Analysis of the clinical characteristics of direct oral anticoagulants-associated atraumatic splenic rupture
Can Shi, Xia Wang, Siyi Zhang, Ren Guo, Tian Wu

TL;DR
This study examines a rare but serious complication of direct oral anticoagulants (DOACs) called atraumatic splenic rupture, highlighting the importance of early diagnosis and treatment.
Contribution
The study provides a detailed clinical analysis of DOAC-associated atraumatic splenic rupture cases, emphasizing risk factors and management strategies.
Findings
Atraumatic splenic rupture occurred in 27 patients, most commonly associated with apixaban.
Elderly patients with comorbidities and polypharmacy were at higher risk.
Most patients survived with interventions like transfusion, embolization, and splenectomy.
Abstract
Atraumatic splenic rupture (ASR), though rare, is an adverse event linked to direct oral anticoagulants (DOACs). Given their widespread use and potentially fatal consequences if undiagnosed, heightened clinical awareness of DOAC-associated ASR is crucial. Our aim was to analyze the occurrence and clinical characteristics of ASR induced by DOACs. We conducted a retrospective analysis of all reported DOAC-associated ASR cases through 15 April 2025, without language restrictions. A total of 27 patients (11 males and 16 females) were included with a median age of 64 years. Among them, apixaban (n = 17) was the most common DOAC, followed by rivaroxaban (n = 8) and dabigatran (n = 2), with atrial fibrillation (81.5%, n = 22) being the primary indication. The comorbidities observed among patients with DOAC-associated ASR risk included hypertension (25.9%), coronary heart disease (18.5%),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
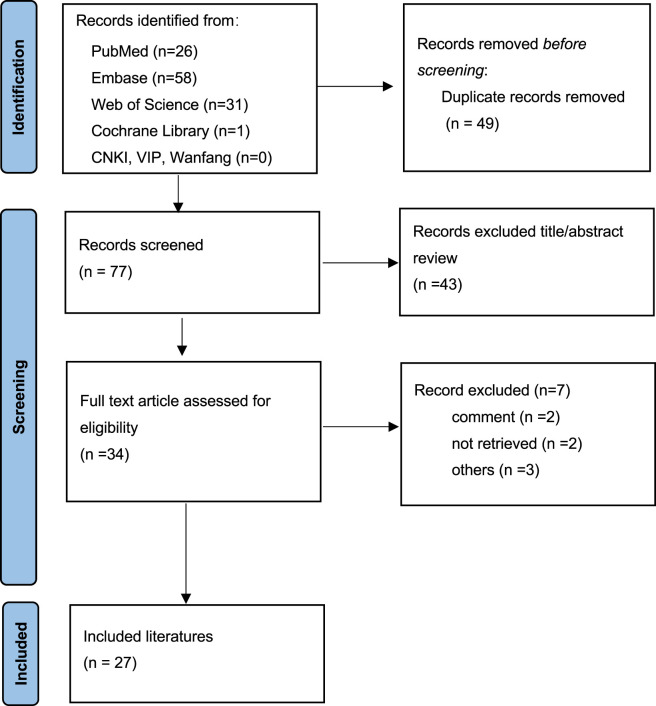 FIGURE 1
FIGURE 1| References | Age/sex | Region | Drug | Indication | Dose | Duration | Symptoms | Risk factor | Concomitant medication | Treatment | Hospitalization day |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| 62/f | Ireland | Apixaban | AF | — | 6d | AP, Hypo | 6d s/p PCI | Clopidogrel | Splenectomy and partial gastrectomy | 18 |
|
| 76/f | United States | Apixaban | AF | — | LT | AP, CP, nausea | Colonoscopy 16d prior | — | PRBCs, splenectomy | 6 |
|
| 77/f | — | Apixaban | AF | — | LT | AP, nausea, hypo | cancer | — | PRBCs,PCC, splenectomy | 10 |
|
| 57/f | United States | Apixaban | PE | — | Recent | AP, hypo | Healthy | — | PRBCs, FFP, PCC, SAE, splenectomy | 12 |
|
| 68/f | United States | Rivaroxaban | DVT | — | — | AP, Hypo | Pancreatitis | — | PRBCs, SAE, splenectomy | 21 |
|
| 88/m | Spain | Apixaban | AF | — | LT | AP | HF, s/p GU surgery | Omeprazole, furosemide | PRBCs, splenectomy | 11 |
|
| 58/f | United States | Apixaban | DVT | — |
| AP, syncope, nausea, hypo | Cancer | — | PRBCs, PCC, SAE | — |
|
| 56/f | United States | Apixaban | AF | — | — | AP | RHD, IE | — | PRBCs, SAE | 8 |
|
| 66/m | AUS | Apixaban | AF | 5 mg bid | LT | Syncope, AP, hypo | s/p Noro, EMCR | Amlodipine, telmisartan, aspirin, atorvastatin, metoprolol, citalopram | PRBCs, Cryo, FFP, platelets, PCC, SAE, splenectomy | 6 |
|
| 78/m | Portugal | Apixaban | AF | — | — | Syncope, nausea, AP, CP, dyspnea, hypo | CLL, DM, HTN | — | PRBCs, FFP, PPC, Fbg, platelets, TXA, splenectomy | — |
|
| 67/m | France | Rivaroxaban | AF | 15 mg qd | 2 m | AP, hypo | Healthy | Betaxolol, rosuvastatin, flecainide, amlodipine | PCC, PRBCs, FFP, splenectomy | — |
|
| 83/m | United States | Apixaban | AF | 2.5 mg bid | LT | Dyspnea, hypo | CKD, COPD, HF,PH | Probenecid, finasteride, omeprazole | PRBCs, FFP, SAE, splenectomy | — |
|
| 63/m | CHE | Apixaban | AF | — | LT | AP, syncope, hypo | CMML | Prednisone | SAE, splenectomy | 13 |
|
| 64/m | Belgium | Rivaroxaban | AF | — | LT | Syncope, AP | HTN, Constip., AFL ablation | Amiodarone, bisoprolol, atorvastatin | PRBCs, FFP, platelets, splenectomy | — |
|
| 65/m | United States | Apixaban | AF | — | LT | Syncope, AP dyspnea, hypo | AEP, ECV | Metoprolol, amiodarone | Splenectomy | — |
|
| 73/f | United States | Rivaroxaban | AF | 15 mg qd | LT | AP, | HTN,HF | — | PRBCs, SAE | — |
|
| 73/f | — | Rivaroxaban | AF | 20 mg qd | LT | AP, CP | COPD | — | PRBCs, PCC, splenectomy | 12 |
|
| 82/f | United States | Apixaban | AF | 2.5 mg bid | LT | AP | ESRD | Clopidogrel | Splenectomy | — |
|
| 81/m | United States | Apixaban | AF | — | LT | AP, hypo | HTN,DM, MG, PCI | Clopidogrel, aspirin | Conservative treatment | — |
|
| 77/f | United Kingdom | Dabigatran | Takotsubo CM | — | 1 day | AP | APE | — | Idarucizumab, PRBCs | — |
|
| 86/m | United States | Apixaban | AF | 5 mg bid | LT | AP, hypo | HTN,DM, CAD | Aspirin, atorvastatin, carvedilol, metformin | PRBCs, PCC, FFP, SAE, splenectomy | 5 |
|
| 75/f | Japan | Apixaban | AF | — | LT | AP | — | — | SAE | — |
|
| 77/f | AUS | Rivaroxaban | AF | 20 mg qd | 1 day | AP, hypo | Depression, ECV, HTN | Metoprolol, atorvastatin esomeprazole, quetiapine, amiodarone | PRBCs, Cryo, FFP, platelets, PCC,SAE | 14 |
|
| 66/f | United States | Apixaban | AF | — | 3 d | AP, hypo | 3d s/p appendectomy, GCCA | — | PRBCs, FFP, splenectomy | 30 |
|
| 78/f | United States | Dabigatran | AF | 100 mg bid | 7d | AP, nausea | CAD, DM, PAD | — | PRBCs, FFP, SAE | — |
|
| 66/m | Australia | Rivaroxaban | AF | 20 mg qd |
| AP, CP, dyspnea | CAD, pneumonia | Aspirin, atorvastatin, metoprolol, ramipril, digoxin | PRBCs, FFP, PCC, splenectomy | 10 |
|
| 76/f | Germany | Rivaroxaban | AF | 20 mg qd | LT | AP | HTN | Verapamil | Splenectomy | — |
| Parameter | Clinical features | Value |
|---|---|---|
| Sex | Male | 11 (40.7) |
| Female | 16 (59.3) | |
| Age | Years | 73 (65–78) |
| Region | United States | 13 (48.1) |
| Australia | 3 (11.1) | |
| Switzerland | 1 (3.7) | |
| France | 1 (3.7) | |
| Belgium | 1 (3.7) | |
| United Kingdom | 1 (3.7) | |
| Japan | 1 (3.7) | |
| Portugal | 1 (3.7) | |
| Spain | 1 (3.7) | |
| Ireland | 1 (3.7) | |
| Germany | 1 (3.7) | |
| Unknown | 2 (7.4) | |
| DOACs | Apixaban | 17 (63.0) |
| Rivaroxaban | 8 (29.6) | |
| Dabigatran | 2 (7.4) | |
| Indications | AF | 22 (81.5) |
| VTE | 3 (11.1) | |
| Other | 2 (7.4) | |
| Accompanying diseases | Hypertension | 7 (25.9) |
| Coronary heart disease | 5 (18.5) | |
| Malignant diseases | 5 (18.5) | |
| Infections | 5 (18.5) | |
| Diabetes | 4 (14.8) | |
| Heart failure | 3 (11.1) | |
| ESRD | 1 (3.7) | |
| Concomitant medications | Statins | 6 (22.2) |
| Aspirin/clopidogrel | 6 (22.2) | |
| β-blockers | 5 (18.5) | |
| Amiodarone | 3 (11.1) | |
| Verapamil | 1 (3.7) | |
| Number of concomitant medications | 1 | 3 (11.1) |
| 2 | 1 (3.7) | |
| 3 | 2 (7.4) | |
| 4 | 5 (18.5) |
| Parameter | Clinical features | Value |
|---|---|---|
| Time to ASR from taking DOACs | 1∼7 days | 6 (22.2) |
| 2 months | 1 (3.7) | |
| Long term | 17 (63.0) | |
| Unknown | 3 (11.1) | |
| Presenting symptoms | Abdominal pain | 27 (100.0) |
| Hypotension | 18 (66.7) | |
| Syncope | 6 (22.2) | |
| Nausea | 5 (18.5) | |
| Dyspnea | 5 (18.5) | |
| Chest pain | 4 (14.8) | |
| Examination | Abdominal CT | 25 (92.6) |
| Ultrasound | 3 (11.1) | |
| Unknown | 1 (3.7) | |
| Risk factors for ASR | Malignant diseases | 5 (18.5) |
| Infections | 5 (18.5) | |
| Electrical cardioversion/AFL ablation | 3 (11.1) | |
| Colonoscopy | 1 (3.7) | |
| Pre/postoperative diagnosis | Preoperative | 9 (33.3) |
| Postoperative | 12 (44.4) | |
| Unknown or not applicable | 6 (22.2) | |
| Laboratory indicators | Hemoglobin | |
| >10 g/dL | 4 (14.8) | |
| 7∼10 g/dL | 7 (25.9) | |
| <7 g/dL | 7 (25.9) | |
| Unknown | 9 (33.3) | |
| INR | | |
| <1.5 | 4 (14.8) | |
| 1.5∼2.0 | 7 (25.9) | |
| Unknown | 16 (59.3) | |
| APTT | | |
| >35 s | 2 (11.1) | |
| Normal | 5 (18.5) | |
| Unknown | 20 (74.1) |
| Parameter | Subgroup/Variable | Value |
|---|---|---|
| Treatments | Stop DOAC | 27 (100.0) |
| Transfusion therapy | 21 (77.8) | |
| PRBCs | 21 (77.8) | |
| FFP | 11 (40.7) | |
| PCC | 9 (33.3) | |
| Platelets | 4 (14.8) | |
| Cryoprecipitate | 2 (7.4) | |
| Splenic artery embolization | 12 (44.4) | |
| Splenectomy | 19 (70.4) | |
| Embolization of the splenic artery + splenectomy | 6 (22.2) | |
| Prognosis | Recovered and discharged | 25 (92.6) |
| Unknown | 2 (7.4) | |
| Resumption of anticoagulation | Yes | 3 (11.1) |
| No or unknown | 24 (88.8) | |
| Hospitalization day | 1∼7 day | 3 (11.1) |
| 8∼14 day | 8 (29.6) | |
| >14 day | 3 (11.1) | |
| Unknown | 13 (48.1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Case Reports on Hematomas · Trauma, Hemostasis, Coagulopathy, Resuscitation
Introduction
Direct oral anticoagulants (DOACs), which act by specifically inhibiting thrombin or activated factor X (factor Xa) in the coagulation cascade, have become increasingly prescribed for thromboembolic prophylaxis and treatment due to their favorable pharmacokinetic profile and convenience (Long and Gottlieb, 2023; Hindley et al., 2023). Multiple large-scale randomized controlled trials (RCTs) have confirmed the satisfactory efficacy of DOACs along with their significant reduction in major bleeding risk (Patel et al., 2011; Agnelli et al., 2013; Granger et al., 2011; Connolly et al., 2009; Giugliano et al., 2013). However, it is noteworthy that despite an overall reduction in bleeding complications, atraumatic splenic rupture (ASR) is increasingly being recognized as a potential adverse effect associated with DOAC therapy (Ostos Perez et al., 2023).
ASR, which is defined as spontaneous capsular disruption of the spleen without significant trauma, is rare and life-threatening, especially if it is not immediately recognized (Renzulli et al., 2009). The mortality rate of ASR is approximately 12.2% (Renzulli et al., 2009). Recently, case reports have identified an association between DOAC use and ASR, a potentially catastrophic complication that remains poorly characterized in the literature.
Despite its rarity, DOAC-associated ASR warrants clinical vigilance due to widespread DOAC use and potentially fatal outcomes if undiagnosed (Writing Committee et al., 2024). In our study, we collected patients with ASR after treatments with DOACs and characterize the clinical features, risk factors, treatments, and outcomes, which will guide clinicians in early detection and appropriate management, ultimately reducing morbidity and mortality.
Methods
Search strategy
A comprehensive literature search was conducted in PubMed, Embase, Web of Science, the Cochrane Library, China National Knowledge Infrastructure (CNKI), VIP Database, and Wanfang Data from their inception through 15 April 2025, to identify studies on DOAC-associated ASR. The search strategy combined Medical Subject Headings (MeSH) terms and free-text words, including (“Apixaban” [MeSH] OR “Dabigatran” [MeSH] OR “Rivaroxaban” [MeSH] OR “Edoxaban” [MeSH] OR “Betrixaban” [MeSH] OR “DOACs” [All Fields] OR “NOACs” [All Fields] OR “Direct Oral Anticoagulants” [All Fields] OR “Novel Oral Anticoagulants” [All Fields]) AND (“Splenic rupture” [MeSH] OR “Spleen rupture” [All Fields]). There was no language restriction. Review articles, commentaries, animal studies, and duplicate reports were excluded.
Data extraction
We used a self-designed table to extract the following patient characteristics: sex, age, nationality, anticoagulant regimen (including specific agent, dosage, and duration), indications for anticoagulation, underlying comorbidities, concomitant medications, risk factors for splenic rupture, clinical presentation, laboratory parameters (hemoglobin level, platelet counts, coagulation profile, and renal function), imaging findings, histopathological results (when available), treatments, and clinical outcomes.
Diagnostic criteria for atraumatic splenic rupture
The diagnosis of ASR was confirmed through comprehensive evaluation incorporating clinical manifestations, imaging findings, and histopathological evidence when available. Key diagnostic components included: (1) acute onset of abdominal pain (typically left upper quadrant or diffuse) accompanied by signs of hemodynamic instability (systolic blood pressure <90 mmHg or a heart rate >100 bpm) and/or laboratory evidence of acute blood loss (hemoglobin decline ≥2 g/dL from baseline); (2) radiographic confirmation via contrast-enhanced abdominal CT demonstrating characteristic findings including splenic parenchymal disruption, subcapsular hematoma, or hemoperitoneum; (3) definitive exclusion of traumatic etiology through detailed history review and physical examination (Liu et al., 2019; Soeborg et al., 2024).
Statistical analysis
Statistical analyses were performed with Statistical Package for Social Science (SPSS) version 27.0 (IBM Corp., Armonk, NY, United States). Categorical variables were expressed as percentages (%), while continuous variables were presented as medians with ranges. The causality of DOAC-associated ASR was assessed using the Naranjo Adverse Drug Reaction (ADR) Probability Scale.
Results
Patients’ information
A flow diagram for the study is provided in Figure 1. According to the inclusion and exclusion criteria, a total of 27 articles (Ostos Perez et al., 2023; Ahmed et al., 2020; Naseem et al., 2015; Bowers et al., 2024; Gonzva et al., 2014; High et al., 2024; Janke et al., 2020; Barnes et al., 2022; Kaufman and Ferraro, 2017; Kawazoe et al., 2022; Nagaraja et al., 2018; Widmer et al., 2021; Labaki and De Kock, 2022; Lopez Marcano et al., 2020; Lowry and Goldner, 2016; Moore et al., 2012; Mourato Nunes et al., 2018; Yau et al., 2020; Natarajan et al., 2021; Patnaik et al., 2021; Pietsch et al., 2021; Abdulrahman et al., 2021; Hetzler and Owens, 2021; Basnet et al., 2019; Carey and Nelatur, 2018; Amin et al., 2016; Abdelhady et al., 2018) involving 27 patients were included after full-text screening (Table 1). The basic information about these patients is summarized in Table 2. These patients (11 males and 16 females) with DOAC-associated ASR in our study were mainly from United States (48.1%) and Europe (37.0%), with a median age of 73 years (65–78 years). The DOACs were apixaban in 17 cases, rivaroxaban in 8 cases and dabigatran in 2 cases, 81.5% of which were prescribed for atrial fibrillation (AF) (22 patients). The most common comorbidity in the patients with DOAC-associated ASR was hypertension (25.9%), coronary heart disease (18.5%), malignant diseases (18.5%), and infectious diseases (18.5%). Among the 27 patients, 11 (40.7%) were prescribed concomitant medications that may potentiate the anticoagulant effect of DOACs. Specifically, 6 patients (22.2%) were on statins, 6 (22.2%) on aspirin and/or clopidogrel, 3 (11.1%) on amiodarone, and 1 (3.7%) on verapamil. Of the 11 patients receiving interacting medications, 3 used one such drug, 1 used two, 2 used three, and 5 used four concurrently. Among the 11 patients taking concomitant medications, only 4 had documented dosages of their anticoagulants. All 4 were on anticoagulation therapy for atrial fibrillation, with 2 of them (Naseem et al., 2015; Pietsch et al., 2021) receiving full-dose regimens.
Flow chart of study selection process for reported cases of direct oral anticoagulants associated atraumatic splenic rupture.
Clinical features
The clinical characteristics of the 27 patients with DOAC-associated ASR were summarized in Table 3. The time from anticoagulant initiation to symptom onset varied from 1 day to several years. Among these patients, 63% were on long-term anticoagulation (defined as ≥12 months of continuous use). All patients presented with abdominal pain, with some cases also exhibiting concurrent chest pain. Among the 27 patients, 18 developed hypotension, 6 experienced syncope, 5 reported nausea, and 5 manifested dyspnea. Identified risk factors for ASR were documented in 14 patients, including 5 with malignancies, 5 with infections, 3 following electrical cardioversion, and 1 after colonoscopy. ASR was preoperatively diagnosed in 9 patients, while 12 patients were diagnosed with ASR only during exploratory laparotomy. Additionally, 6 patients did not undergo surgery, or their surgical status was not described in the article. Based on the Naranjo ADR Probability Scale, the scores were distributed as follows: 13 patients (48.1%) scored 8 points (indicating a probable ADR), while 14 patients (51.9%) scored 5 points (suggesting a possible ADR).
Laboratory tests
Of the 18 patients measured, 14 (51.8%) had hemoglobin levels below 10 g/dL, including 7 cases (38.9%) with severe anemia (<7 g/dL). Coagulation parameters revealed that International Normalized Ratio (INR) values between 1.5 and 2.0 in 7 patients (38.9%) – none exceeding the therapeutic threshold of 2.0 – while only 2 patients (11.1%) showed prolonged activated partial thromboplastin time (APTT >35 s). Details are shown in Table 3.
Treatments and outcomes
The treatment and prognosis of the 27 included patients are summarized in Table 4. All patients immediately stopped DOACs. Among them, 12 patients (44.4%) underwent splenic artery embolization, and 19 patients (70.4%) required splenectomy, including 6 cases (31.6% of splenectomies) where splenic artery embolization failed, necessitating subsequent splenectomy. Transfusion support was provided to 21 patients (77.8%), consisting of packed red blood cells (n = 21), fresh frozen plasma (n = 11), prothrombin complex concentrate (n = 9), platelets (n = 4), and cryoprecipitate (n = 2). Three patients resumed anticoagulation without experiencing recurrent bleeding. All patients had favorable outcomes with no reported mortality cases.
Discussion
ASR has recently been recognized as a bleeding complication of DOACs that is frequently overlooked yet potentially fatal in clinical practice. Our study identified Factor Xa inhibitors as the primary trigger of DOAC-associated ASR, with apixaban being the most frequently implicated. The latency period from anticoagulant initiation to ASR symptom onset varied widely, ranging from 1 day to several years, though most cases occurred during long-term anticoagulation therapy for AF. Notably, DOAC-associated ASR was more commonly reported in elderly patients (>73 years) and those of European/North American descent. The most prevalent comorbidities among DOAC-associated ASR patients included hypertension, coronary heart disease, malignancies, and infectious diseases. Of the 27 patients analyzed, 11 (40.7%) were taking concomitant medications that may potentiate DOAC effects. All patients presented with abdominal pain, and 92.8% required embolization or splenectomy; all patients achieved favorable outcomes following intervention.
The reported incidence of ASR is approximately 3.2% (Liu et al., 2019), with a concerning mortality rate reaching 12.2% (Renzulli et al., 2009). The clinical significance of ASR lies in the potential for delayed diagnosis to lead to persistent internal hemorrhage, hemodynamic instability, and ultimately fatal outcomes. Current research suggests that anticoagulants may increase splenic rupture risk by interfering with the spleen’s hemostatic mechanisms, inducing microtrauma and reactive macrophage infiltration within splenic tissue. This association is supported by systematic reviews, including Aubrey-Bassler and Sowers’ analysis of 613 cases identifying 47 drug-related ASR episodes (7.6%), including 21 anticoagulant-associated cases (Aubrey-Bassler and Sowers, 2012), and Renzulli et al.'s larger series of 845 ASR patients documenting 67 drug-induced instances, 22 of which involved anticoagulants (Renzulli et al., 2009). Apixaban, a direct factor Xa inhibitor, was demonstrated non-inferior to warfarin for stroke prevention in patients with atrial fibrillation as well as for management of venous thromboembolism, with a decreased risk of major bleeding, in the ARISTOTLE (Granger et al., 2011) and AMPLIFY (Agnelli et al., 2013) trials, respectively. Despite the reduced bleeding risk, our study suggested that Factor Xa inhibitors may be a primary trigger of ASR-related cases, with apixaban being the most frequently implicated. This may be related to apixaban having the highest hepatic metabolism proportion (75%) among DOACs (Chan et al., 2020), and the precise mechanisms require further investigation.
The spleen, as the body’s most vascularized lymphoid organ, becomes particularly vulnerable when pre-existing pathological conditions—such as infectious splenomegaly, vascular malformations, or infiltrative disorders—compromise its structural integrity (Akoury and Whetstone, 2025). This vulnerability is exacerbated by anticoagulation therapy through directly impairing hemostasis while (2) potentially accelerating subcapsular hematoma progression to frank rupture. In our study, 14 out of 27 patients (51.9%) had comorbid conditions that could lead to pathological splenic changes, such as malignancies or infections, while 11 patients (40.7%) were taking concomitant medications that may potentiate anticoagulant effects.
Until now, no guidelines for ASR treatment are available, and suggestions are derived from case reports. Splenectomy, splenic artery embolization, and transfusion therapy are the mainstays, which could be inferred from the above-mentioned cases. In our study, among the 12 patients who attempted embolization, 6 ultimately required splenectomy due to embolization failure, representing a 50% failure rate. The underlying mechanisms may involve two key factors: ① impaired tissue repair capacity in pathologically altered spleens, and ② the advanced age of the patient population (mean age 73 years). These findings imply that open splenectomy remains the definitive therapeutic option for anticoagulant-associated ASR, particularly in hemodynamically unstable patients.
This study has several important limitations. First, the case series component included only 27 patients, allowing only descriptive summaries without hypothesis testing, risk estimation, or adjustment for confounders. Second, the absence of a control group precludes distinguishing drug-related risks from those attributable to underlying conditions, concurrent illnesses, recent procedures, or coincidental associations—even in instances where Naranjo scores indicate a possible or probable relationship. Third, heterogeneity in case definitions, reporting completeness, and management strategies limits meaningful subgroup comparisons. Consequently, these findings should be interpreted as exploratory and serve primarily to inform the design of future large-scale, prospective studies.
Conclusion
ASR may represent a critical yet potentially preventable complication of DOAC therapy. Enhancing clinical vigilance, especially in elderly patients with comorbidities and polypharmacy, coupled with prompt imaging for abdominal pain, could help mitigate adverse outcomes. Future research should focus on identifying biomarkers for early detection and exploring spleen-sparing management strategies through prospective studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdelhady A. Ahmed A. Mohamed Y. Binchy J. (2018). Apixaban-associated spontaneous splenic rupture-a case report. Ir. Med. J. 111, 792. 30520619 · pubmed ↗
- 2Abdulrahman Z. Turki M. h. Azeez H. Ben Selma A. (2021). Spontaneous ruptured splenic artery aneurysm presenting as an acute abdominal mass. Am. J. Gastroenterol. 116, S 998–S 999. 10.14309/01.ajg.0000782920.27020.88 · doi ↗
- 3Agnelli G. Buller H. R. Cohen A. Curto M. Gallus A. S. Johnson M. (2013). Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 369, 799–808. 10.1056/NEJ Moa 1302507 23808982 · doi ↗ · pubmed ↗
- 4Ahmed M. M. Khan Z. H. Zaidi S. R. Mukhtar K. (2020). A delayed splenic tragedy beyond the scope of a colonoscope: a rare find. Cureus 12, e 7805. 10.7759/cureus.7805 32467782 PMC 7249756 · doi ↗ · pubmed ↗
- 5Akoury T. Whetstone D. R. (2025). “Splenic rupture,” in Stat Pearls (Teature Island, FL: Stat Pearls Publishing).
- 6Amin A. Safaya A. Ronny F. Islam H. Bhuta K. Rajdeo H. (2016). Hemorrhagic shock from spontaneous splenic rupture requiring open splenectomy in a patient taking rivaroxaban. Am. Surg. 82, E 54–E 55. 26874127 · pubmed ↗
- 7Aubrey-Bassler F. K. Sowers N. (2012). 613 cases of splenic rupture without risk factors or previously diagnosed disease: a systematic review. BMC Emerg. Med. 12, 11. 10.1186/1471-227X-12-11 22889306 PMC 3532171 · doi ↗ · pubmed ↗
- 8Barnes J. Alhaddad Z. Paz R. Haas C. (2022). Atraumatic splenic rupture on direct oral anticoagulation. J. Community Hosp. Intern Med. Perspect. 12, 84–87. 10.55729/2000-9666.1098 36262482 PMC 9529660 · doi ↗ · pubmed ↗