12 days (range: 1-7 days), with 48.51% (n = 49) discharged after three days. Fracture consolidation occurred at a mean of 46.82 ± 4.67 days (range: 44-60 days), with 73.27% (n = 74) consolidating by 45 days. Pins and casts were removed at 50.67 ± 6.01 days (range: 45-60 days). Rehabilitation averaged 17.72 ± 3.22 sessions (range: 10-30), with 23.76% (n = 24) requiring 15 sessions. Complications included superficial infections (n = 3, 2.97%), malunion (n = 3, 2.97%), pin migration (n = 2, 1.98%), complex regional pain syndrome (n = 1, 0.99%), twisted pin (n = 1, 0.99%), radial sensory nerve injury (n = 1, 0.99%), and extensor pollicis longus tendon injury (n = 1, 0.99%) (Table 4).
Functional and radiological results
At a mean follow-up of 27.27 ± 11.85 months (range: 9-53 months), Grumillier criteria outcomes were subjective scores - very good in 84.16% (n = 85) and good in 9.90% (n = 10); objective scores - very good in 77.23% (n = 78) and good in 16.83% (n = 17); and radiological scores (Castaing) - very good in 75.25% (n = 76) and good in 19.80% (n = 20) (Table 5).
Statistical insights
Principal component analysis (PCA) indicated that prolonged rehabilitation correlated with worse subjective and objective scores, while better scores showed a negative correlation. Castaing fracture types were inversely correlated with outcomes, with type I fractures achieving superior results compared to types 4 and 8. Extended hospital stays were associated with poorer objective scores and inversely related to better scores. Factorial analysis with mixed data confirmed that poor objective scores predicted failed socio-professional reintegration. Age and gender did not influence outcomes across subjective, objective, or radiological domains.
Discussion
This study demonstrates the efficacy of fluoroscopy-free percutaneous intrafocal pinning for distal radius fractures in a resource-limited setting, yielding excellent anatomical, radiological, and functional outcomes. Among 101 patients, predominantly with Castaing type I fractures (92.08%), very good subjective (84.16%), objective (77.23%), and radiological (75.25%) results were achieved at a mean follow-up of 27.27 months. Complications were minimal, and early rehabilitation contributed to robust recovery. These findings highlight the technique’s potential as a safe, effective alternative in environments lacking advanced imaging, challenging the reliance on fluoroscopy while affirming its applicability in low-resource contexts.
Epidemiological profile
In this series, males predominated (68.32%, n = 69), consistent with findings from Traore et al. and Parupalli and Mithun [16,17], but contrasting with studies reporting female predominance [18-20]. The male predominance likely reflects the higher exposure of young men to high-risk occupations and activities in South Kivu, such as manual labor and transportation. The mean age was 36.41 ± 12.61 years (range: 18-70), aligning with African series [17,21] but younger than Western cohorts [4]. This younger age profile may be attributed to the high-energy trauma mechanisms prevalent in a youthful Congolese population. Civil servants (n = 37, 36.63%), students (n = 13, 12.87%), and shopkeepers (n = 12, 11.88%) were the most affected occupations, mirroring patterns in African studies [16,17]. These groups’ active and mobile lifestyles increase their exposure to road traffic accidents and falls, the leading causes of injury in this study. Urban patients (78.22%, n = 79) outnumbered rural ones (19.80%, n = 20), differing from Dworkin et al. [22], likely due to the urban location of study hospitals facilitating easier access. Diabetes (n = 6, 5.94%) and osteoporosis (n = 3, 2.97%) were the primary comorbidities, consistent with Nemmar et al. [23]. These conditions may exacerbate bone fragility, contributing to fracture risk.
Clinical characteristics
Road traffic accidents (35.64%, n = 36) and falls from height (31.68%, n = 32) were the predominant etiologies, aligning with Traore et al. and Parupalli and Mithun [16,17]. This reflects South Kivu’s poor road infrastructure, non-compliance with traffic regulations, and mountainous terrain, which predispose to falls. The right wrist was more commonly affected (53.47%, n = 54) than the left (45.54%, n = 46), consistent with Kacimi et al. [18], likely due to the dominance of the right hand in most individuals, though some studies (e.g., Nemmar et al., 2024) [23] report otherwise, suggesting variability by chance or population.
Radiological findings
Per the modified Castaing classification, type I fractures dominated (92.08%, n = 93), followed by types 2 and 4 (2.97%, n = 3 each). The prevalence of extra-articular fractures, particularly Pouteau-Colles type, aligns with multiple studies [17,18,24,25]. This pattern likely results from the common compression-extension mechanism in this cohort, reflecting the high-energy trauma observed.
Treatment and perioperative outcomes
All fractures were reduced using external maneuvers and stabilized with fluoroscopy-free percutaneous intrafocal pinning, employing three pins via mini-incisions. Immediate postoperative radiographs showed excellent (48.51%, n = 49), very good (34.65%, n = 35), or good (12.87%, n = 13) alignment, underscoring the technique’s efficacy despite the absence of intraoperative imaging. The mean preoperative delay was short (1.34 ± 0.52 days), comparable to Ayouba et al. [15] and Panthi et al. [19], facilitated by urban proximity to hospitals and the urgency of pain-driven consultations. General anesthesia was universal, reflecting limited resources for locoregional anesthesia, consistent with Chgoura [25]. The mean hospital stay (3.70 ± 1.12 days) was slightly longer than reported by Panthi et al. [19] and Kacimi et al. [18], possibly due to socioeconomic constraints or insurance coverage variations. Consolidation occurred at 46.82 ± 4.67 days, within the expected four- to six-week range, similar to Ayouba et al. [15] and Khadka et al. [24], likely due to precise reduction and stable fixation. Pin and cast removal averaged 50.67 ± 6.01 days, aligning with standard protocols.
Complications and rehabilitation
Complications were infrequent, including superficial infections (2.97%, n = 3), malunion (2.97%, n = 3), pin migration (1.98%, n = 2), complex regional pain syndrome (0.99%, n = 1), twisted pin (0.99%, n = 1), radial sensory nerve injury (0.99%, n = 1), and extensor pollicis longus tendon injury (0.99%, n = 1). These rates are lower than or comparable to other series [22,25], likely due to meticulous surgical technique, including short incisions and early rehabilitation. Rehabilitation averaged 17.72 ± 3.22 sessions, consistent with Ayouba et al. [15], emphasizing its role in recovery. Peyroux et al. highlight physiotherapy’s benefits in reducing pain, edema, and improving function, supporting its critical role in this cohort [26].
Functional and radiological outcomes
At a mean follow-up of 27.27 ± 11.85 months, outcomes were excellent: subjective scores were very good in 84.16% (n = 85) and good in 9.90% (n = 10); objective scores were very good in 77.23% (n = 78) and good in 16.83% (n = 17); and radiological scores were very good in 75.25% (n = 76) and good in 19.80% (n = 20). These results align with Peyroux et al. [26], Nemmar et al. [23], and Parupalli and Mithun [17], surpassing some series (e.g., Ayouba et al. [15]). The consistency between functional and radiological outcomes reflects the young cohort’s recovery potential, precise surgical technique, and early rehabilitation. Notably, subjective and objective functional results slightly outperformed radiological outcomes, possibly due to the adaptive capacity of younger patients.
Statistical correlations
Principal component analysis (PCA) revealed that prolonged rehabilitation correlated with poorer scores, while shorter rehabilitation predicted better outcomes. Castaing type I fractures yielded superior results compared to types 4 and 8, reflecting simpler fracture patterns. Longer hospital stays were associated with worse objective scores, likely indicating more complex cases. Factorial analysis confirmed that poor objective scores predicted failed socio-professional reintegration, underscoring the societal impact of functional outcomes. Age and gender had no influence on outcomes, consistent with the literature.
Implications of fluoroscopy-free technique
The absence of an image intensifier, a potential limitation, did not compromise outcomes, challenging reliance on intraoperative imaging in resource-limited settings. While fluoroscopy ensures precision, its risks, including radiation-induced skin, thyroid, and ocular damage [12,13], highlight the value of alternative approaches. This study supports fluoroscopy-free pinning as a viable, safe technique, particularly where resources are scarce, echoing Nordback et al. [7].
Limitations
This study has several limitations. First, the absence of intraoperative fluoroscopy may have reduced the precision of fracture reduction and pin placement, particularly for complex fracture patterns, although outcomes remained favorable. Second, the cohort was predominantly composed of Castaing type I fractures (92.08%), potentially limiting the generalizability of fluoroscopy-free percutaneous intrafocal pinning to more complex distal radius fractures. Third, the study did not include a control group treated with fluoroscopy-guided pinning, precluding direct comparison of efficacy and safety between techniques. Fourth, long-term complications beyond the mean follow-up of 27.27 months were not assessed, possibly underestimating late sequelae specific to this approach. Finally, the reliance on manual reduction and anatomical landmarks introduces operator-dependent variability, which may affect reproducibility in less experienced hands.
Conclusions
Fluoroscopy-free percutaneous intrafocal pinning proved to be a highly effective and safe technique for managing distal radius fractures in adults in the resource-constrained setting of South Kivu, Democratic Republic of Congo. This prospective study demonstrated excellent anatomical, radiological, and functional outcomes, with very good subjective, objective, and radiological results at a mean follow-up period. The low complication rate and rapid consolidation underscore the technique’s reliability, even without intraoperative imaging. These findings challenge the necessity of fluoroscopy in simpler fracture patterns, such as Castaing type I, and highlight the critical role of early rehabilitation in optimizing recovery. By offering a viable alternative to resource-intensive methods, this approach holds significant promise for improving fracture care in low-resource settings globally. Future research should focus on comparative studies with fluoroscopy-guided pinning and long-term outcomes across diverse fracture types to further validate and refine this technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Distal radius fractures-why do they fail?J Orthop Dhandapani B Wahegaonkar A 24324920243809060510.1016/j.jor.2023.11.004PMC 10711036 · doi ↗ · pubmed ↗
- 2Functional outcome of distal radius fractures managed by minimally invasive plate osteosynthesis: a prospective study of 20 patients J Orthop Case Rep Dondapati A Pandian H Mohideen S Pradeep E Kumar KV Balamurugan P 26927315202510.13107/jocr.2025.v 15.i 05.5630 PMC 1206422640351646 · doi ↗ · pubmed ↗
- 3Epidemiology and treatment of distal radius fractures in Finland - a nationwide register study J Clin Med Raudasoja L Aspinen S Vastamäki H Ryhänen J Hulkkonen S 28511120223562897810.3390/jcm 11102851 PMC 9143261 · doi ↗ · pubmed ↗
- 4Distal radius fractures: approaches, indications, and techniques J Hand Surg Am Alluri RK Hill JR Ghiassi A 8458544120162734217110.1016/j.jhsa.2016.05.015 · doi ↗ · pubmed ↗
- 5Fixation of distal radius fractures in adults: a review Orthop Traumatol Surg Res Obert L Rey PB Uhring J 2162349920132351807010.1016/j.otsr.2012.03.023 · doi ↗ · pubmed ↗
- 6Management of distal radius fractures: evidence-based clinical practice guideline 12 2025 2020 https://www.aaos.org/globalassets/quality-and-practice-resources/distal-radius/drfcpg.pdf
- 7A proposed paradigm shift in the management of distal radius fractures J Orthop Nordback PH Ragupathi T Cheah AE 1171224920243815242610.1016/j.jor.2023.11.065PMC 10749825 · doi ↗ · pubmed ↗
- 8Epidemiology, classification, treatment and mortality of distal radius fractures in adults: an observational study of 23,394 fractures from the national Swedish fracture register BMC Musculoskelet Disord Rundgren J Bojan A Mellstrand Navarro C Enocson A 882120203203548810.1186/s 12891-020-3097-8PMC 7007648 · doi ↗ · pubmed ↗