Dietary index for gut microbiota is inversely associated with colorectal cancer risk: a case–control study
Qingzhen Song, Jing Lian, Yongjing Chen, Chuchu Shi, Peng Bu

TL;DR
A diet that supports gut microbiota is linked to a lower risk of colorectal cancer and better overall health.
Contribution
This study introduces a dietary index for gut microbiota and shows its inverse association with colorectal cancer risk.
Findings
CRC patients had significantly lower DI-GM scores than controls.
Higher DI-GM scores were associated with lower systemic inflammation and better psychosocial health.
Individuals with the highest DI-GM tertile had 68% lower odds of CRC.
Abstract
Gut microbial dysbiosis is a recognized contributor to colorectal cancer (CRC) development, with diet serving as a primary modifiable factor influencing microbiota composition. While previous research has largely focused on individual nutrients or the inflammatory potential of diet, few studies have investigated dietary patterns explicitly designed to support gut microbiota health in relation to CRC risk. In this case–control study, 350 adults (175 newly diagnosed CRC patients and 175 age- and sex-matched controls) were recruited. Dietary intake was assessed using multiple 24-h recalls and a validated food-frequency questionnaire to calculate the Dietary Index for Gut Microbiota (DI-GM), which emphasizes prebiotic fibers, polyphenols, fermented foods, fruits, vegetables, legumes, and whole grains, while penalizing ultra-processed and pro-inflammatory foods. Anthropometric, lifestyle,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
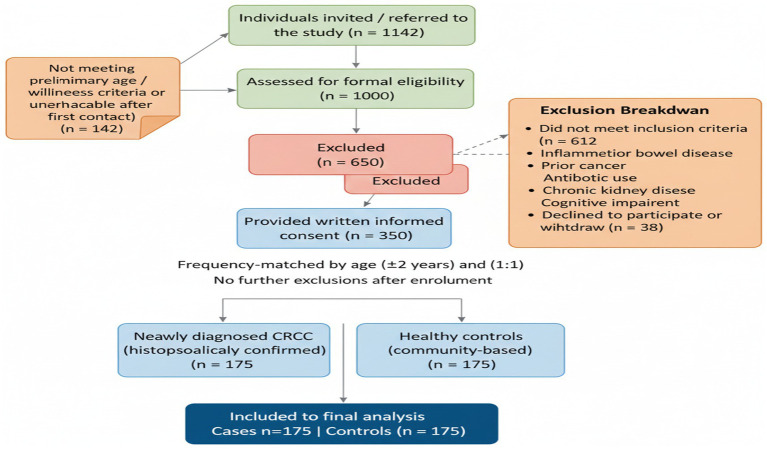 Figure 1
Figure 1| Variable | Case ( | Control ( | |
|---|---|---|---|
| Age, years | 59.59 ± 1.09 | 59.56 ± 1.10 | 0.808 |
| DI-GM Score | 7.29 ± 2.70 | 11.34 ± 2.55 | <0.001 |
| BMI, kg/m2 | 26.43 ± 4.65 | 24.86 ± 1.62 | <0.001 |
| Sex, male, n (%) | 91 (51) | 88 (49) | 0.415 |
| Smoking, n (%) | 39 (22) | 25 (14) | 0.036 |
| Alcohol drinking, n (%) | 43 (24.5) | 26 (15) | 0.016 |
| Socio-Economic Status, n (%) | 0.519 | ||
| Low | 68 (19.5) | 75 (21.5) | |
| Medium | 61 (17.5) | 71 (20.3) | |
| High | 39 (11.2) | 35 (10) | |
| Physical activity (total MET), MET | 16.07 ± 7.99 | 21.71 ± 7.86 | <0.001 |
| CRP, mg/L | 4.84 ± 1.44 | 2.70 ± 1.37 | <0.001 |
| IL-6, pg./mL | 4.71 ± 1.34 | 2.97 ± 1.08 | <0.001 |
| Hemoglobin, g/dL | 11.78 ± 1.78 | 13.07 ± 1.80 | <0.001 |
| WBC, ×103/μL | 7.71 ± 0.96 | 6.52 ± 0.84 | <0.001 |
| NLR | 3.35 ± 0.86 | 1.96 ± 0.91 | <0.001 |
| Platelets, ×103/μL | 295.79 ± 45.69 | 259.15 ± 26.12 | <0.001 |
| Albumin, g/dL | 3.50 ± 0.48 | 4.03 ± 0.39 | <0.001 |
| HbA1c, % | 5.66 ± 1.19 | 5.47 ± 0.56 | 0.052 |
| PHQ-9, score | 11.95 ± 4.42 | 9.63 ± 4.14 | <0.001 |
| PSQI, score | 9.90 ± 3.60 | 8.06 ± 3.43 | <0.001 |
| Insulin, μIU/mL | 17.29 ± 7.65 | 12.53 ± 7.50 | <0.001 |
| HOMA-IR | 4.84 ± 2.23 | 3.25 ± 2.25 | <0.001 |
| Energy, kcal/day | 1939.40 ± 242.67 | 1973.17 ± 255.64 | 0.207 |
| Fiber, g/day | 15.4 ± 6.95 | 18.42 ± 8.34 | 0.381 |
| Carbs, g/day | 274.69 ± 19.84 | 276.63 ± 21.21 | 0.378 |
| Protein, g/day | 61.20 ± 13.32 | 63.09 ± 14.21 | 0.201 |
| Fat, g/day | 66.21 ± 13.81 | 68.26 ± 14.14 | 0.172 |
| Systolic BP, mmHg | 127.61 ± 8.36 | 129.43 ± 8.15 | 0.040 |
| Diastolic BP, mmHg | 81.63 ± 4.16 | 82.38 ± 4.28 | 0.098 |
| Glucose, mg/dL | 91.06 ± 4.32 | 91.81 ± 4.41 | 0.110 |
| HDL, mg/dL | 45.72 ± 7.01 | 44.51 ± 6.95 | 0.105 |
| TG, mg/dL | 129.83 ± 4.86 | 130.14 ± 5.24 | 0.567 |
| LDL, mg/dL | 94.83 ± 6.66 | 95.83 ± 6.82 | 0.164 |
| Cholesterol, mg/dL | 185.98 ± 11.68 | 187.78 ± 11.95 | 0.156 |
| Variable | Tertile 1 | Tertile 2 | Tertile 3 | Tertile 1 | Tertile 2 | Tertile 3 | ||
|---|---|---|---|---|---|---|---|---|
| Case group ( | Control group ( | |||||||
| CRP (mg/L) | 5.65 ± 0.82 | 4.03 ± 1.34 | 1.90 ± 0.50 | <0.001 | 5.38 ± 0.18 | 3.16 ± 1.40 | 1.92 ± 0.15 | <0.001 |
| IL-6 (pg/mL) | 5.39 ± 1.08 | 4.01 ± 1.06 | 2.30 ± 0.50 | <0.001 | 5.14 ± 0.10 | 3.31 ± 1.07 | 2.35 ± 0.12 | <0.001 |
| Zonulin (ng/mL) | 57.1 ± 22.38 | 57.7 ± 18.26 | 31.4 ± 0.54 | 0.006 | 69.3 ± 0.78 | 50.3 ± 20.17 | 39.0 ± 16.00 | <0.001 |
| FCP (μg/g) | 97.0 ± 39.54 | 94.7 ± 36.43 | 41.1 ± 1.07 | 0.001 | 119.4 ± 2.38 | 80.3 ± 40.30 | 58.5 ± 32.39 | <0.001 |
| TNF-α (pg/mL) | 22.5 ± 8.96 | 20.4 ± 7.24 | 9.43 ± 0.53 | <0.001 | 24.9 ± 0.71 | 17.7 ± 7.95 | 13.1 ± 6.09 | <0.001 |
| PHQ-9 | 12.4 ± 4.68 | 12.0 ± 3.92 | 6.57 ± 0.53 | <0.001 | 14.6 ± 0.49 | 10.6 ± 4.45 | 8.15 ± 3.42 | <0.001 |
| PSQI | 10.3 ± 3.86 | 9.8 ± 3.12 | 5.57 ± 0.53 | 0.003 | 12.1 ± 0.68 | 8.9 ± 3.75 | 6.8 ± 2.82 | <0.001 |
| Frailty Index | 2.75 ± 0.16 | 1.98 ± 0.60 | 1.00 ± 0.2 | <0.001 | – | – | – | – |
| CEA (ng/mL) | 4.65 ± 2.99 | 5.15 ± 3.18 | 6.20 ± 2.85 | 0.314 | – | – | – | – |
| CA19-9 (U/mL) | 29.9 ± 23.58 | 34.2 ± 25.68 | 44.0 ± 22.32 | 0.232 | – | – | – | – |
| Variable | Model 1a: B (95% CI) | Model 2b: B (95% CI) | Model 3c: B (95% CI) | |||
|---|---|---|---|---|---|---|
| CRP (mg/dL) | −1.87 (−1.89, −1.85) | <0.001 | −1.89 (−1.91, −1.88) | <0.001 | −1.90 (−2.35, −1.88) | <0.001 |
| IL-6 (pg/mL) | −2.19 (−2.23, −2.16) | <0.001 | −2.20 (−2.23, −2.18) | <0.001 | −2.20 (−2.23, −2.18) | <0.001 |
| TNF-α (pg/mL) | −0.26 (−0.30, −0.23) | <0.001 | −0.26 (−0.30, −0.23) | <0.001 | −0.27 (−0.30, −0.23) | <0.001 |
| Zonulin (ng/mL) | −0.08 (−0.09, −0.06) | <0.001 | −0.10 (−0.12, −0.08) | <0.001 | −0.11 (−0.12, −0.09) | <0.001 |
| Frailty Index | −3.91 (−4.21, −3.62) | <0.001 | −4.25 (−4.38, −4.12) | <0.001 | −4.27 (−4.40, −4.14) | <0.001 |
| PHQ-9 (Score) | −0.37 (−0.44, −0.30) | <0.001 | −0.47 (−0.56, −0.39) | <0.001 | −0.48 (−0.57, −0.40) | <0.001 |
| Variable | OR (95% CI)—crude model | Model 1a | Model 2a | P for trend* |
|---|---|---|---|---|
| DI-GM tertiles | <0.001 | |||
| Tertile 1 (Low) | Reference | Reference | Reference | |
| Tertile 2 (Moderate) | 0.55 (0.34–0.89) | 0.52 (0.31–0.87) | 0.50 (0.30–0.84) | |
| Tertile 3 (High) | 0.38 (0.23–0.63) | 0.34 (0.20–0.58) | 0.32 (0.19–0.55) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGut microbiota and health · Nutritional Studies and Diet · Probiotics and Fermented Foods
Introduction
Colorectal cancer (CRC) continues to be one of the most prevalent causes of cancer-related illness and death globally, with its occurrence increasing in various parts of the world (1). Accumulating evidence has implicated gut microbiota dysbiosis—characterized by altered microbial diversity and composition—in the pathogenesis of CRC (2). The gut microbiota exerts a profound influence on host metabolic processes, immune function, and intestinal barrier integrity, all of which are critical determinants in colorectal carcinogenesis (3, 4). Consequently, interventions targeting the modulation of gut microbial communities have gained increasing attention as potential strategies for CRC prevention and management (5).
Diet is recognized as one of the most influential and modifiable factors shaping the gut microbiota (6). Diets high in prebiotic fibers, polyphenols, fermented foods, whole grains, legumes, fruits, and vegetables foster the growth of beneficial microbes and promote the production of short-chain fatty acids (SCFAs), which have demonstrated anti-inflammatory, immunomodulatory, and antineoplastic properties (7, 8). Conversely, diets rich in ultra-processed foods and pro-inflammatory components have been linked to gut microbial dysbiosis, systemic inflammation, and elevated cancer risk (9, 10). Several dietary indices, such as the Dietary Inflammatory Index (DII) and Mediterranean diet, have been developed and shown to predict inflammation-related cancer risk, including CRC (11–13).
Despite these advances, most prior research has focused on the inflammatory potential of diet or isolated nutrients rather than comprehensive dietary patterns explicitly designed to promote gut microbiota health (14–16). Moreover, few studies have integrated assessments of gut microbial diversity, intestinal permeability, metabolic biomarkers, psychological health, and frailty status in relation to diet and cancer risk (17). This leaves a critical knowledge gap in understanding the multifactorial pathways linking gut microbiota-supportive diets to colorectal carcinogenesis.
To address these gaps, the Dietary Index for Gut Microbiota (DI-GM) is an a priori literature-derived dietary score designed to quantify adherence to a microbiota-supportive diet based on known effects of foods on microbial diversity, fermentation capacity, and intestinal barrier integrity (18). Using a case–control design, we investigated (1) the association between DI-GM and CRC risk and (2) the relationships between DI-GM and multidimensional biomarkers—including inflammatory markers, intestinal permeability, metabolic factors, frailty, depression, and sleep quality. This integrative approach provides a more comprehensive understanding of how microbiota-targeted diet as quantified by the DI-GM dietary index may influence CRC risk.
Methods
Study design and participants
This case–control study was conducted to examine the association between adherence to a microbiota-targeted diet as quantified by the DI-GM dietary index and CRC risk. A total of 350 adults aged 40–75 years were recruited, including 175 newly diagnosed CRC patients (cases) and 175 healthy controls selected using frequency matching based on age and sex. Cases were confirmed by histopathological diagnosis at Shanxi Cancer Hospital, ensuring all diagnoses met standardized oncological criteria. All CRC patients were enrolled within 2 weeks of histopathological diagnosis and prior to treatment. Controls were recruited from the same geographical area through community health screenings and matched by frequency to cases by age (±2 years) and sex to minimize confounding. Control participants were excluded if they had a history of colorectal cancer or any other malignancy, inflammatory bowel diseases (such as ulcerative colitis or Crohn’s disease), recent gastrointestinal infections or antibiotic use within the past 3 months, chronic autoimmune or systemic inflammatory disorders, or any major chronic diseases that could influence gut microbiota composition or dietary patterns (including, liver cirrhosis, chronic kidney disease, or uncontrolled diabetes). Participants with colorectal polyps, adenomatous lesions, or dysplasia without invasive carcinoma were excluded. Additionally, controls with significant cognitive impairment or inability to provide informed consent were excluded to ensure the reliability of dietary and lifestyle data collection. Exclusion criteria for case group included prior cancer diagnosis, inflammatory bowel disease, recent antibiotic or probiotic use (within 3 months), major chronic illnesses affecting diet or microbiota (e.g., chronic kidney disease, autoimmune disorders), and inability to provide informed consent. Figure 1 provides a step-by-step schematic representation of participant screening, application of inclusion and exclusion criteria, confirmation of newly diagnosed CRC prior to treatment, frequency matching of controls by age and sex, and the final allocation of participants included in the statistical analyses.
Flowchart illustrating participant recruitment, eligibility assessment, exclusion criteria, and final inclusion of colorectal cancer cases and frequency-matched controls in the case control study.
Sample size calculation
Sample size was determined a priori using logistic regression power calculations to detect an odds ratio of ≤0.58 for colorectal cancer when comparing the highest versus lowest tertile of the Dietary Index for Gut Microbiota (DI-GM), assuming equal-sized case and control groups, two-sided α = 0.05, and 80% power; this yielded a minimum requirement of approximately 150 participants per group. To accommodate potential missing data and to ensure sufficient power for stratified analyses, we enrolled 175 newly diagnosed CRC cases and 175 age- and sex-matched healthy controls (total n = 350). A post-hoc power analysis based on the observed fully adjusted odds ratio of 0.32 (95% CI 0.19–0.55) for the highest versus lowest DI-GM tertile confirmed >99.9% power, verifying that the achieved sample size was more than adequate for the primary study objective (13).
Ethical considerations
The study protocol was approved by the Institutional Review Board of Shanxi Cancer Hospital (Approval No. 20258LL2550). All participants provided written informed consent prior to enrollment, and all procedures adhered strictly to the principles outlined in the Declaration of Helsinki and relevant national guidelines.
Dietary assessment and DI-GM score calculation
Dietary intake was assessed using three 24-h dietary recalls (two weekdays and one weekend day) conducted on three non-consecutive days including two weekdays and one weekend day to capture typical dietary variation, administered by trained dietitians using standardized multi-pass interview methods. Additionally, a validated semi-quantitative food frequency questionnaire (FFQ) covering habitual intake over the preceding 12 months was administered to capture longer-term dietary patterns (19). Using both recalls and FFQ captured short-term intake variability and habitual long-term diet, reducing measurement error. Nutrient and food group intakes were calculated using comprehensive food composition tables, incorporating local food items and adjustments for preparation methods. The daily nutrient intake for each subject was calculated using the Chinese Food Composition Table. Implausible energy reporters were assessed using the Goldberg cut-off method; none met exclusion criteria (20).
The DI-GM was developed to reflect adherence to a dietary pattern supportive of gut microbiota health (18). The index incorporated intakes of prebiotic fibers, polyphenols, fermented foods, whole grains, legumes, fruits, and vegetables, scored positively based on consumption frequency and quantity. Conversely, consumption of ultra-processed and pro-inflammatory foods—including refined sugars, red and processed meats, and trans fats—was penalized. Each dietary component was weighted according to its established effect on gut microbial modulation in the literature, and individual scores were standardized before summation to generate a composite DI-GM score, with higher scores indicating greater adherence to microbiota-supportive diet.
Anthropometric and lifestyle data
Measurements followed ISAK guidelines. Weight was measured with a Seca 813 scale and height with a Seca 217 stadiometer. BMI was calculated as kg/m^2^ and classified using WHO cut-offs. Physical activity was assessed using the IPAQ (21).
Clinical and biochemical measurements
Fasting venous blood samples were collected in the morning following an overnight fast of at least 10 h. Serum and plasma were separated by centrifugation at 3000 rpm for 10 min and stored at −80 °C until analysis. Systemic inflammatory markers, including high-sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6), were quantified using enzyme-linked immunosorbent assays (ELISA) with commercially available kits from Wuhan Fine Biotech Co., Ltd. (Wuhan, China) and R&D Systems China, both validated for clinical research and demonstrating high sensitivity and specificity in previous studies. Additional laboratory parameters, including complete blood count (CBC), fasting insulin, and glucose, were measured using standardized automated analyzers (e.g., Sysmex XN-1000, Roche Cobas 6,000), following rigorous internal and external quality control protocols to ensure accuracy and reproducibility. The ELISA assays were performed according to manufacturers’ protocols, with all samples and standards run in duplicate to minimize analytical variability. Tumor stage at diagnosis was recorded from pathology reports according to the TNM classification (Stage I–IV).
Frailty assessment
Frailty status was assessed using the modified five-item frailty index (mFI-5), which incorporates comorbidities (e.g., diabetes, hypertension), functional status, and other clinically relevant parameters. The index has been validated in oncologic and general populations and was administered via patient interview and medical record review. Higher scores indicate greater frailty and vulnerability to adverse outcomes (22).
Psychological assessments
Depressive symptoms were evaluated via the Patient Health Questionnaire-9 (PHQ-9), a widely validated self-administered instrument that assesses the severity of depression over the past 2 weeks. The PHQ-9 is a 9-item questionnaire, with each item rated on a scale from 0 to 3, producing a cumulative score between 0 and 27. Elevated scores reflect increased severity of depressive symptoms, with recognized thresholds categorizing depression as minimal, mild, moderate, or severe. This tool has shown high reliability and validity in various populations, including individuals diagnosed with cancer (23).
Sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI), a generally used self-administered questionnaire designed to assess perceived sleep quality and related disturbances over the preceding month. The PSQI comprises 19 items, organized into 7 components—such as sleep onset latency, efficiency, sleep duration, and daytime impairment. Each component is scored from 0 to 3, contributing to a total global score ranging from 0 to 21, with higher scores reflecting poorer sleep quality. A global score exceeding 5 typically signifies a clinically meaningful sleep disturbance. The PSQI has been extensively validated and is frequently employed in both clinical practice and research, including among cancer patients (24).
Statistical analysis
All statistical analyses were conducted using Stata version 14. Statistical significance was defined as a two-sided p-value < 0.05. Baseline characteristics were summarized as means ± standard deviations for continuous variables and counts with percentages for categorical variables. Normality assumptions were evaluated using the Shapiro–Wilk test. Between-group differences (cases vs. controls) were tested using independent samples t-tests or Mann–Whitney U tests for non-normally distributed variables, and chi-square tests for categorical variables. Participants were categorized into tertiles based on the distribution of DI-GM scores in the total sample. To evaluate the association between DI-GM tertiles and CRC risk, logistic regression analyses were conducted to calculate odds ratios (ORs) and corresponding 95% confidence intervals (CIs), using the lowest tertile as the reference category. Tests for linear trend were conducted by modeling the median value of each tertile as a continuous variable. Linear regression analyses were performed to assess the associations between DI-GM scores (continuous and tertiles) and biomarkers of inflammation, intestinal permeability, metabolic status, psychological health, and frailty. All models included adjustment for relevant covariates, including sociodemographic factors and lifestyle behaviors.
Results
Baseline characteristics of participants
Baseline characteristics of contributors, categorized by case and control groups, are summarized in Table 1. The mean age of participants was similar between cancer patients (cases) and healthy controls (59.59 ± 1.09 vs. 59.56 ± 1.10 years; p = 0.808). However, the mean DI-GM score was significantly lower in cancer cases compared to controls (7.29 ± 2.7 vs.11.34 ± 2.55; p < 0.001), suggesting poorer dietary quality in the case group. Cases also had significantly higher BMI (26.43 ± 4.65 vs. 24.86 ± 1.62 kg/m^2^; p < 0.001), greater prevalence of smoking (p = 0.036) and alcohol use (p = 0.016), and lower levels of physical activity (16.07 ± 7.99 vs. 21.71 ± 7.86 METs; p < 0.001).
Markers of systemic inflammation including CRP (4.84 ± 1.44 vs. 2.70 ± 1.37 mg/L; p < 0.001) and IL-6 (4.71 ± 1.34 vs. 2.97 ± 1.08 pg./mL; p < 0.001) were significantly elevated in the case group.
Furthermore, cases exhibited poorer metabolic and clinical profiles, including lower hemoglobin (11.78 ± 1.78 vs. 13.07 ± 1.80 g/dL; p < 0.001), higher WBC counts (7.71 ± 0.96 vs. 6.52 ± 0.84 × 10^3^/μL; p < 0.001), elevated NLR (3.35 ± 0.86 vs. 1.96 ± 0.91; p < 0.001), higher platelet counts, and reduced albumin levels. Psychological and metabolic indicators such as PHQ-9, PSQI, insulin, and HOMA-IR were also significantly poorer among cancer patients. Dietary intake of macronutrients did not significantly differ between groups.
Among CRC patients, 28 (16.0%) were classified as Stage I, 46 (26.3%) as Stage II, 61 (34.9%) as Stage III, and 40 (22.9%) as Stage IV at diagnosis. DI-GM scores did not differ significantly across tumor stages (p = 0.41; Supplementary Table S1).
Association of DI-GM tertiles with biomarkers
Table 2 shows the distribution of inflammatory, microbial, and psychological biomarkers across tertiles of the DI-GM score, stratified by case–control status. In both groups, higher DI-GM tertiles were associated with significantly lower levels of inflammatory markers (CRP, IL-6, TNF-α), intestinal permeability markers (Zonulin, FCP), and psychological distress (PHQ-9, PSQI; p < 0.001 for all).
Among cancer patients, CRP levels decreased progressively from 5.65 ± 0.82 mg/L in the lowest DI-GM tertile to 1.90 ± 0.5 mg/L in the highest (p < 0.001). A similar trend was observed for IL-6 (5.39 ± 1.08 to 2.30 ± 0.5 pg./mL), and TNF-α. Notably, the frailty index was significantly lower in the highest tertile compared to the lowest (2.75 ± 0.16 vs. 1.00 0.5; p < 0.001).
Comparable trends were observed in the control group. For example, IL-6 decreased from 5.14 ± 0.10 pg./mL in the lowest tertile to 2.35 ± 0.12 pg./mL in the highest (p < 0.001), and PHQ-9 scores declined from 14.6 ± 0.49 to 8.15 ± 3.42 (p < 0.001). This indicates a robust dose–response relationship between DI-GM and multiple health indicators in both groups.
Multivariate associations between DI-GM and clinical biomarkers
As shown in Table 3, multivariable linear regression analysis among cancer patients revealed that higher DI-GM scores were strongly and independently associated with favorable inflammatory and clinical profiles. In the fully adjusted model (Model 3), each unit increase in DI-GM was associated with significant reductions in CRP (B = −1.90; 95% CI: −2.35, −1.88; p < 0.001), IL-6 (B = −2.20; 95% CI: −2.23, −2.18; p < 0.001), TNF-α (B = −0.27; 95% CI: −0.30, −0.23; p < 0.001), and Zonulin (B = −0.11; 95% CI: −0.12, −0.09; p < 0.001).
Additionally, higher DI-GM was significantly associated with lower frailty scores (B = −4.27; 95% CI: −4.40, −4.14; p < 0.001) and PHQ-9 scores (B = −0.48; 95% CI: −0.57, −0.40; p < 0.001), independent of demographic and dietary confounders.
Association between DI-GM score and Cancer risk
Table 4 presents the association between DI-GM tertiles and colorectal cancer risk. In the crude model, participants in the highest DI-GM tertile had 62% lower odds of CRC compared with those in the lowest tertile (OR = 0.38, 95% CI 0.23–0.63). After adjustment for age, sex, and BMI (Model 1), the OR was 0.34 (95% CI 0.20–0.58). In the fully adjusted model (Model 2) that additionally controlled for total energy intake, carbohydrate intake, and protein intake, individuals in the highest tertile showed 68% lower odds of colorectal cancer (OR = 0.32, 95% CI 0.19–0.55) compared with the lowest tertile. A significant dose–response relationship was observed across tertiles (P for trend < 0.001).
Discussion
This study demonstrates that adherence to a gut microbiota-supportive dietary pattern—as quantified by the DI-GM—is strongly associated with reduced CRC risk and with favorable inflammatory, microbial, metabolic, psychological, and frailty profiles. The magnitude of the association (68% lower odds for highest vs. lowest tertiles) is comparable to or stronger than associations reported for the Mediterranean and other plant-forward diets.
A recent large-scale prospective cohort study by Li et al. reported an inverse association between the DI-GM and the risk of gastrointestinal cancers (25). While that study provided important epidemiological evidence, our investigation differs substantially in three aspects. First, we focused exclusively on colorectal cancer rather than gastrointestinal cancers as a group, allowing disease-specific interpretation. Second, we incorporated detailed inflammatory, microbial, intestinal permeability, psychological, and frailty assessments in newly diagnosed patients prior to treatment, providing mechanistic insight beyond risk association. These elements extend prior findings and highlight the multi-system relevance of microbiota-supportive diets in CRC. Our findings are consistent with emerging evidence that suggests diet-mediated modulation of the gut microbiota plays a critical role in cancer prevention and overall systemic health (11–13). Specifically, individuals with higher DI-GM scores demonstrated significantly lower levels of pro-inflammatory biomarkers, including CRP, IL-6, TNF-α, and Zonulin. This finding is particularly important as it indicates that dietary patterns can influence systemic inflammation, which is a known risk factor for various chronic diseases, including cancer (26). This observation aligns with prior research demonstrating that diets rich in dietary fiber and polyphenols can effectively reduce inflammation through the production of short-chain fatty acids (SCFAs) (27). SCFAs inhibit the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway, which is instrumental in reducing pro-inflammatory cytokines (28, 29).
Psychological outcomes, such as depression and sleep quality, also exhibited a significant inverse relationship with DI-GM scores. This finding is consistent with the proposed mechanisms of the gut brain axis, suggesting that gut health can influence mental health outcomes (30, 31). This connection highlights the multifaceted nature of health, where dietary choices not only affect physical health but also mental well-being (26, 32, 33). Our findings resonate with previous studies that have linked dietary patterns that promote microbial balance to diminished depressive symptoms. This effect may occur through the modulation of tryptophan metabolism, immune signaling pathways, and the vagus nerve (34). Additionally, the inverse association between DI-GM scores and the frailty index further indicates that interactions between diet and microbiota may significantly impact physical resilience in cancer patients. This suggests that dietary interventions could play a crucial role in enhancing the overall quality of life for cancer patients by improving both their physical and psychological health.
Importantly, in this case–control study of 350 Chinese adults, higher adherence to a gut microbiota-supportive dietary pattern, as reflected by higher DI-GM scores, was independently associated with substantially lower odds of colorectal cancer. Participants in the highest tertile of DI-GM had 68% lower odds of CRC (fully adjusted OR = 0.32, 95% CI 0.19–0.55; P for trend < 0.001) compared with those in the lowest tertile. This association remained robust after adjustment for age, sex, BMI, total energy intake, and macronutrient composition, and represents one of the strongest protective dietary associations reported for colorectal cancer to date, comparable in magnitude to high adherence to the Mediterranean or plant-based dietary patterns in previous meta-analyses. To our knowledge, the first CRC-specific study integrating to demonstrate such a pronounced inverse association between a microbiota-focused dietary index and cancer risk in a human population. No association was observed between DI-GM and tumor stage, suggesting that microbiota-supportive dietary habits may be more strongly related to CRC risk than to disease severity at the time of diagnosis. These findings suggest that dietary patterns that promote a healthy gut microbiota may serve as a modifiable protective factor in cancer prevention and survivorship strategies. Our results are consistent with prior research showing that diets rich in fiber, polyphenols, and fermented foods—such as the Mediterranean or MIND diets—are linked to a lower risk of gastrointestinal malignancies (11–13). Furthermore, several recent studies (2024–2025) reinforce the protective effects of high-quality, anti-inflammatory, or microbiota-supportive dietary patterns against CRC and gastrointestinal (GI) cancers, while contrasting them with risks from Western-style or pro-inflammatory diets. For example, a 2025 NHANES analysis showed higher adherence to the Healthy Eating Index-2020 (HEI-2020) and alternative Mediterranean Diet (aMED) scores linked to reduce GI cancer risk, highlighting overall diet quality’s role in prevention (35). A 2022 EPIC-Spain cohort found suggestive increased CRC risk with Western patterns (especially in females and rectal subsite) and protective trends with Mediterranean adherence (particularly early follow-up and distal colon), with limited Prudent pattern effects (36). The 2024 review by Adolph and Tilg connects Western diets to gut microbial dysbiosis, chronic inflammation, and elevated risks of malignancies including CRC, emphasizing the harms of processed foods and low microbiota-supportive elements (37).
Prospective evidence using DI-GM (analogous to ours) further supports microbiota-targeted approaches: a 2025 UK Biobank gene-diet study (n = 178,148; median 13.47-year follow-up) reported higher DI-GM associated with lower GI cancer risk (HR 0.84 for CRC in highest vs. lowest category; HR 0.83 overall GI cancer), with stronger effects in lower genetic risk groups and significant DI-GM–genetic risk interaction (25). Broader systematic reviews, such as the Global Cancer Update Program (CUP Global, 2025), graded limited-suggestive evidence for lower CRC risk with higher alignment to a priori patterns like Mediterranean, healthful plant-based, Healthy Eating Index (HEI)/alternate HEI, and DASH, versus strong-probable increased risk from hyperinsulinemic (EDIH) or proinflammatory (EDIP) patterns (especially colon). A large prospective Study (n = 542,778 women; 12,251 CRC cases over ~16.6 years;) identified strong inverse associations with calcium intake (RR 0.83 per 300 mg/day) and dairy-related factors, alongside positive links to red/processed meat (RR 1.08 per 30 g/day) and alcohol, reinforcing calcium’s protective role (largely driving dairy benefits) and risks from less favorable patterns (38).
However, unlike previous studies, the DI-GM specifically integrates dietary components known to modulate microbial diversity and function, thereby offering a more targeted approach to gut-mediated cancer prevention. Mechanistically, the protective effect of a high DI-GM score may be explained, in part, by enhanced microbial production of short-chain fatty acids (SCFAs), such as butyrate and propionate, which have been shown to exert anti-inflammatory, anti-proliferative, and epigenetic effects on colonocytes (39, 40). In addition, a higher DI-GM score may contribute to better gut barrier function and immune regulation—both critical in mitigating tumorigenesis—potentially through modulation of the gut microbiota.
However, it is essential to acknowledge certain limitations of this study. First, the case–control design inherently carries the risk of reverse causation and recall bias, which must be considered. Although we used multiple 24-h recalls and FFQs to minimize recall bias, the diagnosis of CRC may influence patients’ recall of past dietary habits. Because of the cross-sectional case–control design, temporal relationships and mediation pathways cannot be established. Second, despite adjusting for multiple demographic and lifestyle factors, we cannot completely rule out residual confounding from unmeasured or unknown variables, such as socioeconomic status, genetic predisposition, or specific medication use (e.g., chronic PPI use) that could influence both diet and CRC risk. Additionally, we cannot establish a causal link. Finally, dietary intake was self-reported, which is susceptible to recall bias, potentially affecting the accuracy of our findings. Addressing these limitations in future research will be crucial for validating our findings and enhancing the reliability of dietary recommendations. Future longitudinal and intervention studies are needed to formally evaluate potential biological pathways linking microbiota-targeted dietary patterns and colorectal carcinogenesis.
Conclusion
Higher adherence to a gut microbiota-supportive dietary pattern—reflected by higher DI-GM scores—is associated with significantly lower CRC risk, reduced systemic inflammation, enhanced gut barrier integrity, and better psychosocial outcomes. These findings underscore the potential of microbiota-focused dietary interventions as feasible, modifiable strategies to reduce CRC risk and improve overall health. Prospective cohort studies and randomized dietary trials are warranted to establish causality and inform clinical translation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, 38572751 · doi ↗ · pubmed ↗
- 2Fan X Jin Y Chen G Ma X Zhang L. Gut microbiota dysbiosis drives the development of colorectal cancer. Digestion. (2021) 102:508–15. doi: 10.1159/000508328, 32932258 · doi ↗ · pubmed ↗
- 3Fernandes MR Aggarwal P Costa RGF Cole AM Trinchieri G. Targeting the gut microbiota for cancer therapy. Nat Rev Cancer. (2022) 22:703–22. doi: 10.1038/s 41568-022-00513-x, 36253536 · doi ↗ · pubmed ↗
- 4Priego-Parra BA Remes-Troche JM. Bidirectional relationship between gastrointestinal cancer and depression: the key is in the microbiota-gut-brain axis. World J Gastroenterol. (2024) 30:5104–10. doi: 10.3748/wjg.v 30.i 48.5104, 39735265 PMC 11612697 · doi ↗ · pubmed ↗
- 5Baima G Ribaldone D Romano F Aimetti M Romandini M. The gum–gut Axis: periodontitis and the risk of gastrointestinal cancers. Cancer. (2023) 15:4594. doi: 10.3390/cancers 15184594 PMC 1052674637760563 · doi ↗ · pubmed ↗
- 6Nova E Gómez-Martinez S González-Soltero R. The influence of dietary factors on the gut microbiota. Microorganisms. (2022) 10:1368. doi: 10.3390/microorganisms 1007136835889087 PMC 9318379 · doi ↗ · pubmed ↗
- 7Li Y. The roles and applications of short-chain fatty acids derived from microbial fermentation of dietary fibers in human cancer. Front Nutr. (2023) 10:1243390. doi: 10.3389/fnut.2023.124339037614742 PMC 10442828 · doi ↗ · pubmed ↗
- 8Munteanu C Schwartz B. Interactions between dietary antioxidants, dietary Fiber and the gut microbiome: their putative role in inflammation and Cancer. Int J Mol Sci. (2024) 25:8250. doi: 10.3390/ijms 2515825039125822 PMC 11311432 · doi ↗ · pubmed ↗