Central corneal thickness, corneal endothelial cell density, and morphology in myopic eyes of young Chinese candidates for refractive surgery
Suming Wu, Zhengwei Zhang, Jing Wang, Xuechun Gong, Dongyan Guo, Nan Ye

TL;DR
This study examines corneal thickness and endothelial cell characteristics in young Chinese individuals with myopia who are considering refractive surgery.
Contribution
The study provides insights into the relationship between age, gender, and corneal parameters in myopic refractive surgery candidates.
Findings
Age showed weak negative correlations with central corneal thickness and endothelial cell density.
Males had slightly higher central corneal thickness and endothelial cell hexagonality compared to females.
Spherical equivalent and axial length did not significantly affect corneal thickness or endothelial cell morphology.
Abstract
To assess central corneal thickness (CCT), as well as the density and morphology of corneal endothelial cells (ECD) in myopic eyes. A total of 400 patients scheduled for myopic refractive surgery were consecutively enrolled in this study. Preoperative evaluations encompassed endothelial cell density (ECD), average cell area (CA), coefficient of variation (CV), and percentage of hexagonality (HEX), all measured using the Nidek CEM-530. Additionally, central corneal thickness (CCT) was assessed using the Pentacam HR. Ocular biometric parameters, including axial length (AL), were recorded with the IOL Master 700. Each parameter was analyzed based on ocular laterality, age, gender, spherical equivalent (SE), and AL. The analysis revealed that 39% of participants were female, with a mean age of 25.36 ± 6.92 years and a mean SE of -5.06 ± 1.92D. No statistically significant differences in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
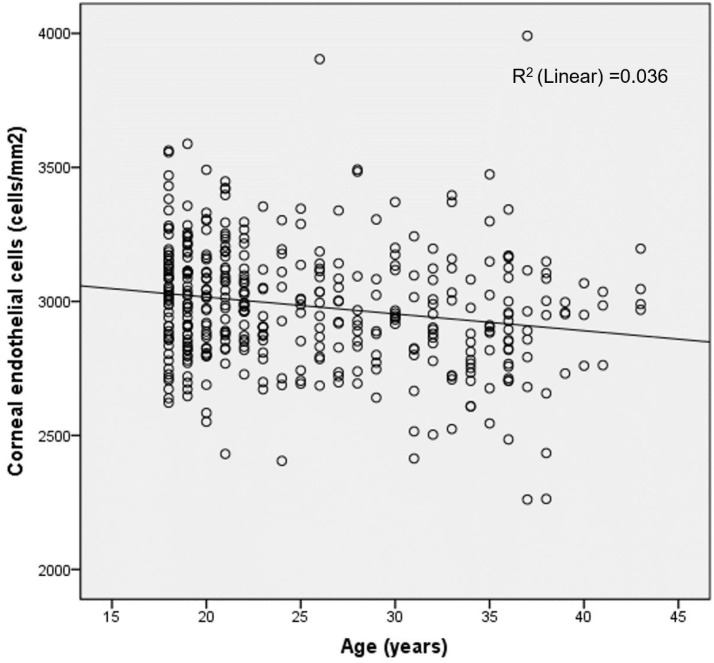 Figure 1
Figure 1| Parameters | All eyes | OD | OS |
|
|---|---|---|---|---|
| No. | 800 | 400 | 400 | |
| Pupil diameter (mm) | 3.42 ± 0.68 (1.93-5.92) | 3.53 ± 0.71 (1.93-5.92) | 3.32 ± 0.66 (1.97-5.47) |
|
| IOP (mmHg) | 15.42 ± 2.85 (8.0-25.0) | 15.54 ± 2.88 (9.0-24.0) | 15.29 ± 2.82 (8.0-25.0) |
|
| SE (D) | -4.92 ± 1.91 (-15.37--0.50) | -5.06 ± 1.92 (-15.37--0.50) | -4.78 ± 1.89 (-10.63--0.50) |
|
| AL (mm) | 25.71 ± 1.19 (22.10-37.54) | 25.77 ± 1.26 (22.98-37.54) | 25.64 ± 1.12 (22.10-29.53) |
|
| ACD (mm) | 3.72 ± 0.27 (2.78-4.52) | 3.72 ± 0.27 (2.78-4.52) | 3.72 ± 0.26 (3.08-4.49) | 0.122 |
| LT (mm) | 3.62 ± 0.28 (2.90-5.21) | 3.62 ± 0.28 (2.90-5.21) | 3.63 ± 0.27 (2.90-4.62) | 0.779 |
| WTW (mm) | 12.08 ± 0.41 (10.40-13.50) | 12.08 ± 0.40 (11.1-13.3) | 12.08 ± 0.42 (10.4-13.5) | 0.948 |
| ECD (cells/mm2) | 2993.50 ± 236.18 (2113-3991) | 2982.39 ± 227.22 (2261-3991) | 3004.61 ± 244.58 (2113-3988) |
|
| CA (µm2) | 317.99 ± 25.90 (249.0-455.0) | 318.97 ± 25.03 (265.0-425.0) | 317.01 ± 26.73 (249.0-455.0) |
|
| CV (%) | 28.53 ± 4.85 (19.0-75.0) | 28.50 ± 4.49 (19.0-47.0) | 28.57 ± 5.19 (20.0-75.0) | 0.774 |
| HEX (%) | 64.94 ± 5.90 (26-82) | 65.14 ± 5.83 (29.0-82.0) | 64.75 ± 5.97 (26.0-80.0) | 0.209 |
| CCT (μm) | 548.41 ± 29.00 (468-629) | 547.72 ± 29.01 (468.0-629.0) | 549.10 ± 29.00 (477.0-629.0) |
|
| Parameters | All eyes (OD) | Female | Male |
|
|---|---|---|---|---|
| No. | 400 | 156 | 244 | |
| Age | 25.36 ± 6.92 (18-43) | 29.39 ± 6.95 (18-43) | 22.78 ± 5.55 (18-40) |
|
| Pupil diameter (mm) | 3.53 ± 0.71 (1.93-5.92) | 3.40 ± 0.70 (2-5.34) | 3.60 ± 0.70 (1.93-5.92) |
|
| IOP (mmHg) | 15.54 ± 2.88 (9.0-24.0) | 14.89 ± 2.47 (9-20) | 15.96 ± 3.04 (9-24) |
|
| SE (D) | -5.06 ± 1.92 (-15.38--0.50) | -5.03 ± 1.63 (-9.50--0.50) | -5.08 ± 2.08 (-15.38--0.50) | 0.777 |
| AL (mm) | 25.77 ± 1.26 (22.98-37.54) | 25.31 ± 1.00 (22.98-27.63) | 26.06 ± 1.32 (23.43-37.54) |
|
| ACD (mm) | 3.72 ± 0.27 (2.78-4.52) | 3.60 ± 0.25 (3.07-4.27) | 3.80 ± 0.25 (2.78-4.52) |
|
| LT (mm) | 3.62 ± 0.28 (2.90-5.21) | 3.74 ± 0.28 (2.90-4.59) | 3.54 ± 0.24 (2.97-5.21) |
|
| WTW (mm) | 12.08 ± 0.40 (11.1-13.3) | 11.94 ± 0.38 (11.1-12.9) | 12.17 ± 0.39 (11.2-13.3) |
|
| ECD (cells/mm2) | 2982.39 ± 227.22 (2261-3991) | 2971.06 ± 251.97 (2263-3991) | 2989.64 ± 210.10 (2261-3563) | 0.122* |
| CA (µm2) | 318.97 ± 25.03 (265.0-425.0) | 319.74 ± 25.95 (265.0-425.0) | 318.48 ± 24.47 (267-418) | 0.428* |
| CV (%) | 28.50 ± 4.49 (19.0-47.0) | 30.06 ± 4.74 (21.0-42.0) | 27.50 ± 4.02 (19.0-47.0) | |
| HEX (%) | 65.14 ± 5.83 (29-82) | 64.20 ± 5.91 (48.0-82.0) | 65.74 ± 5.71 (29.0-78.0) | 0.251* |
| CCT (μm) | 547.72 ± 29.01 (468-629) | 543.62 ± 28.57 (477-629) | 550.34 ± 29.05 (468-614) |
| Parameters | All eyes (OD) | AL<24.0mm | 24.0mm≤AL<26mm | AL≥26.0mm |
|
|---|---|---|---|---|---|
| No. | 400 | 22 | 220 | 158 | |
| Age | 25.36 ± 6.92 (18-43) | 27.86 ± 7.29 (18-43) | 26.08 ± 7.17 (18-43) | 24.00 ± 6.29 (18-43) |
|
| Pupil diameter (mm) | 3.57 ± 0.70 (1.93-5.92) | 3.46 ± 0.65 (2.65-4.50) | 3.50 ± 0.70 (2.00-5.92) | 3.57 ± 0.72 (1.93-5.45) | 0.560 |
| IOP (mmHg) | 15.54 ± 2.88 (9.0-24.0) | 15.36 ± 2.85 (10.0-21.0) | 15.52 ± 3.01 (9.0-24.0) | 15.59 ± 2.70 (9.0-23.0) | 0.929 |
| SE (D) | -5.06 ± 1.92 (-15.37--0.5) | -2.70 ± 1.72 (-5.25--0.5) | -4.44 ± 1.61 (-15.37--1.50) | -6.26 ± 1.60 (-11.00--1.75) |
|
| AL (mm) | 25.77 ± 1.26 (22.98-37.4) | 23.61 ± 0.27 (22.98-23.95) | 25.17 ± 0.51 (24.01-25.99) | 26.91 ± 1.10 (26.00-37.54) |
|
| ACD (mm) | 3.72 ± 0.27 (2.78-4.52) | 3.50 ± 0.26 (3.07-4.32) | 3.67 ± 0.25 (3.09-4.33) | 3.82 ± 0.26 (2.78-4.52) |
|
| LT (mm) | 3.62 ± 0.28 (2.90-5.21) | 3.78 ± 0.26 (3.32-4.37) | 3.64 ± 0.27 (3.09-4.59) | 3.56 ± 0.29 (2.90-5.21) |
|
| WTW (mm) | 12.08 ± 0.40 (11.1-13.3) | 11.80 ± 0.40 (11.2-12.6) | 12.01 ± 0.39 (11.1-11.3) | 12.22 ± 0.37 (11.4-13.1) |
|
| ECD (cells/mm2) | 2982.39 ± 227.22 (2261-3991) | 2955.45 ± 189.65 (2639-3273) | 2984.42 ± 218.72 (2261-3991) | 2983.32 ± 244.04 (2263-3904) | 0.849 |
| CA (µm2) | 318.97 ± 25.03 (265.0-425.0) | 321.96 ± 21.85 (282.0-364.0) | 317.74 ± 23.87 (267.0-418.0) | 320.27 ± 26.99 (265.0-425.0) | 0.532 |
| CV (%) | 28.50 ± 4.49 (19.0-47.0) | 27.91 ± 4.89 (21.0 -41.0) | 28.82 ± 4.43 (19.0-42.0) | 28.15 ± 4.51 (20.0-47.0) | 0.291 |
| HEX (%) | 65.14 ± 5.83 (29.0-82.0) | 66.36 ± 5.86 (57.0-79.0) | 64.63 ± 5.76 (48.0-82.0) | 65.67 ± 5.89 (29.0-77.0) | 0.143 |
| CCT (μm) | 547.72 ± 29.01 (468.0-629.0) | 539.34 ± 27.16 (481.0-606.0) | 548.26 ± 30.50 (468.0-629.0) | 550.13 ± 26.40 (493.0-614.0) | 0.095 |
| Parameters | All eyes (OD) | -3.0D<SE≤-0.50D | -6.0D<SE≤-3.0D | SE≤-6.0D |
|
|---|---|---|---|---|---|
| No. | 400 | 50 | 228 | 122 | |
| Age | 25.36 ± 6.92 (18.0-43.0) | 26.08 ± 7.55 (18.0-41.0) | 25.43 ± 6.90 (18.0-43.0) | 24.91 ± 6.72 (18.0-43.0) | 0.583 |
| Pupil diameter (mm) | 3.53 ± 0.71 (1.93-5.92) | 3.44 ± 0.63 (2.36-4.85) | 3.52 ± 0.68 (1.93-5.45) | 3.57 ± 0.78 (2.00-5.92) | 0.545 |
| IOP (mmHg) | 15.54 ± 2.88 (9.0-24.0) | 15.64 ± 3.16 (10.0-22.0) | 15.40 ± 2.92 (9.0-24.0) | 15.77 ± 2.68 (9.0-23.0) | 0.491 |
| SE (D) | -5.06 ± 1.92 (-15.37--0.50) | -2.11 ± 0.72 (-2.87--0.50) | -4.53 ± 0.83 (-5.87--3.00) | -7.26 ± 1.27 (-15.37--6.00) |
|
| AL (mm) | 25.77 ± 1.26 (22.98-37.54) | 24.57 ± 0.75 (22.98-26.30) | 25.57 ± 1.19 (23.18-37.54) | 26.63 ± 0.98 (24.38-29.94) |
|
| ACD (mm) | 3.72 ± 0.27 (2.78-4.52) | 3.67 ± 0.23 (3.28-4.32) | 3.71 ± 0.26 (3.07-4.33) | 3.76 ± 0.29 (2.78-4.52) | 0.104 |
| LT (mm) | 3.62 ± 0.28 (2.90-5.21) | 3.65 ± 0.28 (3.09-4.37) | 3.62 ± 0.28 (2.90-4.59) | 3.61 ± 0.31 (3.09-5.21) | 0.761 |
| WTW (mm) | 12.08 ± 0.40 (11.1-13.3) | 12.13 ± 0.43 (11.2-13.2) | 12.07 ± 0.40 (11.1-13.3) | 12.09 ± 0.38 (11.4-12.9) | 0.607 |
| ECD (cells/mm2) | 2982.39 ± 227.22 (2261-3991) | 2991.22 ± 252.89 (2261-3991) | 2969.10 ± 213.86 (2263-3563) | 3003.62 ± 240.26 (2405-3904) | 0.384 |
| CA (µm2) | 318.97 ± 25.03 (265.0-425.0) | 319.34 ± 25.43 (267.0-418.0) | 319.88 ± 24.95 (266.0-425.0) | 317.12 ± 25.14 (265.0-402.0) | 0.613 |
| CV (%) | 28.50 ± 4.49 (19.0-47.0) | 28.06 ± 4.98 (19.0-41.0) | 28.34 ± 4.07 (21.0-39.0) | 28.99 ± 4.99 (20.0-47.0) | 0.327 |
| HEX (%) | 65.14 ± 5.83 (29.0-82.0) | 65.84 ± 6.16 (51.0-79.0) | 65.25 ± 5.40 (53.0-82.0) | 64.64 ± 6.45 (29.0-76.0) | 0.428 |
| CCT (μm) | 547.72 ± 29.01 (468.0-629.0) | 539.34 ± 27.16 (481.0-606.0) | 548.26 ± 30.50 (468.0-629.0) | 550.13 ± 26.40 (493.0-614.0) | 0.078 |
| Parameters | All eyes (OD) | < 30 years | ≥30 years |
|
|---|---|---|---|---|
| No. | 400 | 283 | 117 | |
| Age | 25.36 ± 6.92 (18-43) | 21.50 ± 3.23 (18-29) | 34.83 ± 3.23 (30-43) |
|
| Pupil diameter (mm) | 3.53 ± 0.71 (1.93-5.92) | 3.56 ± 0.69 (2.00-5.92) | 3.45 ± 0.74 (1.93-5.45) | 0.168 |
| IOP (mmHg) | 15.54 ± 2.88 (9.0-24.0) | 15.87 ± 2.94 (9.0-24.0) | 14.74 ± 2.54 (10.0-21.0) |
|
| SE (D) | -5.06 ± 1.92 (-15.38--0.50) | -5.14 ± 1.94 (-11.0--0.50) | -4.86 ± 1.86 (-15.38--1.63) | 0.183 |
| AL (mm) | 25.77 ± 1.26 (22.98-37.54) | 25.96 ± 1.32 (23.18-37.54) | 25.31 ± 0.98 (22.98-27.63) |
|
| ACD (mm) | 3.72 ± 0.27 (2.78-4.52) | 3.79 ± 0.25 (3.07-4.52) | 3.57 ± 0.25 (2.78-4.09) |
|
| LT (mm) | 3.62 ± 0.28 (2.90-5.21) | 3.51 ± 0.20 (2.90-4.01) | 3.89 ± 0.28 (3.32-5.21) |
|
| WTW (mm) | 12.08 ± 0.40 (11.1-13.3) | 12.14 ± 0.39 (11.2-13.3) | 11.95 ± 0.39 (11.1-13.0) |
|
| ECD (cells/mm2) | 2982.39 ± 227.22 (2261-3991) | 3007.51 ± 214.20 (2405-3904) | 2921.63 ± 246.53 (2261-3991) |
|
| CA (µm2) | 318.97 ± 25.03 (265.0-425.0) | 315.98 ± 23.44 (265-402) | 326.21 ± 27.30 (269-425) |
|
| CV (%) | 28.50 ± 4.49 (19.0-47.0) | 27.81 ± 4.40 (19.0-47.0) | 30.19 ± 4.28 (21.0-42.0) |
|
| HEX (%) | 65.14 ± 5.83 (29-82) | 65.42 ± 5.81 (48-82) | 64.44 ± 5.85 (29-75) | 0.127 |
| CCT (μm) | 547.72 ± 29.01 (468-629) | 548.97 ± 30.18 (468-629) | 544.69 ± 25.86 (485-606) | 0.181 |
| Variables | Univariate linear regression | Multivariate linear regression | ||||
|---|---|---|---|---|---|---|
| B | 95% CI |
| B | 95% CI |
| |
| Age | -6.28 | -9.48, -3.09 | <0.001 | -4.66 | -8.00, -1.33 | 0.006 |
| WTW | 88.02 | 32.38, 143.65 | 0.002 | 71.88 | 12.04, 131.72 | 0.019 |
| CCT | 1.12 | 0.35, 1.88 | 0.004 | 1.09 | 0.32, 1.87 | 0.006 |
| AL | 19.80 | 2.16, 37.43 | 0.028 | |||
| SE | -3.42 | -15.10, 8.26 | 0.566 | |||
| IOP | -5.61 | -13.38, 2.16 | 0.157 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal surgery and disorders · Ophthalmology and Visual Impairment Studies · Glaucoma and retinal disorders
Introduction
Myopia, a globally pervasive public health issue notably affecting East Asian youth, is anticipated to exceed 740 million cases worldwide by 2050 (1). Despite the escalating prevalence and severity of myopia, current clinical strategies lack fully effective, evidence-based interventions to comprehensively prevent its onset and progression (2). With advancing surgical techniques and growing demand for spectacle-free lifestyles, refractive procedures are experiencing rising adoption. In recent decades, phakic intraocular lens (pIOL) implantation has emerged as a viable therapeutic strategy within refractive surgical protocols, particularly for young adults requiring correction of high myopia, in whom deep excimer laser stromal ablation—necessary for large refractive errors—would increase the risk of postoperative corneal ectasia. However, growing concerns have been raised regarding the long-term safety of iris-claw pIOLs, particularly due to progressive endothelial cell loss (3, 4). Consequently, posterior chamber pIOLs appear to be the more favorable option (5).
While current evidence suggests minimal corneal endothelial impact from laser keratorefractive surgery (6), isolated cases of corneal decompensation have been reported in patients with preexisting endothelial pathology, such as Fuchs endothelial corneal dystrophy (FECD), manifested as central corneal guttata. For example, one case involved a 58-year-old woman with preoperative FECD who developed persistent corneal edema and vision loss following laser-assisted in situ keratomileusis (LASIK) (7), while another described a 47-year-old woman with asymptomatic guttata who experienced bilateral corneal decompensation post-LASIK (8). Additionally, Moshirfar et al. (9) reported a 12.4% decrease in endothelial cell density (ECD) and increased central corneal thickness one year after LASIK in eyes with corneal guttata. These findings underscore the importance of careful patient selection, as individuals with compromised endothelium may not be suitable candidates for laser vision correction. In light of the above, assessing endothelial morphometric parameters remains critical for risk stratification in pIOL implantation in young adults (10). Therefore, refractive surgeons should incorporate perioperative evaluation of endothelial functional integrity in all pIOL candidates and in keratorefractive surgery candidates who exhibit any abnormal endothelial findings on slit-lamp examination.
Although prior investigations have characterized corneal endothelial cell density and morphology in Chinese pediatric populations (11–13) and individuals over 40 years of age, both with or without myopia (14–16), a critical knowledge gap persists regarding corneal endothelial parameters and central corneal thickness (CCT) in myopic young Chinese adults, who constitute the predominant candidates undergoing refractive surgery. This retrospective cross-sectional study involved young myopic patients scheduled for refractive surgery at our hospital. During preoperative evaluations, we systematically gathered demographic data and ocular parameters. The findings offer valuable and detailed insights into the corneal characteristics of this surgical group.
Methods
Study design
This retrospective cross-sectional study was carried out at Wuxi Aier Eye Hospital, located in Jiangsu Province, China. Written informed consent was obtained from all participants prior to their inclusion in the study. The research adhered to the principles outlined in the Declaration of Helsinki and complied with the ARVO statement regarding human subjects. The study protocol received approval from the Institutional Review Board of Wuxi Aier Eye Hospital (Approval No. WXAE-ETH-2024-018).
Population and sample
We recruited candidates for refractive surgery from Wuxi Aier Eye Hospital, China, who were of Han Chinese ethnicity and aged 18 years or older. The inclusion criteria were as follows: (1) comprehensive preoperative ocular and systemic evaluations were completed; (2) spherical equivalent (SE) refractive error of ≤ -0.50D in each eye; and (3) best-corrected visual acuity (BCVA) of ≥ 20/20 in each eye. Exclusion criteria included: (1) anatomical abnormalities of the eye (such as corneal or ocular surface diseases, glaucoma, or uveitis); (2) a history of inflammation or infection (including active or past ocular infections); (3) a history of surgery or trauma (such as ocular trauma or prior intraocular or corneal procedures); (4) external factors that could interfere with results (e.g., contact lens usage within the past month or recent use of ocular medication); and (5) systemic diseases (including diabetes mellitus, autoimmune disorders, and others). When only one eye’s data from each participant was needed for statistical analysis, we used data from the right eyes to minimize potential confounding effects from high interocular correlation.
Data collection procedures
At the baseline assessment, all subjects underwent standardized preoperative evaluations, including comprehensive systemic and ocular examinations. Ocular biometric parameters were measured, with axial length (AL) assessed using the IOL Master 700 (Carl Zeiss Meditec AG, Germany; Ver. 1.90R38), and intraocular pressure (IOP) determined using the Nidek NT-510 tonometer (Nidek Co., Ltd., Japan). Corneal endothelial analysis was performed with the Nidek CEM-530 specular microscope (Nidek Co., Ltd., Japan), capturing parameters such as endothelial cell density (ECD), coefficient of variation (CV), average cell area (CA), and hexagonality percentage (HEX). Only sharply defined images, where the corneal endothelial cells were automatically delineated and analyzed, were deemed valid for examination. Additionally, central corneal thickness (CCT) and pupillary diameter were obtained using Scheimpflug tomography through the Pentacam HR system (Oculus Optikgeräte GmbH, Germany; Ver. 1.26r28) in a dimly lit examination room. The corneas with a CCT < 500 μm were screened for keratoconus using anterior and posterior elevation maps. All imaging procedures were carried out by a certified ophthalmic imaging specialist, adhering strictly to standardized protocols.
Data analysis
Continuous variables were expressed as the mean ± standard deviation (SD). The normality of their distributions was assessed using the one-sample Kolmogorov-Smirnov test prior to applying tests of significance. All continuous variables exhibited normal distributions, with the exceptions of age and IOP. Furthermore, the continuous variables refractive state and AL were categorized into subgroups. Refraction subgroups were stratified based on SE as follows: low myopia (-3.0D < SE ≤ -0.50D), moderate myopia (-6.0D < SE ≤ -3.0D), and high myopia (SE ≤ -6.0D). AL subgroups were classified as medium eyes (AL < 24.0 mm), medium-long eyes (24.0 mm ≤ AL < 26.0 mm), and long eyes (AL ≥ 26.0 mm). Besides, the participants were stratified into two age-based groups: those under 30 years of age and those aged 30 years or older. Besides, given the significant age difference between the male and female groups, analysis of covariance (ANCOVA) with age as a covariate was used to compare corneal parameters between genders.
A paired t-test was performed to compare parameters between the right and left eyes, while an independent Student’s t-test or Mann–Whitney U test was used to examine differences in continuous variables between age and gender groups, based on the normality of data distribution. One-way analysis of variance (ANOVA) with post hoc Bonferroni correction was conducted to compare examination parameters among patients grouped by SE and AL subgroups. The correlation between age and corneal parameters was analyzed using Spearman’s correlation coefficient. Associations between ocular parameters (SE or AL) and corneal metrics, including CCT and corneal endothelial characteristics (ECD, CV, CA, and HEX), were evaluated using Pearson’s correlation coefficient, with adjustments for age and gender.
Univariate linear regression was employed to assess the significance of associations between ECD and continuous variables: age, IOP, SE, AL, WTW, and CCT. Variables demonstrating significant associations (P < 0.05) with ECD were subsequently included in a multiple linear regression model. All statistical analyses were performed using SPSS 21.0 (SPSS Inc., Chicago, Illinois, USA), and statistical significance was defined as P < 0.05.
Results
The study included 400 participants (156 females and 244 males) with a mean age of 25.4 ± 6.9 years (range: 18–43 years). Table 1 details the demographic data and preoperative binocular status of the study population. The right eye demonstrated greater scotopic pupillary diameter, IOP, AL, and CA. In contrast, the left eye showed superior ECD, and CCT. Interocular comparisons revealed no statistically significant disparities in anterior chamber depth (ACD), lens thickness (LT), white-to-white measurement (WTW), CV, or HEX.
The mean values of the measured parameters, categorized by gender, are presented in Table 2. No statistically significant differences were found between genders in SE, CA, or ECD. However, notable gender-based variations were observed in several other parameters. Males showed higher values for AL, ACD, WTW, HEX, and CCT, whereas females exhibited greater values for LT and CV.
In Table 3, the subjects were classified into three groups based on AL: 22 medium eyes (AL < 24.0 mm), 220 medium-long eyes (24.0 mm ≤AL < 26.0 mm), and 158 long eyes (AL ≥ 26.0 mm). No statistically significant differences were detected in ECD or morphology parameters (CV, CA, HEX), or CCT.
In Table 4, participants were stratified into three refractive groups based on SE: low-myopia (-3.0D<SE≤-0.50D, n=50), moderate-myopia (-6.0D<SE≤-3.0D, n=220), and high-myopia (SE ≤ -6.0 D, n=158). Similar to AL-based grouping, no statistically significant differences were detected in ECD or morphology parameters (CV, CA, HEX), or CCT.
In Table 5, participants were stratified by age into two groups: <30 years and ≥30 years. No statistically significant differences were observed between the groups in SE, HEX, or CCT. The younger group exhibited higher ECD values but lower CA and CV values.
Significant negative correlations were observed between age and both ECD (r = -0.197, P < 0.001, Figure 1) and CCT (r = -0.111, P = 0.026), whereas positive correlations were identified with CA (r = 0.166, P = 0.001) and CV (r = 0.364, P < 0.001). Univariable linear regression analysis derived the following regression equation between ECD and age: ECD = 3141.91+(-6.281*age). After adjusting for age, ECD showed no significant association with SE (P = 0.662) or AL (P = 0.179) but exhibited a weak positive correlation with CCT (r = 0.128, P = 0.011).
Scatter plot showing a significant negative correlation between endothelial cell density (ECD) and age (r = -0.197, P < 0.001). Univariable linear regression analysis yielded the equation: ECD = 3141.91+(-6.281Age).*
Table 6 presents the results of both univariable and multivariable linear regression models for ECD. Four variables that showed a significant association with ECD in the univariable analysis were subsequently included in the multivariable model. In the multivariable linear regression analysis, three variables—age, WTW, and CCT—remained significantly associated with ECD.
Discussion
The evaluation of CCT, a key reference index for corneal refractive surgery, and ECD and morphology, critical indicators for intraocular refractive surgery, forms an essential component of refractive surgical practice. These parameters are pivotal for preoperative assessment and postoperative monitoring. Contemporary evidence, as delineated in a recent review, emphasizes that CCT modulation is governed by a multifactorial interplay of determinants, encompassing demographic variables (e.g., age, gender, and ethnicity), systemic comorbidities such as autoimmune diseases, and extrinsic environmental influences (17). As a result, the corneal parameter profiles of various populations undergoing refractive surgery merit further exploration. This study specifically examined young myopic patients of Han Chinese ethnicity residing in Wuxi, China.
Axial elongation in myopia may lead to “stretching” of ocular tissues, potentially including the corneal endothelium, which could result in decreased cell density or altered morphology. In the present study, no statistically significant differences in CCT or ECD and corneal endothelial morphology (CV, CA, HEX) were observed between subgroups categorized by AL or SE (Tables 3, 4). In comparison, Zhang et al. (16) recently reported that highly myopic eyes (axial length: 29.09 ± 2.33 mm) exhibited higher ECD (2730.76 ± 259.03 cells/mm^2^ vs. 2677.74 ± 240.93 cells/mm^2^) but greater pleomorphism and polymegathism compared to controls (axial length: 23.55 ± 1.00 mm) in an elderly cohort (mean age: 65.98 ± 9.83 years). Notably, they found no statistically significant differences in CCT between intergroup comparisons. Panda et al. (18) recently also reported no significant intergroup differences in CCT across 100 myopic, hyperopic, and emmetropic eyes, with no correlation observed between CCT and AL. These findings align with prior studies analyzing data from 150 right eyes of healthy young Egyptian adults (aged 20–30 years) (19) and 111 right eyes of myopic Chinese-Malaysian pediatric subjects (aged 8–9 years) (12).
However, Hafeez et al. (20) recently observed in their analysis of 129 myopic patients (aged 14–40 years) that ECD exhibited a more pronounced reduction in individuals with high myopia compared to those with low-to-moderate myopia. Interestingly, Mutwaly et al. (21) reported a graded relationship between myopia severity and CCT in a young Sudanese cohort (N = 160; aged 16–38 years), with CCT measurements decreasing progressively from low to high myopia, whereas ECD showed no significant intergroup variation across all myopia subgroups. While the associations between CCT or ECD and ametropia or axial length vary across studies, their relationship with age remains remarkably consistent in the literature. These findings further demonstrate that age serves as the primary determinant of ECD reduction in healthy population (22), while refractive error and axial elongation exert negligible effects on ECD or CCT. These results also support the notion that the anterior segment remains relatively stable during the process of ocular elongation in myopia (23). A progressive decline in ECD with advancing age was paralleled by corresponding reductions in CCT (14, 15, 24, 25), as corroborated by the observations in our study (Table 6).
Interestingly, we observed a significant association between WTW diameter and ECD in both univariable and multivariable linear regression models (Table 6). The theoretical basis for this association may stem from the embryological and anatomical relationship between corneal diameter and overall ocular dimensions. Larger WTW measurements typically correlate with greater corneal diameter. Given that ECD represents cell count per unit area, eyes with larger overall dimensions may exhibit distinct endothelial characteristics due to differential tangential stretching during ocular growth and development. Furthermore, WTW serves as a proxy for anterior segment size (26), which may influence endothelial cell distribution patterns and metabolic demands. Notably, WTW emerged as a significant independent predictor even after adjusting for age and CCT, suggesting a genuine anatomical association that warrants further investigation.
It is noteworthy that, while most studies have found no significant correlation between the degree of myopia or AL and ECD, the likelihood of morphological abnormalities in the corneal endothelium—such as guttata—tends to increase with higher degrees of myopia in both younger (21) and old populations (16). Consequently, when assessing ECD values, particular attention should be given to the morphological characteristics of the corneal endothelium, particularly in patients with high myopia or elongated eyes. The presence of guttata is a finding that can occasionally be observed in specular microscopy of young adults. The default software in currently available specular microscopy devices is not capable of automatically identifying guttata, as these systems do not yet incorporate artificial intelligence (AI) algorithms capable of labeling them (27). In the present study, images were not reviewed to confirm the absence of guttata, so this finding may have been missed in a number of cases (likely small), which could have had some impact on the results and represents a limitation of this study. Given the potential risks associated with undetected guttata, particularly in the context of post-refractive surgery corneal decompensation, we strongly recommend the incorporation of AI-assisted identification methods in future clinical protocols.
Additionally, young and middle-aged adults with refractive errors represent a key demographic for the use of corneal contact lenses. Although our study did not specifically investigate the effects of contact lens use on corneal parameters within the examined cohort, findings from previous research provide significant insights. Two recent studies have independently explored the impact of hard contact lenses (HCL) and soft contact lenses (SCL) on corneal endothelial cell density and morphology (28, 29). Ono et al. (28) revealed that prolonged use of HCL (>14 years) induces morphological alterations in the corneal endothelium, including polymegathism (reflected by increased CV) and polymorphism (evidenced by reduced HEX), while ECD remains unaffected. Furthermore, a subsequent study by Ono et al. (29) demonstrated that prolonged SCL wear (>1 year) induces alterations in both corneal endothelial morphology (elevated CV, diminished HEX) and reduced ECD. Given these findings, clinicians are advised to perform comprehensive baseline evaluations of corneal endothelial cell morphology and density before fitting contact lenses. Regular monitoring of endothelial integrity is essential for patients with a history of long-term use of both HCL and SCL (30). These results underscore the importance of meticulous preoperative assessment for individuals who have worn contact lenses extensively, especially in the context of refractive surgery. Particular attention should be directed toward evaluating ECD and morphological changes in this patient population.
Although this study primarily incorporates corneal data from the right eyes for final statistical analysis, the symmetry of corneal parameters between both eyes is also noteworthy. Our investigation revealed statistically significant increases in left-eye CCT (OS: 549.10 ± 29.00 μm vs. OD: 547.72 ± 29.01 μm; P < 0.001) and ECD (OS: 3004.61 ± 244.58 cells/mm^2^ vs. OD: 2982.39 ± 227.22 cells/mm^2^; P = 0.005), without significant interocular disparities in endothelial morphology (CV: P = 0.774; HEX: P = 0.209). Our findings align with a prior multicenter study involving 6,644 Chinese myopic patients (mean age 25.12 ± 5.44 years) (31) and a population-based study involving 5792 Russian subjects (mean age 58.8 ± 10.6 years) (32), which similarly reported significantly greater CCT in right eyes compared to right eyes. However, Kelekele et al. (33) observed no statistically significant interocular variations in ECD, HEX, or CCT parameters within their Congolese cohort (N = 278; mean age 38.9 ± 17.2 years). This absence of laterality was echoed in a Pakistani population study (N = 362; mean age 38.3 ± 10.2 years) by Shaikh and associates (25). These variations may reflect differences in sample size and demographic heterogeneity, particularly variations in racial composition. Although the interocular differences of CCT and ECD observed in our study are indeed statistically significant yet clinically negligible, the findings emphasize the importance of accounting for interocular corneal parameter differences when designing and interpreting large-scale population studies.
Ethnicity is undeniably an important clinical factor that may influence CCT or ECD. When comparing the CCT (547.72 ± 29.01 μm) and ECD (2982.39 ± 227.22 cells/mm²) values observed in our study with those reported in studies involving similar age groups (18–43 years), our findings are consistent with those of a study conducted on a larger cohort of young myopic patients in China (N = 1190; CCT: 539.2 ± 37.8 μm) (34). However, ECD was not reported in this study. Similarly, a study on Thai individuals, who also share an Asian ethnic background, reported CCT and ECD values in healthy participants of the same age group that are closely aligned with our results (35). In contrast, the CCT and ECD of Egyptians aged 20–30 years (CCT: 525.92 ± 46.83 μm; ECD: 2933.75 ± 345.92 cells/mm²) and 30–40 years (CCT: 518.65 ± 67.99 μm; ECD: 2693.57 ± 287.34 cells/mm²) revealed significantly lower values compared to our findings (24). Of interest, a study on young Turkish individuals (20–40 years) reported CCT values (550.3 ± 34.6 μm) that are generally consistent with ours, whereas their ECD values (2659 ± 283 cells/mm²) were found to be significantly lower (36).
Our findings revealed no statistically significant gender-based differences in ECD (ANCOVA, adjusting for age). However, male participants demonstrated significantly higher CCT measurements compared to females (550.34 ± 29.05 μm vs. 543.62 ± 28.57 μm; P = 0.031; ANCOVA, adjusting for age). These results are consistent with a previous study conducted on young myopia patients in China (34). Several studies have similarly reported no statistically significant gender-based differences in ECD or CCT among healthy populations in Egypt (24), Israel (37), and Sudan (21). Intriguingly, two population-based studies in Japan presented conflicting findings regarding ECD: one study reported higher endothelial cell density in males (38), while the other found superior values in females (22). Consequently, the current body of evidence remains inconclusive in identifying definitive gender-dependent variations in CCT or ECD. Previous studies have documented that male eyes are typically larger in overall dimensions, correlating with greater body stature and orbital development (39). Hormonal influences, particularly androgen-mediated differences in collagen synthesis and corneal biomechanics, may contribute to thicker corneas in males. Additionally, differences in lifestyle factors, occupational exposures, and possibly unmeasured variables such as hormonal status could influence these parameters (40).
This study has several limitations that warrant acknowledgment. First, the research employed a single-center, cross-sectional design with a relatively small sample size, which may restrict the generalizability of the findings. The single-center aspect could also introduce selection bias, as the characteristics of participants might reflect local demographic nuances rather than representing a broader population. Second, the study primarily concentrated on Chinese myopic adults aged 18 to 43 years. As a result, the corneal parameters observed may not accurately reflect other refractive status groups (such as hyperopes or emmetropes) or populations of differing ethnic backgrounds. Third, a major limitation was the inability to accurately document and analyze the specific duration of contact lens wear among participants. Previous research has shown that prolonged contact lens use can induce morphological changes in the cornea, highlighting the importance of this factor, which was unfortunately omitted from precise evaluation in this study. Lastly, a critical assessment in candidates for keratorefractive surgery is the determination of whether they may have suspicious or confirmatory signs of corneal ectasia, which is generally evaluated using corneal tomographers. In various studies, it has been found that between 4.1% and 17.5% of candidates for excimer laser refractive surgery are diagnosed with suspected keratoconus or keratoconus (41–43). In our study, 5.0% (20/400) of eyes showed thin pachymetry (less than 500 microns). Unfortunately, the database did not capture which of those eyes had tomographic signs of keratoconus (Pentacam HR), which also constitutes a limitation of the present research.
In conclusion, refractive errors and axial elongation do not significantly affect CCT, corneal endothelial cell density, or cell morphology in our cohort of refractive surgery candidates. However, age demonstrates a mild correlation with both CCT and ECD in this study group, which spans nearly two decades. Additionally, the potential influence of gender and ocular laterality on corneal parameters warrants careful assessment during preoperative evaluations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liang J Pu Y Chen J Liu M Ouyang B Jin Z . Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. (2025) 109:362–71. doi: 10.1136/bjo-2024-325427, PMID: 39317432 · doi ↗ · pubmed ↗
- 2Lawrenson JG Huntjens B Virgili G Ng S Dhakal R Downie LE . Interventions for myopia control in children: a living systematic review and network meta-analysis. Cochrane Database Syst Rev. (2025) 2:CD 014758. doi: 10.1002/14651858.CD 014758.pub 3, PMID: 39945354 PMC 11822883 · doi ↗ · pubmed ↗
- 3Galvis V Villamil JF Acuña MF Camacho PA Merayo-Lloves J Tello A . Long-term endothelial cell loss with the iris-claw intraocular phakic lenses (Artisan®). Graefe’s Arch Clin Exp Ophthalmol. (2019) 257:2775–87. doi: 10.1007/s 00417-019-04506-9, PMID: 31659458 · doi ↗ · pubmed ↗
- 4Li J Song LL Song H . Five-year clinical outcomes of rigid iris-fixated phakic intraocular lens in northern Chinese. Int Ophthalmol. (2022) 42:2551–61. doi: 10.1007/s 10792-022-02303-8, PMID: 35381897 · doi ↗ · pubmed ↗
- 5Kalra N Asif MI Bafna RK Sharma N Sinha R . Posterior chamber phakic intraocular lens implantation for refractive correction in corneal ectatic disorders: A review. J Refract Surg. (2021) 37:351–9. doi: 10.3928/1081597 X-20210115-03, PMID: 34044697 · doi ↗ · pubmed ↗
- 6Juda M Bedlinski M Roszkowska AM Wierzbowska J . Clinical evaluation of corneal endothelial parameters following laser refractive surgery in myopic eyes: A review. J Clin Med. (2024) 13:1665. doi: 10.3390/jcm 13061665, PMID: 38541890 PMC 10971698 · doi ↗ · pubmed ↗
- 7Vroman DT Solomon KD Holzer MP Peng Q Apple DJ Bowie EM . Endothelial decompensation after laser in situ keratomileusis. J Cataract Refract Surg. (2002) 28:2045–9. doi: 10.1016/s 0886-3350(01)01352-9, PMID: 12457684 · doi ↗ · pubmed ↗
- 8Dastjerdi MH Sugar A . Corneal decompensation after laser in situ keratomileusis in fuchs’ endothelial dystrophy. Cornea. (2003) 22:379–81. doi: 10.1097/00003226-200305000-00020, PMID: 12792486 · doi ↗ · pubmed ↗