Mind the Gap: Adult Paradigms and Pediatric Realities in Blunt Traumatic Aortic Injury
Matylda M. Mazur, Anna Kędziora

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1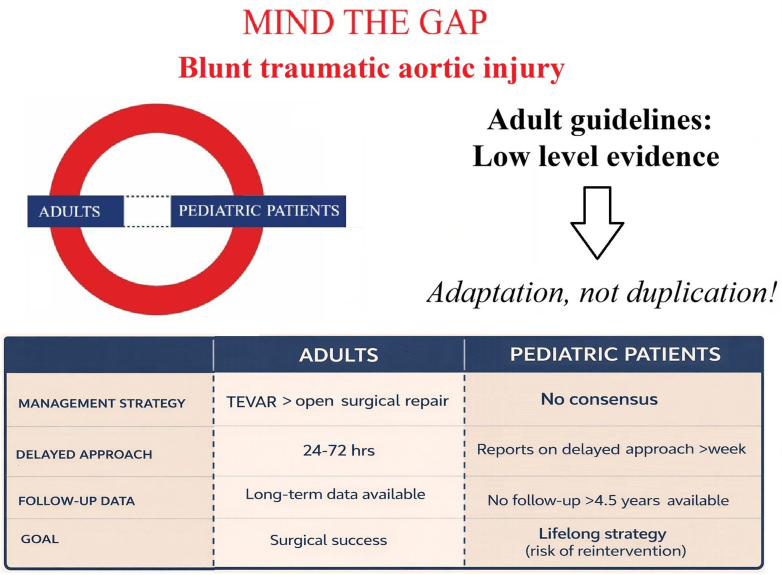 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Aortic injuries in pediatric survivors of motor vehicle accidents are rare. However, the growing use of off-road and youth-sized all-terrain vehicles may shift this landscape, making these injuries an increasingly more common scenario observed in clinical practice. Management is challenging not only because these cases often involve complex, multiorgan trauma, but more so due to the absence of evidence-based guidelines, particularly regarding the timing and modality of intervention in pediatric patients. In this context, well-documented case reports are indispensable, as they illustrate real-world decision-making in high-stakes settings.
In this issue, Portuondo et al1 present a case of an 11-year-old who, following an all-terrain vehicle accident, sustained a transverse aortic arch pseudoaneurysm along with an esophageal tear and pulmonary and cardiac contusions. The latter warranted a 5-day-long veno-arterial extracorporeal membrane oxygenation support and a balloon atrial septostomy to be performed. Subsequently, the multidisciplinary team elected for tight blood pressure control, serial imaging, and other injuries stabilization. Eight weeks after the initial accident, a surgical transverse aortic arch pseudoaneurysm repair with an oversized Dacron graft was performed. Throughout the hospital stay, the patient remained neurologically intact. At 11 months postdischarge, the echocardiography was reassuring, and the patient returned to normal activity level.
One of the key clinical dilemmas is whether blunt traumatic aortic injury (BTAI) should be treated immediately or managed in a staged fashion with initial conservative stabilization. In pediatric patients, treatment strategy by large is extrapolated from the adult guidelines. While a delayed (>24 hours) approach is allowed for contained injuries in adults, it rarely exceeds 72 hours.2, 3, 4, 5, 6 The growing number of pediatric case reports demonstrate that the timing of an intervention can be delayed even by a couple of weeks, with favorable outcomes observed up to 4.5 years after the intervention.7^,^8 In the case presented by Portuondo et al, the surgical intervention was delayed for 8 weeks, which resulted in a good medium-term outcome. That could potentially suggest that high elasticity and compliance of the aorta in pediatric patients can be more forgiving than in an adult, where trauma is superimposed on pre-existing atherosclerosis and calcifications, making the aorta more fragile and prone to rupture.
Beyond determining the optimal timing, selecting the mode of intervention remains a challenge (Figure 1). In adults with high-grade BTAI, thoracic endovascular aortic repair (TEVAR) is currently the gold standard, with open surgical repair reserved for patients with unfavorable anatomy.2^,^3^,^6 Notably, these Class I recommendations are supported by a low Level of Evidence (LOE: C).2^,^3 In children, the same recommendations exist largely in a vacuum of pediatric-specific data, device approvals, and the scarcity of long-term outcome evidence.Figure 1. Challenges in Translating Adult Blunt Traumatic Aortic Injury Guidelines to Pediatric Practice
Adult literature overwhelmingly favors TEVAR, demonstrating lower early mortality and reduced rates of paraplegia and transfusion requirements.9 Meanwhile, pediatric patients undergoing TEVAR appear to have higher rates of traumatic brain injury than those undergoing open repair, without any difference in mortality.8 An increasing number of case reports support the use of TEVAR in children.7^,^10 The case presented in this issue was managed with open surgical repair. This approach should not be interpreted as a rejection of TEVAR. Rather, it reinforces that pediatric BTAI requires individualized decision-making, guided by lesion location, patient size, associated injuries, and institutional expertise. Multidisciplinary discussion is not ancillary here—it is central to safe and effective care.
The management of BTAI in children remains one of the most daunting surgical and cardiac challenges. The report by Portuondo et al underscores that the question is not simply whether to intervene, but when and how, and an individualized approach combined with the art of applying adult-derived algorithms may confer durable clinical success.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maza Portuondo L.Li B.Chakiath M.Traumatic transverse aortic arch pseudoaneurysm in a pediatric patient JACC Case Rep 3110202610693610.1016/j.jaccas.2026.10693641817266 · doi ↗ · pubmed ↗
- 2Czerny M.Grabenwöger M.Berger T.EACTS/STS Scientific Document Group EACTS/STS Guidelines for diagnosing and treating acute and chronic syndromes of the aortic organ Eur J Cardiothorac Surg 6522024 ezad 42610.1093/ejcts/ezad 42638408364 · doi ↗ · pubmed ↗
- 3Czerny M.Schmidli J.Adler S.EACTS/ESVS Scientific Document Group Current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Society for Vascular Surgery (ESVS)Eur J Cardiothorac Surg 551201913316210.1093/ejcts/ezy 31330312382 · doi ↗ · pubmed ↗
- 4Demetriades D.Velmahos G.C.Scalea T.M.Operative repair or endovascular stent graft in blunt traumatic thoracic aortic injuries: results of an American Association for the Surgery of Trauma Multicenter Study J Trauma 643200856157010.1097/TA.0b 013e 3181641 bb 318332794 · doi ↗ · pubmed ↗
- 5Demetriades D.Velmahos G.C.Scalea T.M.Diagnosis and treatment of blunt thoracic aortic injuries: changing perspectives J Trauma 646200814151418[discussion: 1418-1419]10.1097/TA.0b 013e 3181715 e 3218545103 · doi ↗ · pubmed ↗
- 6Fox N.Schwartz D.Salazar J.H.Evaluation and management of blunt traumatic aortic injury: a practice management guideline from the Eastern Association for the Surgery of Trauma J Trauma Acute Care Surg 78120151361462553921510.1097/TA.0000000000000470 · doi ↗ · pubmed ↗
- 7Afzal M.Abdulreda Najar S.Baghazal H.Alshahwani N.Endovascular treatment of a traumatic thoracic pseudo-aneurysm in a pediatric patient: a case report with review of literature J Cardiothorac Surg 18202318310.1186/s 13019-023-02265-737198595 PMC 10193714 · doi ↗ · pubmed ↗
- 8Hasjim B.J.Grigorian A.Barrios C.Jr.National trends of thoracic endovascular aortic repair versus open thoracic aortic repair in pediatric blunt thoracic aortic injury Ann Vasc Surg 59201915015710.1016/j.avsg.2018.12.09430802562 · doi ↗ · pubmed ↗