Development of a clinical algorithm-based scoring system to diagnose smear-negative pulmonary tuberculosis in Sabah, Malaysia using the modified Delphi method
Chee Kuan Wong, Wai Khew Lee, Roddy Teo, Hema Y Ramamurthy, Jiloris Dony, Chin Hai Teo, Sarah Jane JC Chan, Suhashini Sivasegaran, Yao Long Lew, Ri Hui Lam, Karuthan Chinna, Giri S Rajahram, Timothy William, Yin Chin Chan, Jayakayatri J Nathan, Harish Nair, Harry Campbell

TL;DR
This study developed a clinical scoring system to help diagnose smear-negative pulmonary tuberculosis in Malaysia using expert input and statistical validation.
Contribution
A novel clinical algorithm-based scoring system for diagnosing smear-negative TB in resource-limited settings.
Findings
The algorithm achieved an area under the ROC curve of 0.88 with a cut-off score of 19.5.
It showed 86.2% sensitivity and 77.4% specificity in differentiating likely TB from unlikely TB cases.
Abstract
Tuberculosis (TB) remains a major global health threat, particularly in resource-constrained settings where delayed diagnosis of smear-negative pulmonary TB (SNPTB) is common due to limited access to rapid molecular diagnostics. We aimed to develop a clinical algorithm-based scoring system to aid the diagnosis of SNPTB among symptomatic patients in Sabah, Malaysia. We conducted a modified Delphi process between January and June 2024 involving three rounds of expert consultation via email to identify key clinical parameters for diagnosing SNPTB, followed by a consensus meeting to finalise the parameters and assign weightings. We then applied the algorithm to a data set of 60 symptomatic smear-negative individuals, of whom 29 were confirmed to be TB and 31 not TB based on culture. We calculated the sensitivity, specificity, positive predictive value (PPV), and negative predictive values…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
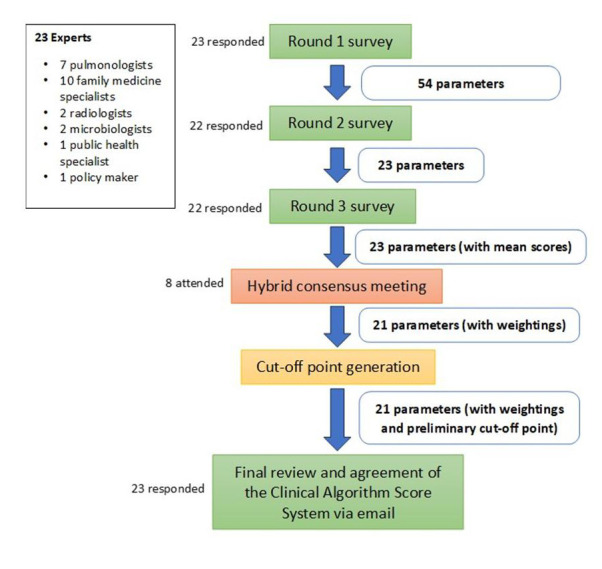 Figure 1
Figure 1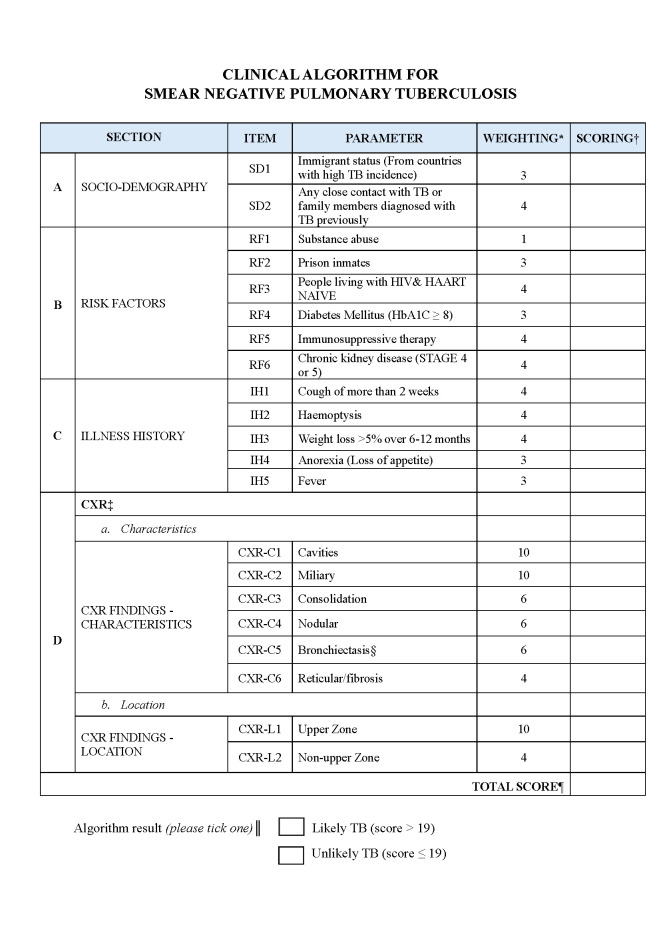 Figure 2
Figure 2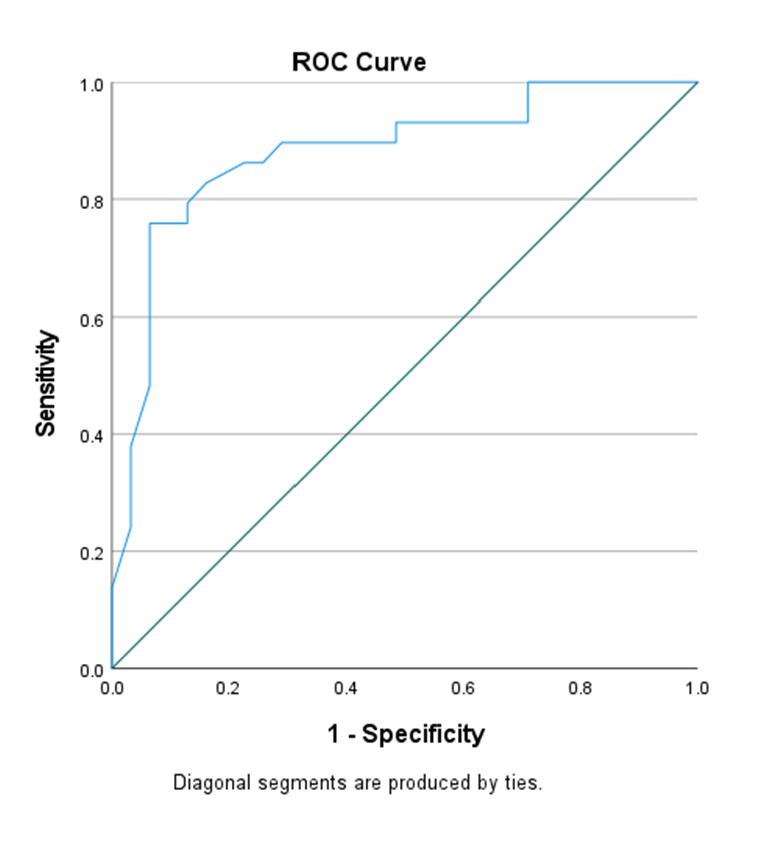 Figure 3
Figure 3| Actual diagnosis | ||||
|---|---|---|---|---|
|
|
|
|
|
|
|
|
| 25 (true positive) | 7 (false positive) | PPV = 25/32 (78.1%) |
|
|
| 4 (false negative) | 24 (true negative) | NPV = 24/28 (85.7%) |
| Sensitivity = 25/29 (86.2%) | Specificity = 24/31 (77.4%) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Delphi Technique in Research · Clinical Reasoning and Diagnostic Skills
Tuberculosis (TB) remains a major global public health problem, accounting for an estimated 10.8 million infections and 1.25 million people deaths worldwide in 2023, with over 80% occurring in low- and middle-income countries [1]. There was an upward trend in TB incidence globally following the COVID-19 pandemic, with most new cases occurring in the World Health Organization (WHO) regions of South-East Asia (45%), Africa (24%) and the Western Pacific (17%) [2]. In this context, timely and accurate diagnoses is critical to strengthening TB prevention and care [3].
While the national TB incidence in Malaysia was 78.3 per 100 000 population in 2023, Sabah, a state in the east of the country, saw a 2-fold rate at 160.3 per 100 000 population [4]. Smear-negative pulmonary TB (SNPTB) cases in Sabah constitute about 20% of all cases of pulmonary TB in the state [5]. Although the use of rapid molecular diagnostic tests has been incorporated into the latest Malaysian clinical practice guidelines for SNPTB since 2021, in line with WHO recommendations, their use remains limited in Sabah due to the high costs and limited availability outside tertiary hospitals [6]. Between 2012 and 2018, rapid molecular diagnostic test coverage was only 1.2% of notified TB cases in Sabah [5]; most SNPTB cases in Sabah are diagnosed clinically. A standardised diagnostic algorithm that can be used in the absence of rapid molecular diagnostic tests, benchmarked against GeneXpert and culture, would therefore be highly useful in this setting.
While algorithms for diagnosing SNPTB have already been developed in different contexts, many national programmes have adopted the WHO 2003 clinical algorithm [7], which has not been formally validated and lacks explicit clinical or radiological indicators, limiting its diagnostic accuracy. Indeed, a Cochrane review by Van’t Hoog et al. found that combining symptom-based and chest x-ray screening improves diagnostic yield, although sensitivity and specificity vary by region [8]. As a result, some countries have developed their own algorithms or adapted the WHO algorithm to include both clinical and radiographic criteria.
Existing diagnostic algorithms for SNPTB have shown variable performance across different settings, with many models demonstrating reduced accuracy compared with Mycobacterium tuberculosis culture and facing challenges in external validation (Table 1) [9–17]. Classical and artificial intelligence (AI)-enhanced diagnostic studies for SNPTB report a wide range of performance, from inconsistent sensitivity in symptom-and-CXR algorithms to moderate-high accuracy with neural networks and automated microscopy, and up to radiologist-level performance with deep-learning computer-aided detection and AI-enabled lung ultrasound (Table 2) [18–28]. This highlights the substantial advantages of data-driven and multimodal approaches over conventional rule-based methods.
However, these more advanced diagnostic tests are not widely accessible in Sabah. Given the limitations of existing algorithms and the unavailability of alternative, higher-cost diagnostic tools, there is a need for a practical clinical algorithm to support the diagnosis of SNPTB among symptomatic patients in settings without access to molecular testing or robust laboratory infrastructure. Therefore, we aimed to develop a locally relevant clinical algorithm scoring system by conducting a modified Delphi exercise to obtain consensus from a panel of experts.
METHODS
Study design: the modified Delphi method
The Delphi method and its modifications have been widely used in health sciences for obtaining a reliable consensus from a group of experts on a specified area [29]. It normally involves several rounds of surveys in which people vote until consensus is reached. The Delphi method can be modified, for example, by including focus group discussions, so long as it leads towards a group consensus.
For this study, we modified the Delphi method by using an online survey platform to enable as many experts as possible to participate. Care was taken to ensure the responses from the experts were collated and de-identified after each round to reduce the dominance of one expert as well as to avoid groupthink. We conducted three rounds of online surveys, after which we held a hybrid consensus meeting to further refine and apply weightings to the parameters in the algorithm.
Study participants
There is no established method to determine the sample size needed for a Delphi study, as it often depends on the topic area and convenience; while a sample of <10 participants is considered insufficient, a very high number would not necessarily improve the quality of the results. Akins et al. [30] recommended the use of at least 23 panellists to ensure reliability.
Here, we identified 27 experts from within Malaysia and internationally and invited them to participate. Individuals had to be TB experts with a minimum of five years’ experience in the management of TB and had to be representative in the management and diagnosis of SNPTB in Sabah. Experts were identified through consultation with local TB stakeholders and by reviewing the list of authors of the latest national clinical guidelines on TB management. Their contact details were obtained from their organisations’ webpages, and they were initially contacted via email or telephone. One international expert accepted the invitation, but subsequently did not respond-when the consent form was sent despite reminders.
Round 1, 2, and 3 survey: questionnaire and analysis
Round 1 of this Delphi survey, conducted in January 2024, aimed to generate a list of parameters for diagnosing TB among symptomatic SNPTB patients in Sabah. The experts were asked regarding their role and experience in managing patients with TB, followed by open-ended questions ‘Q1: what parameter(s) do you think should be included in an algorithm to diagnose smear-negative PTB?’ and ‘Q2: Can you suggest any recent studies or publications that may be relevant to this study? We analysed the answers to Q1 thematically, grouping the suggested parameters into themes and forming a preliminary framework. We also reviewed the publications suggested in Q2 and incorporated the identified parameters into the preliminary framework. After this round, we listed all identified parameters and removed duplicates.
The round 2 survey aimed to distil the proposed list of parameters to diagnose SNPTB. Specifically, we sent the preliminary framework back to the group of experts and asked them to rate the importance of each parameter identified in diagnosing SNPTB in primary care using a five-point Likert scale (1 = ‘not important at all’; 2 = ‘slightly important’; 3 = ‘moderately important’; 4 = ‘very important’; and 5 = ‘extremely important’. An a priori criteria for consensus required ≥70% of the respondents to rate of an item as ‘very important’ or ‘extremely important’ to be included in the refined framework.
The round 3 survey aimed to further refine the framework and attempted to assign a weight to each parameter. We sent this refined framework to the group of experts and asked them to score each item on its likelihood of being a marker for smear negative pulmonary TB using a scale from 0 (unlikely) to 100 (likely).
We collected data using the REDCap secure online platform for all the rounds. New questionnaires were formulated for the subsequent rounds based on the preceding round until a consensus was reached. Each round of questionnaires took approximately 30 minutes to complete, and the experts were given up to three weeks to respond, with reminders sent each week.
Hybrid expert consensus meeting
We initially intended to use the mean score for each parameter at round 3 as the weighting of the parameter. However, we found that the mean scores of the parameters were not distinctive, thus a consensus meeting of experts was convened, where each parameter was discussed and voted on to decide on the inclusion as well as weighting of each parameter (from 0 to 10) in the algorithm. In the event of disagreement, further discussions were carried out, and the final consensus was obtained using a simple majority by voting among those present.
Cut-off score of the clinical algorithm
We used a pragmatic approach to obtain a preliminary cut-off score for ‘likely smear negative TB’ vs. ‘unlikely smear negative TB’ by using existing (retrospective) secondary data set of 60 patients from a university hospital. Twenty-nine (48.3%) were confirmed as having smear negative TB using MTB culture, while 31 (51.6%) were not.
We applied the algorithm (including parameter weightings) to both the negative and positive cases, calculated their mean scores with 95% confidence intervals (CIs), and performed an independent samples t-test to determine any differences between the two. Additionally, we ran a receiver operating curve (ROC) analysis to determine the overall discriminative power based on the area under the curve (AUC) and its 95% CI. We then referred to a coordinates of the curve table to identify the optimal cut-off point based on Youden Index and sensitivity value [31]. Lastly, we calculated the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for the selected cut-off point.
We performed all statistical analysis in SPSS, version 27 (IBM Corp., Armonk, NY, USA).
Final review and agreement of the clinical algorithm
We circulated the draft version of the weighted clinical algorithm with the cut-off point to the experts via email, presenting the process of how the final algorithm was established, as well as the sensitivity, specificity, PPVs, and PNVs. We then asked participants whether they agreed with the final algorithm and invited further comments, which we then reviewed and incorporated, if relevant, into the final version of the algorithm.
RESULTS
Twenty-three (85.2% of the 27 identified and invited experts consented to participate (Figure 1), all of whom were from Malaysia. Twenty-two (95.6%) participated in all the rounds, and one dropped out after round 1. Only eight experts (34.8%) comprising pulmonologists, family medicine specialists, and a policymaker attended the hybrid consensus meeting. Two specialties (radiology and microbiology) were not represented at this meeting. We emailed the algorithm with the weightings and the computation method to all remaining 15 experts to elicit their inputs. All replied promptly with no additional comments, and all agreed unanimously to the final algorithm without any further changes.
Flow diagram of expert participation in the modified Delphi process.
We identified fifty-four parameters from round 1, categorising them by ‘sociodemographic backgrounds’, ‘risk factors’, ‘illness history’, ‘physical examination’, ‘laboratory investigations’, and ‘radiological investigations’ (Online Supplementary Document). After round 2, only 23 parameters were retained. All parameters under ‘laboratory investigations’ were dropped. These 23 parameters were then scored (0–100) in round 3; the mean score of each parameter ranged from 61.5 to 88.1, while the overall mean score across all parameters was 75.3 (standard deviation = 7.95), indicating moderate variability in parameter weightings The mean scores of the parameters were not distinctive, including the CXR parameters, which were hypothesised to have a higher weighting in predicting SNPTB. Seven out of the 23 parameters were dropped in the hybrid consensus meeting, but five new ones were added under the CXR category to improve clarity. This led to a final algorithm of 21 parameters with the categories ‘sociodemographic background’, ‘risk factors’, ‘illness history’, and ‘CXR characteristics and location’. The weightings allocated for each parameter ranged from 1 to 10 (Figure 2).
*The final clinical algorithm for SNPTB with scoring system. This figure illustrates a weighted, point-based clinical scoring algorithm developed to aid the diagnosis of SNPTB in symptomatic patients with negative sputum smear microscopy. The algorithm is intended for use in resource-limited settings to support clinical decision-making when rapid molecular diagnostics are unavailable. It integrates four domains: socio-demographic factors (Panel A), clinical risk factors (Panel B), illness history (Panel C), and chest radiograph (CXR) findings (Panel D), including both radiographic characteristics and anatomical location. Each parameter is assigned a predefined weighting based on expert consensus. †Each parameter is scored independently. ‡For CXR, the scores can be more than one according to the presence of the described lesion(s). §CXR with bronchiectasis features will require further clinical work-up. ¶The total score is the sum of the total weightings. ║A total score >19 indicates likely TB, while a score ≤19 indicates unlikely TB. The scoring should take only 2–5 minutes to complete. CXR – chest x-ray, IH – illness history, RF -risk factors, SD – sociodemographic.
After applying the parameter weightage to the 60 patients’ records, the mean total score was 11.8 (95% CI = 9.6–14.0) among negative cases and 28.4 (95% CI = 26.6–30.2) among positive cases. An independent samples t test demonstrated a difference in mean scores between the two groups (P < 0.001), while the ROC analysis indicate the clinical algorithm achieved an AUC of 0.88 (95% CI = 0.79–0.97) (Figure 3). Based on the coordinates of the curve table, a cut-off score of 19.5 yielded a Youden index of 0.636, sensitivity of 86.2%, specificity of 77.4%, PPV of 78.1%, and NPV of 85.7% (Table 3). All experts (100%) agreed to this version of the clinical algorithm-based scoring system and the proposed cut-off score of 19.5.
ROC curve of the clinical algorithm generated based on the 60 patient records. The ROC curve illustrates the discriminative performance of the weighted clinical algorithm applied to 60 patient records, comparing smear-negative pulmonary tuberculosis cases with non-TB controls. The AUC was 0.88 (95% CI = 0.79–0.97), indicating good diagnostic accuracy. ROC – receiver operating characteristic.
DISCUSSION
In this modified Delphi study, we developed a 21-parameter clinical algorithm to diagnose SNPTB in Sabah state, Malaysia. This algorithm included sociodemographic, risk factor, illness history, and CXR parameters, achieved an AUC of 0.88, and, based on a cut-off score of 19.5, yielded a sensitivity of 86.2%, specificity of 77.4%, PPV of 78.1%, and NPV of 85.7%. However, this preliminary cut-off point may change pending the results of a larger prospective validation study to be carried out in Sabah.
Our initial inclusion of three sociodemographic factors after round 3 (immigrant status, close contact with a TB patient, and overcrowding) is consistent with existing literature, in which many sociodemographic characteristics have been associated with developing TB [32–36]. However, many of these studies were country. or context-specific [34–36], and while overcrowding has been cited in some literature as a risk factor for TB transmission in Malaysia [34,37], it was either linked to institutional settings like prisons or poor socioeconomic factors such as poverty and low-cost housing. There are, to our knowledge, no local studies that quantify number of persons per room in relation to overcrowding and TB infection. Overcrowding was dropped as a parameter in our consensus meeting, as the panel decided that its importance was related to ventilation, which is not an important factor in Malaysia in view of the hot tropical climate that necessitates most houses keeping the windows open. Other associated factors, such as being in institutions like prisons, had already been accounted for in the algorithm.
Six symptoms identified after round 3 were cough duration more than two weeks, haemoptysis, weight loss >5% over 6–12 months, anorexia, fever, and productive cough. The panel decided to drop productive cough, consistent with the list suggested by the WHO [38].
CXR has been shown to improve the yield of diagnosis of TB among smear-negative patients, although its sensitivity and specificity by itself is inadequate [39]. The panel agreed that there are two important components in the CXR manifestations that are suggestive of TB, i.e. both the appearance and the location of the lesions, which was supported by literature [40]. It was decided that weightings should be applied separately for these two factors.
Our clinical algorithm was generated for a high TB incidence, but low HIV prevalence setting. We are now validating this algorithm in a prospective study in our setting. However, even when our full validation study is complete, our algorithm will not be appropriate for use in countries with high HIV setting prevalence, as the CXR findings in HIV patients are likely to be atypical.
Our study has produced a context-specific algorithm for the diagnosis of SNPTB in Sabah, based on the knowledge of Malaysian experts. If future validation demonstrates that this algorithm is non-inferior to rapid molecular diagnostic tests, it could contribute to identifying the ‘missing millions’ of people with TB in Sabah, Malaysia. While the presence of experts who developed the other existing algorithms in low- and middle-income countries may have been beneficial, our algorithm was created for Sabah and thus may not be generalisable to other such context, like those with a high HIV prevalence. The low participation of the experts, along with the absence of radiologist and microbiologist in the consensus hybrid meeting, could have affected the robustness of the algorithm. Lastly, we used a data set of 60 individuals in an urban university hospital for the provisional algorithm (before the full validation study), which may have limited generalisability.
The developed clinical algorithm is intended for use by doctors in primary care settings, particularly in resource-limited areas with restricted access to GeneXpert facilities. It is easy to use and only takes 2–5 minutes to complete. As CXR is a major component of this algorithm, it is important that to ensure its interpretations by primary care doctors are accurate, as radiologist review is not feasible due to limited human resources. Regular training workshops and periodic audits should thus be conducted to enhance the reliability and consistency of CXR interpretation.
CONCLUSIONS
In our preliminary study, we present a clinical algorithm to diagnose SNPTB in resource-constrained settings that have no or limited access to GeneXpert and culture. The algorithm is currently being validated in a larger study.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global tuberculosis report 2024. Geneva, Switzerland: World Health Organization; 2024. Available: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024. Accessed: 30 December 2024.
- 2World Health Organization. Global tuberculosis report 2023. Geneva, Switzerland: World Health Organization; 2023. Available: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023. Accessed: 30 December 2024.
- 3World Health Organization. The End TB strategy. Geneva, Switzerland: World Health Organization; 2015. Available: https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19. Accessed: 30 December 2024.
- 4Department of Statistics Malaysia. Sustainable Development Goals. Available: https://www.dosm.gov.my/portal-main/article/sustainable-development-goals. Accessed: 26 March 2025.
- 5Goroh MM Rajahram GS Avoi Rvan den Boogaard C William T Ralph AP Epidemiology of tuberculosis in Sabah, Malaysia, 2012–2018. Infect Dis Poverty. 2020;9:119. 10.1186/s 40249-020-00739-732843089 PMC 7447595 · doi ↗ · pubmed ↗
- 6Ministry of Health Malaysia. Management of tuberculosis. 4th ed. Putrajaya, Malaysia: Ministry of Health Malaysia; 2021. Available: https://www 2.moh.gov.my/moh/resources/Penerbitan/CPG/Respiratory/CPG-_Management_of_Tuberculosis_%284th_Edition%29.pdf. Accessed: 17 November 2025.
- 7World Health Organization. Treatment of tuberculosis: guidelines for national programmes. 3rd ed. Geneva: World Health Organization; 2003. Available: http://apps.who.int/iris/bitstream/10665/67890/1/WHO_CDS_TB_2003.313_eng.pdf. Accessed: 17 November 2025.
- 8Van’t Hoog A Viney K Biermann O Yang B Leeflang MMG Langendam MW Symptom- and chest-radiography screening for active pulmonary tuberculosis in HIV-negative adults and adults with unknown HIV status. Cochrane Database Syst Rev. 2022;3:CD 010890.35320584 10.1002/14651858.CD 010890.pub 2PMC 9109771 · doi ↗ · pubmed ↗