Case Report: Pleomorphic adenoma of the breast: diagnostic pitfalls and a novel PLAG1::FTO fusion
Jing Lian, Mengqin Yang, Peng Bu, Junfeng Jiang, Chun Wu, Yanfeng Xi

TL;DR
This case report describes a rare breast tumor misdiagnosed as cancer and identifies a new gene fusion that could help in understanding and diagnosing similar cases.
Contribution
The study reports a novel PLAG1::FTO gene fusion in a rare breast tumor, expanding its genetic understanding.
Findings
A breast tumor was initially misdiagnosed as mucinous carcinoma but later confirmed as pleomorphic adenoma.
Hi-C and RNA-Seq revealed a novel PLAG1::FTO gene fusion in the tumor.
The case highlights the diagnostic challenges and genetic complexity of pleomorphic adenoma of the breast.
Abstract
Pleomorphic adenoma (PA) of the breast and its malignant transformation represent extremely rare clinical entities, and the molecular alterations underlying this tumor type remain largely uninvestigated to date. Herein, we report a diagnostic challenge posed by a case of mammary pleomorphic adenoma, which was initially misdiagnosed as mucinous carcinoma during frozen section examination; the definitive diagnosis was ultimately confirmed based on a comprehensive analysis of the surgical resection specimen. As implied by the term “pleomorphic,” this tumor exhibits remarkable phenotypic heterogeneity. Therefore, a thorough understanding of the morphological features of rare breast PA is crucial for mitigating the risk of misdiagnosis in clinical practice. To explore the genetic characteristics of this tumor, we employed High-throughput Chromosome Conformation Capture (Hi-C) and RNA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
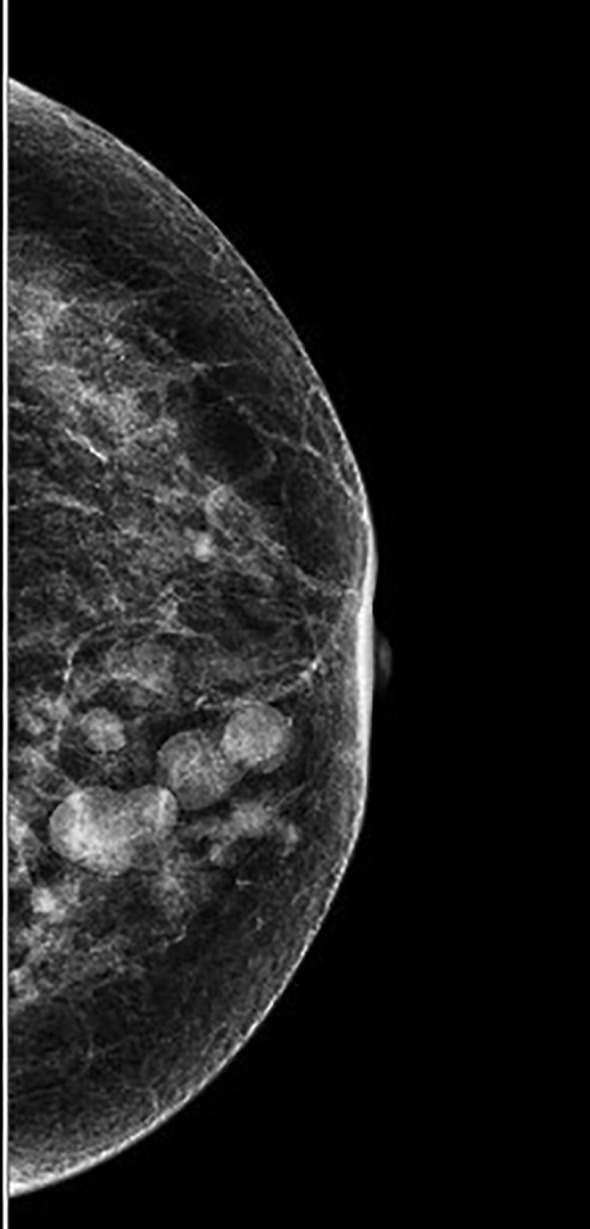 Figure 1
Figure 1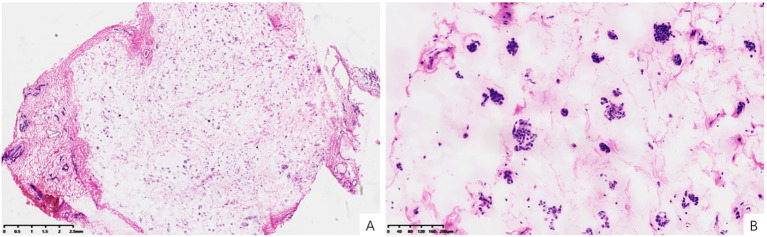 Figure 2
Figure 2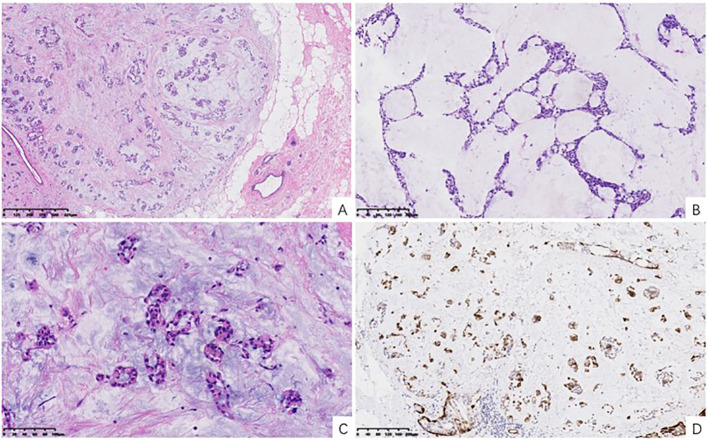 Figure 3
Figure 3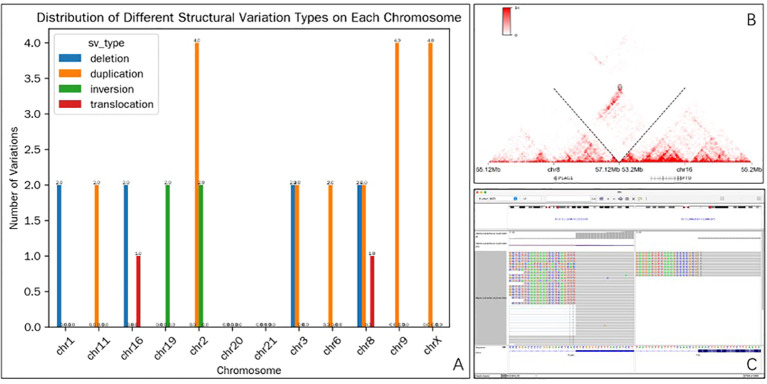 Figure 4
Figure 4| Tumor type | Recurrent molecular alterations | Key features |
|---|---|---|
| Pleomorphic adenoma | PLAG1 rearrangements (PLAG1::FTO, PLAG1::CTNNB1, PLAG1::TRPS1, etc.), HMGA2 rearrangements (HMGA2::WIF1) | Benign; biphasic differentiation; chondromyxoid stroma |
| Mucoepidermoid carcinoma | CRTC1::MAML2, CRTC3::MAML2 fusions | Malignant; epidermoid/intermediate cells; mucous cells |
| Adenoid cystic carcinoma | MYB::NFIB, MYBL1 rearrangements | Malignant; cribriform/tubular pattern; basaloid cells |
| Adenomyoepithelioma | HMGA2::WIF1 (subset), PLAG1 rearrangements (subset) | Dual differentiation; prominent myoepithelial layer |
| Secretory carcinoma | ETV6::NTRK3 fusion | Malignant; S100+, mammary-type secretion |
| Carcinosarcoma/Metaplastic carcinoma | TP53 mutations, PIK3CA mutations, PTEN loss, complex karyotypes | Malignant; heterologous elements; high-grade atypia |
| Benign phyllodes tumor | MED12 mutations, TERT promoter mutations, RARA rearrangements | Leaf-like architecture; stromal overgrowth; no PLAG1/HMGA2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Breast Cancer Treatment Studies · Salivary Gland Tumors Diagnosis and Treatment
Introduction
Pleomorphic adenoma (PA), is the most commonly encountered benign neoplasm observed in the salivary glands. In contrast, Its manifestation in the breast is extremely rare, with only isolated case reports and small series having been documented (1–8). It may easily be overlooked in breast pathology, resulting in missed diagnosis, particularly when evaluating frozen sections or needle biopsy samples. The abundant myxoid stroma can mimic mucinous carcinoma or matrix-producing variants of metaplastic carcinoma, particularly on limited sampling (5, 9). As a result, there is a risk of misdiagnosis and potential overtreatment. PLAG1 or HMGA2 fusion is currently the most widely recognized genetic event in salivary gland PA, but molecular research on breast PA remains relatively rudimentary, with published studies having documented the same morphologic features as in corresponding salivary neoplasms. Here, we report for the first time a case of breast PA with PLAG1::FTO fusion and describe its clinical, pathological, and molecular features.
Materials and methods
Clinical presentation
A 59-year-old woman presented with palpated nodules in the left breast, which she had identified on self-examination. Physical examination revealed several non-tender nodules in the lower inner quadrant of the left breast without overlying skin changes, nipple discharge, or ulceration. Mammographic imaging revealed multiple rounded opacities with segmental distribution along the ductal system, the largest measuring 1.9 × 1.3 cm (Figure 1). Targeted breast ultrasound demonstrated multiple well-circumscribed, complex cystic-solid nodules with heterogeneous internal echotexture, localized to the 6–7 o’clock, 8–9 o’clock, and 9 o’clock periareolar regions. The largest measured 1.07 × 0.902 cm, with others ranging between 0.336 cm and 0.765 cm in maximal dimension.
Mammography: Multiple small and large round nodules of different sizes were found in the lower inner quadrant of the left breast, distributed in a segmental pattern along the ducts.
Immunohistochemistry
Representative formalin-fixed, paraffin-embedded tissue samples were selected, and 4 μm-thick sections were stained with antibodies specific for estrogen receptor (ER, clone: SP1, Abcam), progesterone receptor (PR, clone: SP2, Abcam), CK5/6 (clone: D5/16B4, DAKO), HER2 (clone: 4B5, Roche); p63 (clone: 4A4, Gene), S100 (clone: 4C4.9, Abcam), Calponin (clone: EP798Y, LBPMedicin), and Ki67 (clone: MIB-1, DAKO).
Hi-C library preparation
Hi-C sample preparation and library preparation were performed by Abcepta. Briefly, 3–5 FFPE tissue sections (10 μm thick) were deparaffinized and incubated in 0.3% SDS at 65 °C for 30 minutes, followed by quenching with 3% Triton X-100 at 37 °C for 15 minutes. The samples were then washed and resuspended in digestion buffer. Chromatin was digested with 200 U of DpnII restriction enzyme at 37 °C overnight with gentle rotation. Subsequently, dCTP, dGTP, dTTP, biotin-14-dATP, and Klenow DNA polymerase (5 U/μL) were added, followed by incubation at 23 °C for 4 h with rotation. The digested chromatin was ligated with 400 U T4 DNA ligase at 16 °C overnight. DNA was then isolated, and unligated ends were treated with T4 DNA polymerase to remove biotin labeling.
Up to 1 μg of DNA was fragmented, followed by end repair, A-tailing, and purification. The ligation products were enriched using 10 μl streptavidin beads and used as input for library preparation. Final libraries were quantified with a Qubit 4.0 Fluorometer (Thermo Fisher) and Qsep100 (BiOptic Inc.), followed by sequencing on an MGI DNBSEQ-T7 platform (30–50 million paired-end reads/sample).
RNA sequencing
Total RNA from each sample was extracted with an RNA extraction kit used as directed. RNA quality and concentration were evaluated with Qubit 4.0 Fluorometer and Nanodrop One (Thermo Fisher Scientific) instruments. Libraries were prepared following the standard protocol (catalog number, Vazyme), which included cDNA synthesis, A-tailing, adapter ligation, and PCR amplification. Probes were designed for a panel of 180 genes often fused in common solid tumors to capture the targeted regions of interest with the probeCap Hybridization and Wash Kit (catalog number, Homgen). Pair-end sequencing was performed using an MGI DNBSEQ-T7 platform, yielding 15–30 million reads.
Results
Frozen section
The patient underwent lumpectomy of the left breast. The gross specimen revealed multiple well-circumscribed nodules ranging from 0.3 cm to 1.9 cm in greatest dimension, with a firm, gray-white cut surface and glistening myxoid areas. Sections from representative nodules revealed a mucin-rich neoplasm composed of small nests and clusters of uniform epithelial cells suspended in a myxoid background (Figure 2A). No significant cytological atypia, mitotic figures, or necrosis were observed (Figure 2B). Nevertheless, due to the prominent mucin and architectural pattern, the preliminary diagnosis suggested a “mucin-producing tumor” favoring a mucinous carcinoma.
Frozen section. (A) Neoplasm with prominent mucin secretion (H&E, x10). (B) Small clustered or nest-like cells floating within the myxoid stroma (H&E, x100).
Paraffin section
Histologic evaluation of paraffin-embedded sections demonstrated a multinodular, well-demarcated lesion separated from adjacent breast tissue by variably thick fibrous pseudocapsules (Figure 3A). The neoplasm exhibited a range of architectural configurations, including tubules, cribriform islands, solid nests, and cords, intermixed within a strikingly myxoid to chondromyxoid stroma (Figures 3B, C). The epithelial component featured bland cuboidal cells with uniform nuclei, while the myoepithelial component appeared as spindled or stellate cells dispersed within the stroma or enveloping epithelial structures. There was no evidence of mitotic activity, necrosis, perineural invasion, or lymphovascular infiltration.
Histopathological features of mammary pleomorphic adenoma. (A) Low-power magnification showing a well-circumscribed, multinodular tumor with a fibrous pseudocapsule (H&E, x40). (B) Medium-power magnification demonstrating diverse architectural features, including tubular structures and solid nests within a myxoid background (H&E, x100). (C) High-power magnification highlighting the characteristic chondromyxoid stroma with chondrocyte-like cells (H&E, x200). (D) Immunohistochemistry staining for Calponin, highlighting the prominent myoepithelial cell component surrounding epithelial nests and dispersed within the stroma (Calponin IHC, x100).
Immunohistochemistry
Immunostaining confirmed the biphasic cellular nature of the tumor. Cytokeratin staining highlighted epithelial tubular and ductal structures. P63 and Calponin strongly labeled the myoepithelial cells both around glandular units and within the stroma (Figure 3D), with diffuse positivity. S100 protein staining revealed diffuse nuclear and cytoplasmic staining in stromal and chondroid areas. Estrogen receptor (ER), progesterone receptor (PR), and HER2 staining results were all negative. The Ki-67 proliferation index was approximately 5%.
Molecular analysis
Hi-C was employed to identify the distribution of different structural variation types on each chromosome (Figure 4A), revealing the presence of a novel PLAG1::FTO gene translocation variant on chromosomes 16 and 8 (Figure 4B). Cross-validation via RNA-seq confirmed the fusion event (Figure 4C).
Characterization of the PLAG1::FTO translocation. (A) Distribution of Different Structural variant types on each chromosome. (B) Hi-C analysis (10-kb resolution) identifying a robust balanced translocation event between the PLAG1 locus (chromosome 8) and the FTO locus (chromosome 16). (C) IGV visualization depicting the transcriptional read alignment patterns from RNA sequencing data, supporting the translocation event.
Treatment and outcome
Following lumpectomy, the case was successfully followed up for ten months, with no recurrence or metastasis.
Discussion
PA of the breast, initially described by Smith and Taylor in 1969 (1), is an exceedingly uncommon clinical entity. It predominantly affects postmenopausal women, with a reported female-to-male ratio of approximately 10:1, although isolated cases in males have been documented (3, 8). The pathogenesis of mammary PA is not fully elucidated, but some authors propose that it may arise from intraductal papillomas through exaggerated myoepithelial proliferation and stromal matrix production. Multifocal occurrences, as observed in this case, have also been linked to the presence of multiple underlying papillomatous foci (8, 10, 11).
Consistent with its “pleomorphic” designation, the histological heterogeneity of PA can present significant diagnostic challenges, particularly when working with frozen sections, fine needle aspirates, or core biopsy specimens (5, 9, 12). The present case illustrates the diagnostic complexities associated with mammary PA. Microscopically, the lesion consisted of well-formed glands and cords lined by an inner layer of epithelial cells and an outer layer of myoepithelial cells, set within an abundant myxoid matrix. Notably, the tumor lacked significant cytologic atypia, mitotic activity, or necrosis. While mucinous carcinoma typically exhibits cohesive clusters of bland epithelial cells floating in lakes of mucin with minimal stromal architecture. Immunohistochemistry played a vital role in diagnosing this case, highlighting myoepithelial elements with Calponin and P63, and confirming stromal myoepithelial presence via S100 positivity. The absence of ER, PR, and HER2 expression, along with a low Ki-67 proliferation index, further supported the benign nature of this neoplasm. A uniformly myxoid stroma may falsely suggest mucinous carcinoma, but the presence of stromal myoepithelial cells and biphasic architecture are not typical of mucinous carcinoma.
Other key entities to consider in the differential diagnosis include matrix-producing metaplastic carcinoma, adenomyoepithelioma, papilloma with cartilaginous metaplasia, and myxoid fibroadenoma. Importantly, breast carcinosarcoma or metaplastic carcinoma may mimic PA histologically due to the presence of heterologous elements and myxoid stroma; however, these lesions are malignant and typically demonstrate significant cytologic atypia, high mitotic activity, and different molecular profiles, such as TP53 mutations, PI3K pathway mutations (PIK3CA, PTEN loss), and complex karyotypes, rather than the specific PLAG1 or HMGA2 rearrangements characteristic of PA. Similarly, benign phyllodes tumor can show stromal overgrowth and heterologous cartilaginous or osseous elements, but it is genetically distinct, typically harboring MED12 mutations, TERT promoter mutations, or RARA rearrangements instead of PLAG1/HMGA2 fusions. In this case, the absence of nuclear atypia and low mitotic activity helped exclude matrix-producing metaplastic carcinoma. Although adenomyoepithelioma also exhibits dual epithelial-myoepithelial differentiation, it typically features a prominent and often stratified myoepithelial layer with less chondroid stroma. Salivary gland-type carcinomas such as adenoid cystic carcinoma (ACC) and mucoepidermoid carcinoma (MEC) may enter the differential. Neither exhibits the hallmark chondromyxoid stroma or PLAG1 gene rearrangement characteristic of PA. These molecular differences are summarized in Table 1, which highlights the distinct genetic landscapes of salivary gland-like tumors and their differential diagnoses.
Genetically, salivary gland PA frequently harbor chromosomal rearrangements involving PLAG1 or HMGA2. Recent studies have demonstrated that breast PAs share similar genetic alterations with their salivary gland counterparts, including fusions such as HMGA2::WIF1, CTNNB1::PLAG1, and TRPS1::PLAG1 in mammary PA (6, 7). However, the full spectrum of molecular alterations in breast PA remains to be fully characterized, and further studies are needed to determine whether all genetic changes defining salivary gland PA are also present in breast PA. Interestingly, HMGA2::WIF1 has also been detected in a subset of adenomyoepitheliomas, suggesting potential overlap in pathogenesis or derivation from a common progenitor lesion (13). In the present report, Hi-C was used to identify the distribution of different structural variants across chromosomes (including chromosomes 1, 11, 16, 19, 2, 3, 6, 7, 9, and X). Different chromosomes exhibited distinct frequencies of each structural variant type. For instance, chr2 presented with relatively high numbers of duplication (4 occurrences) and inversion (2 occurrences) events, while translocation was relatively rare and only appeared on chr16 and chr8. Cross-validation via RNA-seq confirmed the identified fusion event. PLAG1 encodes a zinc finger protein associated with cell cycle progression that can become activated as a result of promoter exchange with a variety of different partner fusion genes. When overexpressed, PLAG1 target genes tend to become dysregulated, most importantly IGF2, thereby driving tumorigenesis through transcriptional activation and altered MAPK pathway signaling. The novel PLAG1::FTO fusion gene is likely associated with the development of this breast PA lesion, further expanding the molecular spectrum associated with this rare breast tumor type. While the presence of this fusion was confirmed by both Hi-C and RNA-seq, the inability to perform PLAG1 immunohistochemistry limits our ability to demonstrate PLAG1 protein overexpression at the translational level. Therefore, the pathogenic significance of this specific fusion requires validation in additional cases and functional studies, which we acknowledge as a limitation of the current study.
Surgical excision with negative margins remains the standard treatment for breast PA (14–16). The prognosis is generally favorable, though incomplete excision may lead to local recurrence. Rare instances of malignant transformation have been reported, prompting some investigators to classify PA as a neoplasm of uncertain malignant potential (5). In light of this, we recommend long-term surveillance and consider molecular testing in diagnostically uncertain or recurrent cases. Further research is needed to define the clinical and prognostic significance of specific molecular alterations, such as the PLAG1::FTO fusion described here.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith BH Taylor HB . The occurrence of bone and cartilage in mammary tumors. Am J Clin Pathol. (1969) 51:610–8. doi: 10.1093/ajcp/51.5.610, PMID: 4305299 · doi ↗ · pubmed ↗
- 2Sato K Ueda Y Shimasaki M Ozaki M Nitta N Chada K . Pleomorphic adenoma (benign mixed tumor) of the breast: a case report and review of the literature. Pathol Res Pract. (2005) 201:333–9. doi: 10.1016/j.prp.2005.03.004, PMID: 15991841 · doi ↗ · pubmed ↗
- 3Molland JG Morgan GJ Walker DM Lin BP . Pleomorphic adenoma of the parotid and breast in a male patient. Pathology. (2005) 37:263–5. doi: 10.1080/00313020500099015, PMID: 16175906 · doi ↗ · pubmed ↗
- 4Leekha N Muralee M Mathews A Preethi TR Ahamed MI . Pleomorphic adenoma of breast-a case report and review of literature. Indian J Surg Oncol. (2014) 5:152–4. doi: 10.1007/s 13193-014-0310-y, PMID: 25114471 PMC 4116544 · doi ↗ · pubmed ↗
- 5Rakha EA Aleskandarany MA Samaka RM Hodi Z Lee AH Ellis IO . Pleomorphic adenoma-like tumour of the breast. Histopathology. (2016) 68:405–10. doi: 10.1111/his.12757, PMID: 26096183 · doi ↗ · pubmed ↗
- 6Pareja F Da Cruz Paula A Gularte-Mérida R Vahdatinia M Li A Geyer FC . Pleomorphic adenomas and mucoepidermoid carcinomas of the breast are underpinned by fusion genes. NPJ Breast Cancer. (2020) 6:20. doi: 10.1038/s 41523-020-0164-0, PMID: 32550265 PMC 7275089 · doi ↗ · pubmed ↗
- 7Ma S Zhao D Liu Y Rohr J Zhang F Ma Y . Some pleomorphic adenomas of the breast share PLAG 1 rearrangements with the analogous tumour of the salivary glands. Histopathology. (2021) 79:1030–9. doi: 10.1111/his.14461, PMID: 34292619 · doi ↗ · pubmed ↗
- 8Elaiwy O Al-Sawalmeh K Samra HA Haider A Akhtar M . Pleomorphic adenoma of breast: report of two cases, one in A male patient. Turk Patoloji Derg. (2022) 38:153–7. doi: 10.5146/tjpath.2021.01543, PMID: 34514577 PMC 9999686 · doi ↗ · pubmed ↗