Myocardial Bridging and Cardiac Arrest
Karthik V. Iyer, Robert J. Hieger, Rahul Rajput, Katherine L. Raymer, Ananya P. Ganesan, Souheil Khoukaz, Bassam Roukoz, Bassem Mikhail, Jooho P. Kim, Vikram V. Oke

TL;DR
This paper reports a case of myocardial bridging causing cardiac arrest and highlights its potentially dangerous effects, even without obstructive heart disease.
Contribution
The study adds a new clinical case and emphasizes the need to reconsider myocardial bridging as a non-benign condition.
Findings
Myocardial bridging can lead to sudden cardiac arrest even in the absence of obstructive coronary disease.
Ventricular fibrillation is the common arrest rhythm in MB-associated cardiac arrest cases.
Most reported cases involve the left anterior descending artery and predominantly affect men.
Abstract
Myocardial bridging (MB) is a congenital coronary anomaly in which a segment of an epicardial artery tunnels through the myocardium. Although frequently considered benign, MB has been increasingly linked to ischemia, malignant arrhythmias, and sudden cardiac death. We describe a case of a 39-year-old woman with mid–left anterior descending artery MB who presented with sudden chest pain followed by cardiac arrest. Coronary angiography revealed MB without obstructive disease. Despite prolonged resuscitation and hypoxic brain injury, she achieved functional recovery after intensive care. We compared our patient with 10 previously published cases of MB-associated cardiac arrest. Patients were typically men with ventricular fibrillation as the universal arrest rhythm, and the left anterior descending artery was most commonly involved, with variable outcomes. MB should not be regarded as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
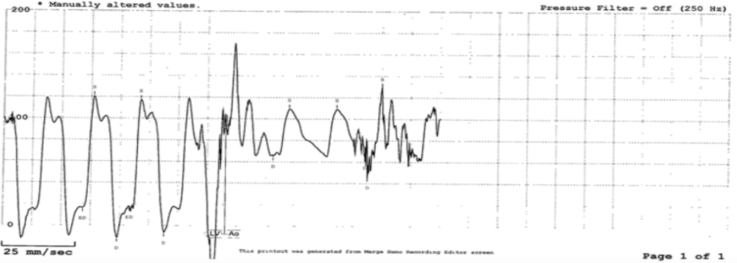 Figure 1
Figure 1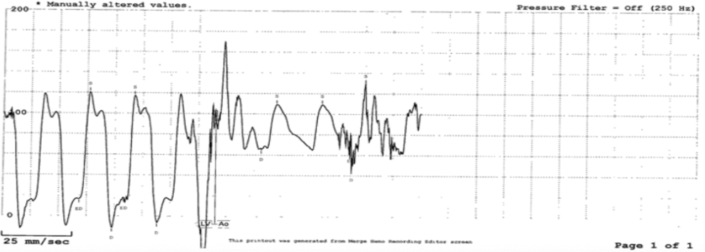 Figure 2
Figure 2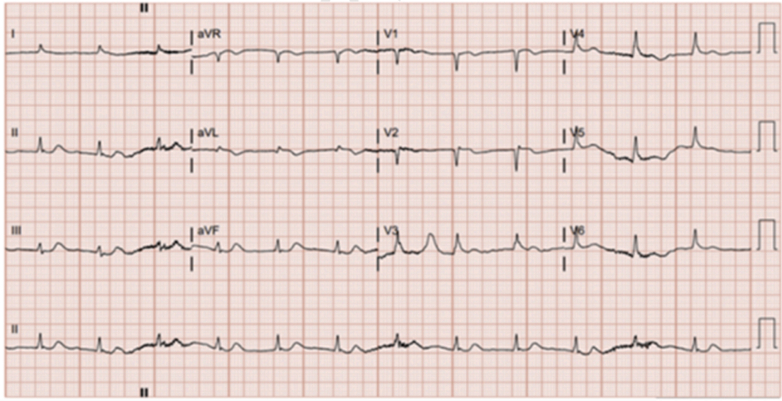 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Cardiac Structural Anomalies and Repair · Cardiac Arrhythmias and Treatments
Myocardial bridging (MB) is a congenital coronary anomaly in which a segment of an epicardial artery courses intramyocardially. First described by Reyman in 1732, MB was long regarded as a benign incidental finding.1 However, accumulating evidence demonstrates that MB can precipitate angina, myocardial ischemia, malignant arrhythmias, and sudden cardiac death. Prevalence varies by modality, reported in 1.5% to 16% of angiographic studies and up to 80% of autopsy series.2^,^3Take-Home Messages
- •Myocardial bridging should not be regarded as uniformly benign.
- •Recognition of its malignant potential—particularly in patients with no obstructive coronary disease—is critical for diagnosis, management, and secondary prevention.
Dynamic compression of the tunneled segment during systole reduces coronary perfusion, particularly in tachycardic states. Repetitive systolic compression creates abnormal shear stress that may injure the endothelium, resulting in endothelial dysfunction and impaired vasomotor reactivity. This predisposes to localized vasospasm and turbulent flow within the bridged segment, further compromising diastolic filling. In addition, recurrent flow acceleration and delayed relaxation can extend into the microcirculation and contribute to microvascular ischemia. These hemodynamic and structural changes are believed to promote arrhythmogenesis through heterogeneous repolarization and the development of myocardial fibrosis. These alterations can produce localized zones of delayed conduction and repolarization dispersion, forming the substrate for ventricular arrhythmias—especially under sympathetic stimulation.4 Although most cases are asymptomatic, certain anatomical features (bridge length, depth, and degree of systolic compression) and clinical contexts (exertion and vasospasm) increase the risk of ischemia and arrhythmia.
We present a case of out-of-hospital cardiac arrest attributed to mid–left anterior descending artery (LAD) MB and review the literature to highlight patterns and implications of MB as a cause of cardiac arrest.
Case Presentation
A 39-year-old woman with hypertension, hyperlipidemia, obesity, obstructive sleep apnea, epilepsy, and known mid-LAD MB presented with sudden severe chest pain at night. Sublingual nitroglycerin provided no relief. Shortly thereafter, she collapsed and was found by emergency medical services in ventricular fibrillation. She underwent 4 rounds of defibrillation and multiple rounds of cardiopulmonary resuscitation, achieving return of spontaneous circulation.
On arrival to the emergency department, the initial electrocardiogram showed ventricular tachycardia evolving into ventricular fibrillation. She had a history of non–ST-segment elevation myocardial infarction with elevated troponin (783 ng/L) and an ejection fraction of 40% to 45%, as shown in Figures 1 and 2.Figure 1EMS Rhythm StripEMS rhythm strip showing ventricular tachycardia on arrival, which rapidly deteriorated into ventricular fibrillation requiring defibrillation. EMS = emergency medical service.Figure 2. Initial Electrocardiogram Obtained in the Emergency DepartmentSlight ST-segment elevation is present in lead V_2_, consistent with septal myocardial infarction, with a prolonged QRS duration suggesting possible right ventricular conduction delay.
Cardiac catheterization revealed no obstructive coronary disease but confirmed MB of the mid- to distal LAD. Echocardiography showed mildly reduced global systolic function (ejection fraction 45%-50%) with apical wall hypokinesis (see Video 1 demonstrating MB of the mid- to distal LAD with associated coronary artery spasm).
The patient was admitted to the intensive care unit and treated with targeted temperature management. Her course was complicated by aspiration pneumonia, seizure-like activity, and hypoxic-ischemic brain injury on magnetic resonance imaging. She required tracheostomy and percutaneous endoscopic gastrostomy tube placement but gradually regained neurological function. She was ultimately decannulated and discharged home with functional recovery. Table 1 includes pertinent serum laboratory values obtained upon initial presentation to the hospital’s emergency department.Table 1. Pertinent Laboratory Values at PresentationLaboratory TestPatient ValueReference RangeUnits of MeasurementCardiac biomarkers Troponin (baseline)165≤10ng/L Troponin T (6 h)783<11ng/L CK-MB–––Metabolic/electrolytes Sodium (Na^+^)138135-145mmol/L Potassium (K^+^)3.73.5-5.1mmol/L Chloride (Cl^−^)10398-107mmol/L CO_2_1022-29mmol/L BUN176-20mg/dL Creatinine1.070.51-0.95mg/dL Glucose33474-99mg/dL Total protein5.86.6-8.7g/dL Albumin3.54.0-5.0g/dL Total bilirubin0.3≤1.2mg/dL Alkaline phosphatase9835-104U/L AST156<40U/L ALT138≤33U/L GFR>60≥60mL/min/1.73 m^2^ Anion gap255-15mmol/LHematology Hemoglobin13.511.9-15.1g/dL Hematocrit40.538.0-47.0% WBCs24.64.0-11.0×10^3^ cells/μL Platelets335150-400×10^3^ cells/μLInflammatory/coagulation CRP6.7≤5.0mg/L PT/INR––– aPTT–––Metabolic/endocrine HbA_1c_4.4≤5.6% Lactic acid13.9≤2.0mmol/LALT = alanine transaminase; aPTT = activated partial thromboplastin time; AST = aspartate transaminase; BUN = blood urea nitrogen; CK-MB = creatine kinase-MB; CO_2_ = bicarbonate; CRP = C-reactive protein; GFR = glomerular filtration rate; HbA_1c_ = glycosylated hemoglobin; PT/INR = prothrombin time/international normalized ratio; WBC = white blood cell.
Discussion
This case adds to a growing body of literature illustrating the malignant potential of MB. Although MB is common and often regarded as a benign congenital anomaly, in certain patients, it can serve as a precipitant of ventricular fibrillation and cardiac arrest. To contextualize our findings, we compared our patient with 10 previously published cases of MB-associated cardiac arrest, as shown in Table 2.Table 2. Clinical Characteristics, Interventions, and Outcomes of Patients With Myocardial Bridging–Related Cardiac ArrestPatientaGenderAge, yComorbiditiesPresentationRhythmArteryInterventionsbLaboratory ResultsECGMB DxOutcomeAF50NoneSudden LOCVFDistal LAD and diagonal branches10 min CPR, 5 defib, intubation 4 d, CCB and ARB↑ WBC, proBNP, troponin I, D-dimerRBBB, ST ↑, Q V1-V4CAG, CMRAliveAsymp 1 yBM43Smoked 1 ppdSudden LOCVFLADDefib 5 min, ICDNormalT inv anterolateral, normalized 3 dCAGAliveAsymp 18 moCM17NoneArrest during exerciseVFMid-LAD (3 × 1 cm)3 defib, intubation 48 h, surgical unroofing; postoperatively treated with diltiazem and bisoprolol; consented for ICD insertion due to the history of v-fibN/AST ↓Coronary CTAliveAsymp 3 moDM21NoneArrest during exerciseVFLAD (1.8 cm)CPR, 2 defibN/AN/AAutopsyDiedEM46LVH, normal stressSudden LOCVFLCx (1.3 cm)CPR, defib, debridging operation; no symptoms discharged on CCBNormalNegative T waves in the precordial and inferior leadsCAGAliveAsymp 6 moFF52HTNCP, sudden LOCVFMid-LADCPR, defib, antiplatelet agents, high-intensity statins, CCBs; patient remained symptom free on follow-up visits↑ Troponin I (1.332 ng/mL)ST ↑ with pathologic Q wavesCAGAliveAsymp on follow-upGM52Dilated cardiomyopathy (recipient)Sudden cardiac death on postop day 2 after heart transplantationNot specifiedMid-LAD (1.8 cm intramural course)Heart transplantation (biatrial method) due to the diagnosis of dilated cardiomyopathyNo rejection (C4d negative)Not specifiedAutopsyDied on postop day 2HM12Hypoplastic coronariesCP and LOC during mild exerciseVentricular arrhythmiaLADLoop recorder, advised restriction of exertionTroponin ↑; stress perfusion CMR: large perfusion defect; MRI: fibrosisST ↓Coronary CT, MRI, CAGDiedAsymp at 1 y follow-up, died shortly after while exercisingIM29Tobacco, alcohol useFirst: sudden LOCSecond (4 mo later): sudden LOCFirst: polymorphic VTach, VFSecond: VFLAD (20 mm, ∼80% systolic compression)First: CPR, multiple shocks, intubation (“number of days”)Second: multiple rounds of defib, patient refused surgical treatment; discharged on empirical amiodaroneFirst: pH 7.18, K^+^ 2.8, CPK 8,000 (MB 40)Second: CPK 590 (MB 71)ST ↑ anterolateral/inferior; later diffuse St-T; +SAECGCAGAliveAsymp 2 moJM17NoneSudden LOC during exerciseVFLADCPR, defib, ICD implantationMild ↑ troponin T; electrolytes and inflammatory markers normalTransient borderline prolonged QT intervalCAGAlivePostanoxic encephalopathy with persistent short-term memory lossKF38HTN, HLD, obesity, OSA, former smoker (quit in January 2024), NSTEMI, epilepsyCP the day before; CP, SOB, LOC on the day of presentationVFLADCPR, 3 defib, intubation (15-20 min estimated total time of arrest), tracheostomy and PEG tube placed on day 9 of admission EV-ICD placement, discharged to LTAC with diltiazemElevated WBC, troponin T, glucose, AST, ALT, Mg, CRPLow QRS voltage, possible RV conduction delay, septal MICAGAliveHypoxemic brain injuryLong-term or guideline-directed medical therapy (eg, β-blockers and anticoagulants) is not included.↑ = increased; ALT = alanine transaminase; ARB = angiotensin receptor blocker; AST = aspartate transaminase; Asymp = asymptomatic; CAG = coronary angiography; CCB = calcium-channel blocker; CMR = cardiac magnetic resonance; CP = chest pain; CPK = creatine phosphokinase; CPR = cardiopulmonary resuscitation; CRP = C-reactive protein; CT = computed tomography; defib = defibrillation; ECG = electrocardiogram; EV-ICD = epicardial/ventricular implantable cardioverter-defibrillator; F = female; HLD = hyperlipidemia; HTN = hypertension; ICD = implantable cardioverter-defibrillator; LAD = left anterior descending artery; LCx = left circumflex artery; LOC = loss of consciousness; LTAC = long-term acute care facility; LVH = left ventricular hypertrophy; M = male; MB = myocardial bridge; MB Dx = myocardial bridge diagnosis; MI = myocardial infarction; MRI = magnetic resonance imaging; N/A = not available; NSTEMI = non–ST-segment elevation myocardial infarction; OSA = obstructive sleep apnea; proBNP = NT-proBNP 1/4 N-terminal pro–B-type natriuretic peptide; PEG = percutaneous endoscopic gastrostomy; postop = postoperative; ppd = pack-per-day (tobacco use); RBBB = right bundle branch block; RV = right ventricular; +SAECG = positive signal-averaged electrocardiogram; SOB = shortness of breath; ST ↑ = ST-segment elevation; ST ↓ = ST-segment depression; St-T = ST-T segment; T inv = T-wave inversion; VF = ventricular fibrillation; v-fib = ventricular fibrillation; VTach = ventricular tachycardia; WBC = white blood cell.aCase sources: Patient A = Ki10; patient B = Sciahbasi et al8; patient C = Toya et al11; patient D = Ceauşu et al7; patient E = Tio et al12; patient F = Oh et al13; patient G = Phulware et al 14; patient H = Holtrup et al15; patient I = Cutler and Wallace9; patient J = Knaapen et al16; patient K = current case.bInterventions listed reflect immediate resuscitation measures (eg, CPR, defibrillation, and intubation).
Our analysis of these cases alongside our own reveals several striking consistencies. The mean age was 34 years, with a strong male predominance (73%). The vast majority of patients had no comorbidities, and ventricular fibrillation was the presenting rhythm at the time of cardiac arrest. Most patients collapsed suddenly without prodrome, and nearly one-third experienced arrest during exertion. The LAD was implicated in 82% of cases, aligning with prior reports of MB's anatomic predilection.5 Outcomes were heterogeneous: although 73% survived, 27% died, and 2 survivors (including our patient) sustained neurologic sequelae. These findings underscore that MB, although often regarded as benign, carries malignant potential, particularly when involving the LAD, and can lead not only to sudden death but also to long-term morbidity in survivors.
The mechanisms by which MB precipitates malignant arrhythmias remain multifactorial. Dynamic systolic compression of the tunneled artery can impair coronary perfusion, particularly during tachycardia or stress. Because coronary blood flow occurs primarily in diastole, most systolic bridges are clinically silent; however, tachycardia shortens diastolic filling time and can convert an otherwise benign bridge into a clinically significant source of ischemia.6 Associated endothelial dysfunction, vasospasm, or myocardial remodeling may further increase arrhythmic risk. Diagnostic challenges arise because MB is frequently discovered incidentally on coronary angiography, and ischemic changes may be absent unless provoked. Advanced imaging, such as intravascular ultrasound, computed tomography angiography, or stress perfusion studies, may help identify high-risk bridges.1
Management of MB requires an individualized stepwise approach based on symptom severity, anatomic features, and response to medical therapy. Initial treatment focuses on medical management, primarily with β-blockers or calcium-channel blockers (CCBs) to reduce heart rate, prolong diastole, and lessen systolic compression of the tunneled artery. Some reports suggest CCBs may be superior in cases with associated coronary spasm, as β-blockers can occasionally exacerbate systolic narrowing.7 Nitrates should generally be avoided, as they dilate the nonbridged arterial segments, increase the pressure gradient across the bridged area, and reduce preload, leading to reflex tachycardia and worsened compression. Ivabradine may be used off-label in patients intolerant to β-blockers or CCBs, particularly those with reduced ejection fraction.8 Patients with mild or incidental findings, such as young athletes, may be managed conservatively with lifestyle modifications—avoiding excessive exertion, stress, and stimulants—while undergoing continued monitoring or cardiac magnetic resonance imaging to rule out structural abnormalities.
In cases refractory to medical therapy, interventional or surgical options may be considered. Percutaneous coronary intervention is generally reserved for short superficial bridges but carries high complication rates, including in-stent restenosis up to 75% with bare-metal stents and 25% with drug-eluting stents, as well as 6% stent perforation.8 Surgical management, such as myotomy (unroofing) or coronary artery bypass grafting (CABG), is indicated for deep (>5 mm) or long (>25 mm) bridges or when percutaneous coronary intervention fails.9 Myotomy directly relieves compression but may lead to chest pain recurrence in up to 60% of adults due to residual endothelial dysfunction.8 CABG using saphenous vein grafts has higher long-term patency (∼80%) compared to LIMA-LAD grafts (only 10% patent at 18 months) due to competitive flow. Outcomes data suggest lower major adverse cardiac event rates with myotomy (7%) than with CABG (41%).8 In patients presenting with ventricular tachyarrhythmias or cardiac arrest, implantable cardioverter-defibrillator placement is warranted for secondary prevention. After comparison, about 50% of patients were discharged with rate-controlling medications, and patients with an initial rhythm of ventricular fibrillation underwent implantable cardioverter-defibrillator placement or were recommended to receive one. Surgical unroofing was done in only 2 cases, and 1 patient refused surgical treatment. Overall, management should be tailored to anatomy, symptoms, and patient preferences, with a focus on hemodynamic control, risk factor modification, and cautious escalation to invasive interventions when medical therapy is insufficient.
Conclusions
MB, although often considered benign, can have life-threatening consequences. Across published cases and our own, common features included ventricular fibrillation arrest, LAD involvement, and sudden collapse, often in otherwise healthy individuals. Recognition of MB's malignant potential is critical, particularly when patients present with ischemia or cardiac arrest in the absence of obstructive coronary artery disease. Although systolic bridging alone is frequently benign, tachycardia and other stressors that reduce diastolic perfusion can unmask its malignant potential. Early identification and appropriate secondary prevention strategies may improve outcomes in this under-recognized population.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sternheim D.Power D.Samtani R.Kini A.Fuster V.Sharma S.Myocardial bridging: diagnosis, functional assessment, and management J Am Coll Cardiol 782220212196221210.1016/j.jacc.2021.09.85934823663 · doi ↗ · pubmed ↗
- 2Bansro V.Gurbakhshani M.Siddiq H.Shetty R.A young adult with myocardial bridging: a case report Cureus 1572023 e 4145210.7759/cureus.41452 PMC 1040406137546119 · doi ↗ · pubmed ↗
- 3Lee M.S.Chen C.-H.Myocardial bridging: an up-to-date review J Invasive Cardiol 2711201552152825999138 PMC 4818117 · pubmed ↗
- 4Toya T.Coronary endothelial dysfunction and vasomotor dysregulation in myocardial bridging J Cardiovasc Dev Dis 12220255410.3390/jcdd 1202005439997488 PMC 11856107 · doi ↗ · pubmed ↗
- 5Choi J.G.Park C.Lee C.Choi J.Ventricular fibrillation due to coronary spasm at the site of myocardial bridge -A case report Korean J Anesthesiol 58120109910.4097/kjae.2010.58.1.9920498820 PMC 2872901 · doi ↗ · pubmed ↗
- 6Evbayekha E.Nwogwugwu E.Olawoye A.A comprehensive review of myocardial bridging: exploring diagnostic and treatment modalities Cureus 1582023 e 4313210.7759/cureus.43132 PMC 1048404137692750 · doi ↗ · pubmed ↗
- 7Ceauşu M.Ionescu R.A.Mălinescu B.Rusu M.C.Hostiuc S.Dermengiu D.Sudden cardiac death due to triple myocardial bridging associated with atypical coronary topography Rom J Morphol Embryol 543 Suppl 201383383724322036 · pubmed ↗
- 8Sciahbasi A.Summaria F.Patrizi R.Lioy E.Cardiac arrest and myocardial bridging Ital Heart J 511200486987115633444 · pubmed ↗