Oral preexposure prophylaxis use and the risk of bacterial sexually transmitted infections and HIV among African women: A prospective observational cohort study
David Mukasa, John Kinuthia, Allison Meisner, Daniel Matemo, Torin Schaafsma, Jennifer Morton, Cynthia Wandera, Elvira Budiawan, Valarie Kemuto, Cherotich Irine, Stephen Odhiambo, Mercy Bii, Beatrice Oduor, Esther Achieng, Tessy Oyombra, Ugochinyere Vivian Ukah

TL;DR
This study found that using HIV preexposure prophylaxis (PrEP) among African women did not increase the risk of bacterial STIs, and HIV incidence was low among consistent PrEP users.
Contribution
The study provides novel evidence on PrEP use and STI risk in African women, showing no increased STI risk and highlighting missed HIV prevention opportunities.
Findings
PrEP use was not associated with increased STI risk compared to non-users.
Chlamydia accounted for 87.7% of STI diagnoses during follow-up.
No HIV infections occurred among consistent PrEP users despite high condomless sex rates.
Abstract
Oral preexposure prophylaxis (PrEP) effectively reduces HIV incidence when used with sufficient adherence, but does not protect against bacterial sexually transmitted infections (STIs). Several studies have documented high rates of bacterial STIs among individuals initiating and using PrEP. We evaluated the association between PrEP use and the risk of STI among African women accessing family planning clinics. We conducted a prospective cohort study nested within a large pragmatic stepped-wedge cluster randomized trial of PrEP delivery in Kenyan family planning clinics, with participant enrollment from June 18, 2021, to May 18, 2023, and follow-up through February 02, 2024 (ClinicalTrials.gov: NCT04666792). The study population included sexually active HIV–negative women aged ≥15 years at elevated HIV risk per Kenyan PrEP guidelines. Participants were offered standard-of-care oral PrEP…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
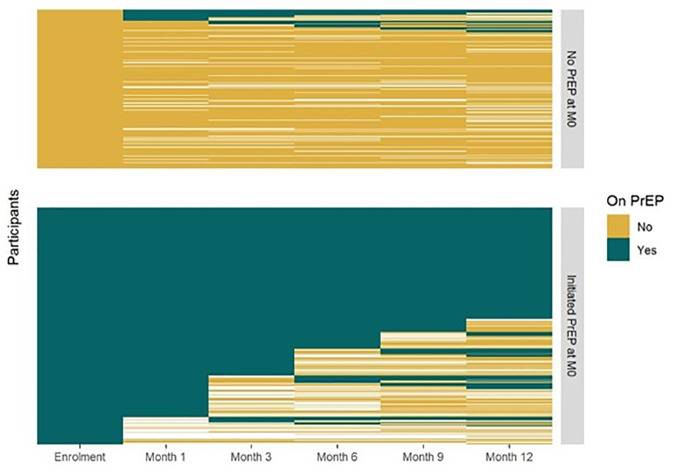 Fig 1
Fig 1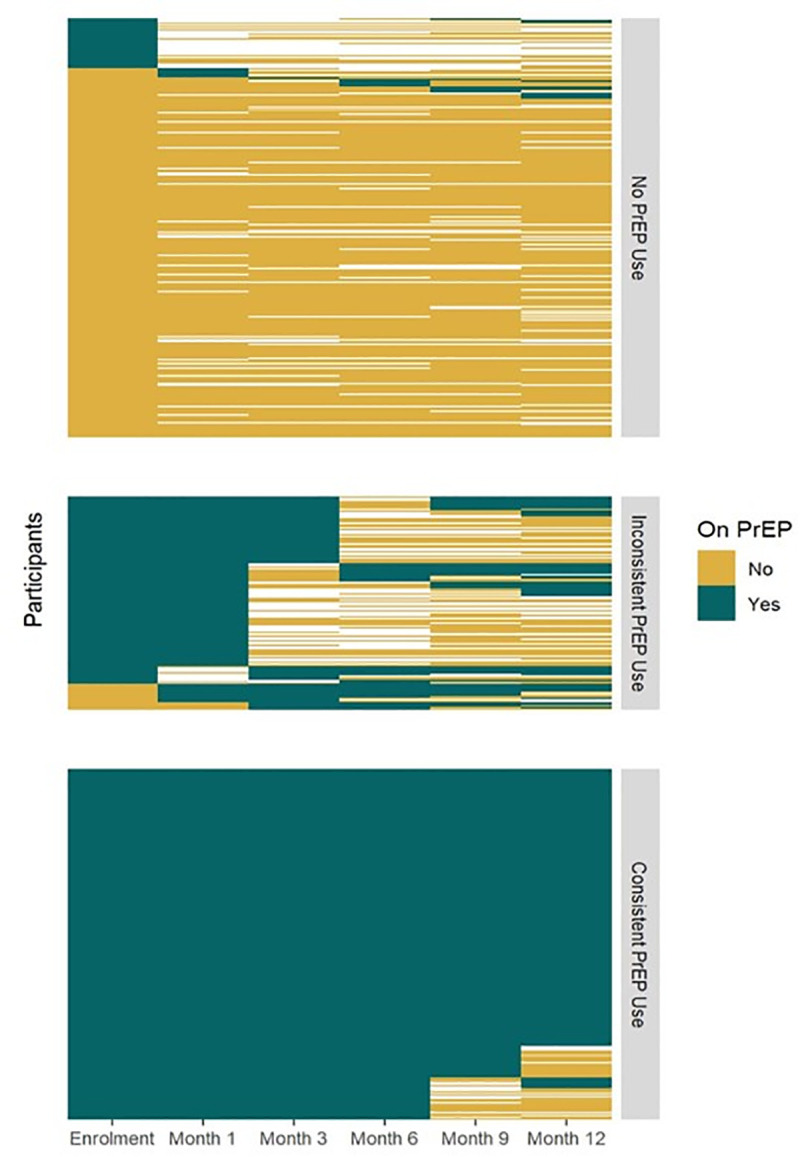 Fig 2
Fig 2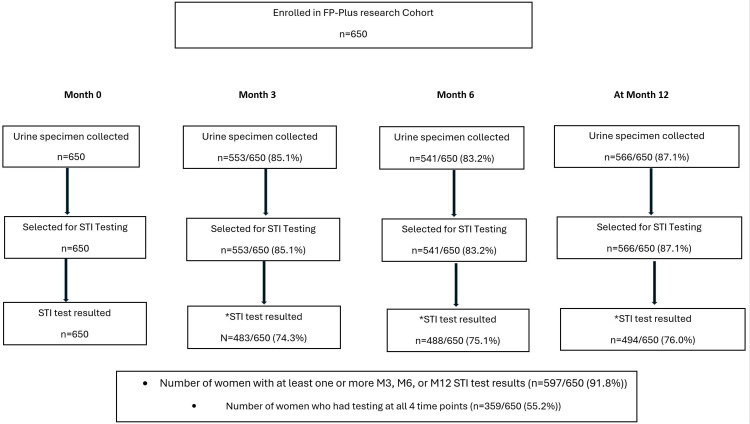 Fig 3
Fig 3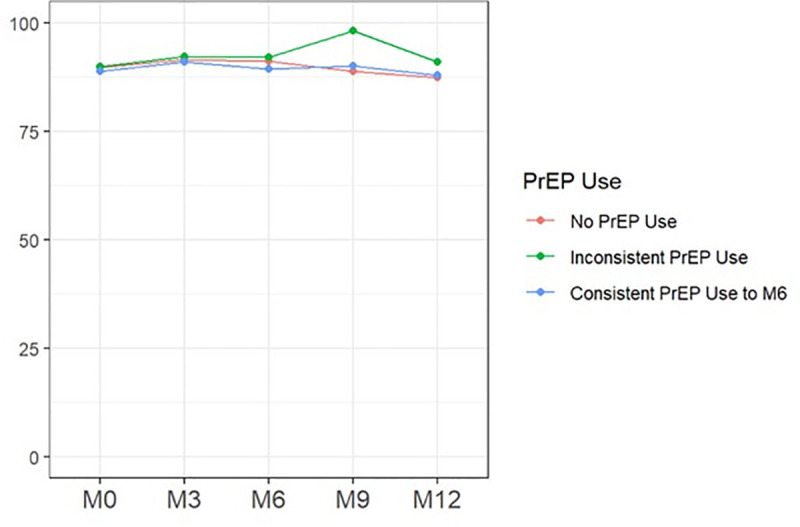 Fig 4
Fig 4- —http://dx.doi.org/10.13039/100000025National Institute of Mental Health
- —http://dx.doi.org/10.13039/100000025National Institute of Mental Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS oral health manifestations · HIV/AIDS Research and Interventions · Reproductive tract infections research
Introduction
The HIV epidemic continues to pose significant public health challenges, particularly in sub-Saharan Africa [1], where women bear a disproportionate burden of the disease [2]. At the same time, African women also face a disproportionate burden of sexually transmitted infections (STIs), including high rates of curable bacterial pathogens such as Chlamydia trachomatis and Neisseria gonorrhoeae [3]. Preexposure prophylaxis (PrEP) with daily oral emtricitabine-tenofovir disoproxil fumarate (FTC/TDF) is a highly effective and approved strategy to prevent HIV acquisition when taken with sufficient adherence [4–8]. New, proven longer-acting PrEP options that could help overcome individual-level challenges are also rapidly emerging [9,10]. Although the effectiveness of PrEP against HIV is well established [11–16], all current approved HIV PrEP options do not and were not expected to protect against bacterial STIs.
The burden of STIs is highest in low- and middle-income countries worldwide, and since the beginning of the HIV epidemic, the coexisting epidemics of bacterial STIs and HIV have been recognized in Africa [17–21]. Despite evidence that the increasing STI trends [22] predate the PrEP era [23], as the adoption of oral PrEP for HIV prevention has gradually increased, its role in driving the increased risk for STI infection among individuals using PrEP has become a source of substantial scientific and public health debate. Some studies have suggested that PrEP use may alter an individual’s perceived risk and sexual behavior, potentially increasing exposure to other STIs if condom usage declines among PrEP users—a phenomenon commonly referred to as risk compensation [24,25]. Conversely, individuals who accept PrEP may have a higher perceived risk of HIV and STIs and be more cautious in general, and the increased frequency of medical visits and counseling associated with PrEP could offset that greater overall risk of STIs. Understanding these dynamics is crucial for informing public health strategies and optimizing integrated strategies to prevent HIV and STI transmission.
We hypothesized that among African women at elevated risk for HIV, PrEP use would not be associated with the risk of incident diagnosis of C. trachomatis and/or N. gonorrhoeae during follow-up. The overall aim of this prospective cohort study was to examine the association between PrEP use and the risk of C. trachomatis and N. gonorrhoeae diagnosis among African women who were assessed to be at elevated risk for HIV based on the Kenya PrEP guidelines.
Methods
Study design
Between June 18, 2021, and February 02, 2024, we conducted a prospective observational cohort study nested within a large pragmatic oral PrEP implementation project (the FP Plus Project). Participants in the nested cohort were enrolled between June 18, 2021, and May 18, 2023, with follow-up continuing through February 02, 2024. The details of the parent study protocol and methods are published elsewhere [26]. Briefly, the FP Plus Project was a stepped-wedge cluster randomized trial to integrate oral PrEP delivery in 12 public health family planning clinics in Kenya (ClinicalTrials.gov: NCT04666792). The overall goal of the parent stepped-wedge project was to catalyze scale-up of integrated oral PrEP delivery within public FP clinics using existing infrastructure and staff. The program was built for all HIV–negative women 15–49 years accessing the participating clinics. The intervention for the stepped-wedge design included technical support to the clinics and training of FP clinic staff to build their capacity to deliver integrated PrEP services as part of routine services in FP clinics. Within the large Stepped-wedge programmatic project, we enrolled a nested observational cohort of women not living with HIV but assessed by the FP clinic staff to be at elevated risk for HIV and eligible for PrEP. The overall goal of the nested cohort was to measure detailed individual-level outcomes on HIV prevention behavior, and STI burden, incident HIV, and PrEP use patterns. Both women who initiated PrEP and those eligible for PrEP but who chose not to initiate PrEP were eligible to be enrolled and followed up for 12 months. This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline (S1 Checklist).
Study population and setting
We enrolled 650 sexually active women who were not living with HIV and were accessing family planning services in the Kisumu area of Kenya, a region with an HIV prevalence of 28% among young women. Eligibility for the observational cohort was based on being ≥15 years old, sexually active, able and willing to provide consent for follow-up in the cohort, not known to live with HIV, and having at least one behavior and epidemiological factor defined by the Kenya PrEP guidelines to indicate a substantial ongoing risk of acquiring HIV. These behavior and epidemiological factors are the same indicators for PrEP eligibility defined by the Kenya PrEP guidelines and include: a) inconsistent condom use; b) having a sex partner(s) who is high risk and whose HIV status is unknown; c) engaging in transactional sex; d) ongoing intimate partner violence and gender-based violence; e) recent bacterial STI; f) recurrent use of post-exposure prophylaxis; g) recurrent sex under the influence of alcohol/recreational drugs; and h) injection drug use with shared needles and/or syringes [27]. At recruitment, all women were offered oral PrEP for HIV prevention by the Ministry of Health (MOH) staff as part of the standard of care. Within the large PrEP program, women assessed to be eligible for PrEP by the MOH staff were offered same-day PrEP initiation as part of the standard of care. Nearly 96% of all those who initiated PrEP started it on the first encounter they were deemed eligible for PrEP. Similarly, women eligible and interested in participating in the cohort were typically enrolled on the same day they were first assessed to be eligible for PrEP. PrEP medications and HIV testing kits were provided by the Kenya national stock of antiretrovirals from the Kenya Medical Supply Authority (KEMSA) as part of the national PrEP scale-up program. PrEP has regulatory and normative guidance sanctions in Kenya and is defined as part of standard care [28–37]. PrEP was provided at initiation, at one month, and quarterly, with the last refill provided 12 months after initiation.
Facility selection
The nested cohort study was conducted at five of the 12 family planning clinics participating in a large stepped-wedge programmatic project in Kisumu County, Kenya. Clinic selection for the large Stepped-wedge PrEP program was based on high client volume, readiness to participate, catchment area to capture the diversity that represents the geographic, economic, and demographic characteristics of all women accessing family planning services, and breadth among the clinic staff. For the nested cohort, the five clinics were all high-volume clinics selected from the 12 clinics participating in the stepped-wedge program, based on feasibility to efficiently enroll and space availability to conduct research procedures.
Follow-up and data collection
Enrolled women had research visits at enrollment and 1, 3, 6, 9, and 12 months, with HIV testing at each visit. HIV testing was performed in line with the Kenya national HIV testing algorithms, using Determine HIV-1/2 and Fast Response test kits. At each scheduled visit, structured questionnaires were administered to obtain demographics, PrEP use status, HIV risk, contraception method, and HIV prevention methods use. Urine samples were tested for N. gonorrhoeae and C. trachomatis using the GeneXpert CT/NG real-time PCR assay (Cepheid, CA, USA) for all participants at baseline and for a randomly selected subset at 3, 6, and 12 months due to logistical constraints. With additional funding, 83%–87% of archived urine samples from randomly selected participants were tested, and 91.8% of women had at least one or more follow-up STI test results. This ensured that sample sizes remained close to the calculated minimum and minimized anypotential impact on the analyses. In addition, the sample included all participants aged ≥15 and all who had a baseline infection. At each visit participants received comprehensive counseling on HIV and STI risk reduction, including provision of condoms and testing for HIV in accordance with national guidelines. Within the large PrEP program, PrEP delivery was done by MOH clinic staff, and PrEP was provided to clients including cohort participants for free as part of standard of care services. At the end of the study, cohort participants using PrEP continued to receive PrEP services at the clinics as part of standard of care services. All research procedures for the cohort activities were conducted by study-dedicated staff.
Measurement of exposure of interest and outcome
Study participation required individuals to be eligible for oral PrEP based on the Ministry of Health PrEP guidelines, and both women who accepted and those who declined PrEP were eligible to be enrolled. The primary PrEP exposure was ascertained through both self-reported quantitative questionnaires on PrEP use and validated with clinic visit attendance and PrEP pharmacy refill records. PrEP exposure status was categorized in two ways to better triangulate PrEP exposure classification throughout the 12 months period (Figs 1 and 2). First, the primary exposure of interest was categorized as a binary variable based on PrEP initiation status ascertained at enrollment (i.e., initiated or not). Second, given that PrEP use is dynamic, and users may cycle on and off PrEP, and those who initiate may go off PrEP just after initiation, conditioned on baseline PrEP initiation status, we also classified PrEP use exposure based on consistency of PrEP use during the first 6 months since enrollment with three categories: never used PrEP at all, inconsistently on PrEP, and consistently on PrEP. In the primary analysis with the binary PrEP use exposure, the outcome was the number of etiological STI diagnoses of C. trachomatis or N. gonorrhoeae during the 12-month follow-up. For the second PrEP exposure variable based on the consistency of PrEP use through 6 months, the outcome was based on the number of etiological STI diagnoses of C. trachomatis or N. gonorrhoeae ascertained at months 6 and 12. For logistical reasons, real-time etiological testing for chlamydia and gonorrhea was conducted only at baseline. Participants diagnosed with chlamydia and gonorrhea at baseline were given their results and received treatment per the Ministry of Health standard of care and were also provided with expedited partner STI testing and therapy services. During follow-up period, only standard-of-care syndromic diagnosis and treatment were done, but at each visit, urine was collected and archived. Thus, testing for urine samples collected at months 3, 6, and 12 was conducted after the study ended and those results were not returned to study participants. Tenofovir diphosphate levels in dried blood spots among a subset of clients on oral PrEP were not available at time of analysis of the cohort and are not included in the current study. The secondary outcomes were incident HIV infection and follow-up sexual behaviors, which included condomless sex at last sex, sex with any new partners in the past 3 months, and multiple sex partners. HIV testing was performed at each scheduled visit, at enrollment, and 1, 3, 6, 9, and 12 months following the Kenya national HIV testing algorithm, using Determine HIV-1/2 and Fast Response test kits. Sexual behavior outcomes were ascertained through questionnaires administered at enrollment and 3, 6, 9, and 12 months.
Preexposure prophylaxis use categorization (PrEP initiation at enrollment).Figure depicts PrEP usage patterns over 12 months, with assessments at each study visit: enrollment, month 1, and quarterly thereafter. Each horizontal line represents one participant, color-coded by PrEP use status (green = yes, gold = no, white = missing data). Figure categorizes participants by PrEP initiation at enrollment: 389 (60%) initiated. Each row represents an individual participant and each column a study visit month. The figure visualizes individual repeated measures; due to the large participant-by-visit structure, these underlying values are not interpretable in table form. The heat map displays temporal patterns in PrEP initiation, continuation, and switching patterns.
Preexposure prophylaxis use categorization (PrEP use through M6 (3 categories)).Figure depicts PrEP usage patterns over 12 months, with assessments at each study visit: enrollment, month 1, and quarterly thereafter. Each horizontal line represents one participant, color-coded by PrEP use status (green = yes, gold = no, white = missing data). Figure categorizes participants by PrEP use through M6: non-users (if initiated, did not refill; 277 [43%]), inconsistent users (≥1 refill, with gaps; 141 [22%]), or as consistent users (n = 232 [36%]). Each row represents an individual participant, and each column a study visit month. The figure visualizes individual repeated measures; due to the large participant-by-visit structure, these underlying values are not interpretable in table form. The heat map displays temporal patterns in PrEP initiation, continuation, and switching patterns.
Statistical analysis
The sample size was calculated for the cohort study to investigate the association between PrEP use and the risk of sexually transmitted bacterial infections. We aimed to detect a relative risk (RR) of 1.5 when the probability of STI infection among women who declined PrEP use is 0.2 and with α = 0.05 and β = 0.20. The estimated sample size per group was 294 (a minimum total sample size of 588). 650 were enrolled to account for potential 10% attrition. The sample size was calculated using SAS version 9.4 (SAS Institute, Cary, NC). We used stratified sampling based on the primary exposure status to ensure an equal sample size in both the exposed and unexposed groups, though the exposed group in the study was slightly larger than the unexposed group. The primary hypothesis was that PrEP use is associated with the risk of incident C. trachomatis and/or N. gonorrhoeae diagnosis. A prospective statistical analysis plan was finalized prior to data analysis (Statistical Analysis Plan in S2 File). Analytic methods were guided by the study objectives, existing literature, and established epidemiologic principles. Analyses performed, including adjustments and sensitivity analyses, are explicitly described. Analytic refinements made during manuscript revision in response to peer review and the rationale included refining covariate adjustment to strengthen epidemiologic validity, assess robustness through sensitivity analyses, and improve transparency regarding missing data, clustering, and analytic assumptions.
Descriptive statistics were used to summarize sociodemographic, PrEP use status, and sexual behaviors. Categorical variables were summarized as frequencies and percentages, and non-normal continuous variables as medians and interquartile ranges. We used modified Poisson generalized estimating equation (GEE) models with robust standard errors with a working independence correlation matrix to estimate the RR and 95% confidence intervals (95% CIs) of infection with chlamydia or gonorrhoeae during follow-up by self-reported PrEP status [38]. GEE accounted for repeated observations per woman and clustering by clinic. Notably, clinic-level intracluster correlation coefficients were minimal to undetectable (0–0.0015), indicating negligible within-clinic correlation.
Pre-planned subgroup analyses were conducted within age categories and among those with STI diagnosis or treatment in 6 months pre-enrollment, STI at enrollment, and any contraceptive use at enrollment. As appropriate all models were adjusted for baseline covariates determined apriori potential confounders based on Directed Acyclic Graphs principles, which included age ≤24, STI diagnosis at enrollment, any contraceptive use, more than one sexual partner, education status, marital status, last partner HIV status, any transactional sex in 3 months pre-enrollment, and clinic site, all selected a priori. The adjusted models for the association between the primary exposure and secondary sexual behavioral outcomes included age, marital status, education status, and clinic site. Age was dichotomized at 24 years to distinguish young adults (15–24 years), a population that bears the greatest burden of HIV and STI in sub-Saharan Africa and is consistently identified in the literature as having lower PrEP awareness, uptake, and adherence and higher HIV incidence compared with older adults [2,39–41]. This cut-point aligns with definitions used by UNAIDS and CDC to characterize adolescents and young adults in HIV prevention research. All participants, including those with a baseline STI diagnosis, were included in this model, but only subsequent STI diagnoses were considered as events in the analysis. Three STI outcome measurement time points (i.e., 3, 6, and 12 months) were included in the primary analysis models based on the binary baseline PrEP initiation exposure.
For models using PrEP use exposure defined by PrEP consistency through 6 months (multi-category exposure); only STI outcome measurements ascertained at 6 and 12 months were included in the analysis. Behavioral outcomes were likewise evaluated at 3-, 6-, and 12-month visits to align with the 3-month recall period for these measures. We used a complete case analysis approach since the proportion of missing data was low (<1% for most covariates). Levels of missingness did not differ meaningfully by PrEP initiation status or by STI outcome categories. Variables with unreliable reporting (e.g., income) were excluded from adjusted analyses, and indeterminate STI test results were excluded from the analysis. Secondary outcomes included pathogen-specific STI diagnoses (C. trachomatis and N. gonorrhoeae), longitudinally assessed sexual behavior measures (condomless sex at last sex, new sexual partners in the past 3 months, and transactional sex), and HIV incidence. These analyses were conducted to provide contextual insight and are interpreted as secondary and exploratory hypothesis-generating. HIV incidence was estimated by dividing the number of new HIV infections by the accrued person-time of follow-up, overall and by PrEP status, with 95% CIs calculated using the Poisson exact method. Statistical analysis was performed using R version 4.4.1 and SAS ver. 9.4 (SAS Institute, Cary, NC).
Ethics approval
The protocol, implementation plan, informed consent forms, data collection tools, and patient education materials were reviewed and approved by the University of Washington Human Subjects Review Committee and the Kenyatta National Hospital-University of Nairobi Ethical Review Committee (ClinicalTrials.gov: NCT04666792). All participants provided written informed consent for all research procedures not related to routine care. Participants received $5 as compensation reimbursement for their time and transportation expenses to participate in the study procedures for study visits.
Results
Participant general characteristics
A total of 650 participants were enrolled, and follow-up over the 12-month period was variable (Fig 3).
*Flow diagram of study participants and sexually transmitted infections testing results received (Patient ID level).Some results were indeterminate/inconclusive after testing. Numbers shown for participants with follow-up STI testing include only those with valid (non-indeterminate) results; indeterminate tests were excluded from outcome analyses.
The median age (IQR) was 26 (23–30) years, and 40% (262/650) were ≤24 years, 81% (526/649) were married, 46% (296/650) had a primary or lower education level, 50% (282/568) had no personal income, and 85% (553/649) reported using at least one contraception method (Table 1). The most frequently used contraception methods at baseline were injectables at 31% (204/649), implants at 22% (143/649), and oral pills at 19% (123/649), as self-reported by the women. Overall, at enrollment, 67% (436/648) of the study participants did not know the HIV status of their primary sexual partner, and the HIV status of the person they last had sex with was unknown in 78% (504/645) (Table 1).
Table 1: Baseline characteristics stratified by baseline oral preexposure prophylaxis (PrEP) initiation status.
Oral PrEP uptake and use patterns
The heat map displaying the classification and patterns of reported PrEP use is presented in Fig 1 and 2. Overall, of 650 women, 60% (389/650) accepted PrEP while 261 declined PrEP at baseline. During follow- up, 14.6% (38/261) of women who initially declined subsequently started PrEP post-enrollment, translating into a total of 427 of 650 (65.7%) who ever initiated PrEP during the study period. Considering PrEP use patterns in the first 6 months, 42.6% (277/650) of women never started PrEP at all, 21.7% (141/650) inconsistently used PrEP while 35.7% (232/650) reported consistent PrEP use. Among women who initiated PrEP at baseline, 14.7% (57/389) discontinued PrEP but later restarted. Among those who reported inconsistent PrEP use, 36.2% (51/141) had only one refill visit after starting PrEP.
Oral PrEP initiation, PrEP use consistency, and STI diagnosis through 12 months
During the 12-month follow-up, 608 women had urine collected for STI testing on at least one follow-up visit (i.e., 3, 6, or 12), of whom 597 had at least one NAAT test result (Fig 3). Among women with at least one NAAT result (n = 597), 19.1% (114) had at least one STI diagnosis: 19.2% (68/354) among women who initiated PrEP at baseline compared to 18.9% (46/244) among women who declined PrEP (adjusted relative aRR:1.11, 95%CI: 0.76–1.61; p = 0.580 (Tables 2 and S3). Overall, 11% (74/650) had an STI diagnosis at baseline: 9.9% (23/232) of those who consistently used PrEP, 9.2% (13/141) of those who inconsistently used PrEP, and 14% (38/277) of those who declined PrEP (S1 Table). Similarly, the frequency of any STI diagnosis was not different based on the reported consistency of PrEP use through 6 months: any STI was diagnosed in 6.0% (12/200) of women who were consistently on PrEP (aRR: 0.56, 95%CI: 0.27–1.19; p = 0.130), 16.5% (17/103) of women who were inconsistently on PrEP (aRR: 1.43, 95%CI: 0.73–2.77; p = 0.290) compared to 12.7% (25/197) of women who never used PrEP at all during follow-up (S2 Table). Chlamydia accounted for 87.7% (100/114) of the women who received at least one STI diagnosis (Table 2). The overall effect was consistent with etiology-specific rates for chlamydia and gonorrhea diagnoses (S2 Table).
Table 2: STI diagnosis through 12 months by oral PrEP initiation status at enrollment.
Sexual behaviors and association with oral PrEP use
Fig 4 shows patterns in the proportion of women reporting condomless sex at the last sex encounter by PrEP use status.
Percent of participants reporting condomless sex at last sex.The percentage of participants reporting condomless sex at last sexual encounter was assessed at baseline (M0) and at months 3(M3), 6 (M6), 9 (M9), and 12 (M12). Estimates are stratified by PrEP use classification: no PrEP use, inconsistent PrEP use, and consistent PrEP use through month 6. Values represent the proportion of respondents within each group reporting condomless sex at each time point.
Overall, the frequency of condomless sex was high in the study population starting at baseline and remained high during the 12-month follow-up. Specifically, the proportion of women reporting condomless sex at the last sex encounter at baseline, 6, and 12 months was 89% (576/644), 90% (491/543), and 88% (489/554), respectively, which was not different between women who initiated versus those who declined PrEP at baseline (aRR: 0.99, 95% CI 0.73–1.35; p = 0.958). In contrast, sex with any new partners in the past 3 months (aRR: 1.54, 95% CI 1.01–2.37; p = 0.047) and multiple sex partners (aRR: 1.05, 95% CI 1.01–1.09; p = 0.0128) were reported more frequently among women who initiated compared to those who declined PrEP.
Similarly, during the 12 months of follow-up, there was no association between frequency of condomless sex at the last sex and PrEP use consistency through 6 months. Compared to women who never used PrEP at all during follow-up, the RR estimates were (aRR: 1.02, 95%CI: 0.73–1.43; p = 0.9138) for women consistently on PrEP and (aRR: 0.77, 95%CI: 0.53–1.12; p = 0.1688) for women inconsistently on PrEP. On the other hand, PrEP use through 6 months was associated with any new sex partners within the past 3 months: (aRR: 1.55, 95%CI: 0.99–2.43; p = 0.0538) for women consistently on PrEP and (aRR: 1.67, 95%CI: 1.01–2.74; p = 0.0447) for women inconsistently on PrEP. The association was also observed between PrEP use through 6 months and multiple sex partners: (aRR: 1.05, 95% CI: 1.01–1.10; p = 0.0157) for women consistently on PrEP and (aRR: 1.07, 95% CI: 1.019–1.12; p = 0.0056) for women inconsistently on PrEP compared to women who never used PrEP. Baseline associations between covariates and STI infection were examined to contextualize adjusted models but are presented in S3 Table to maintain focus on the primary exposure of interest (PrEP initiation).
HIV incidence
Overall, a total of 594 person-years of follow-up were accrued with a median follow-up of 12.2 months (IQR: 10.8–12.9). Four women tested HIV–positive during the period, translating to an overall HIV incidence of 0.67 (95% CI: 0.18–1.72) cases per 100 person-years. The HIV incidence was 0.00 (95%CI: 0.00–1.58) cases per 100 person-years among women consistently on PrEP, 0.83 (95% CI: 0.02–4.61) cases per 100 person-years among women inconsistently on PrEP, and 1.25 (95% CI: 0.26–3.66) cases per 100 person-years for women never on PrEP during the first year of follow-up.
Discussion
In this prospective cohort study among African women at substantial risk of HIV acquisition accessing family planning clinics, more than two-thirds used PrEP for HIV prevention at some point during the study period. STI diagnoses were highly concentrated among young women ≤24 years and those who had any STI at baseline, with 87% of the diagnoses due to chlamydia infection. Although STI diagnoses were high, the proportion of participants who had any STI diagnosis was relatively lower compared to what was reported in a randomized controlled trial on doxycycline postexposure prophylaxis (PEP) for cisgender women in the same setting [42]. The differences may be attributed to differences in the study designs, outcome definition, and inclusion criteria. The latter was an intervention study with more restrictive inclusion criteria for participants among women 18–30 years of age who were receiving PrEP against HIV and included Treponema pallidum in the outcome definition [42]. Overall, the one-year HIV incidence in the study population was 0.67 per 100 person-years, and no HIV acquisition occurred in women who reported consistently high adherence to PrEP.
Over the past two decades, the burden of bacterial STIs has increased substantially, coinciding with population-level implementation of emerging HIV prevention options, including oral PrEP and treatment as prevention. A systematic review and meta-analysis of the global epidemiology of STIs among persons using PrEP found a pooled prevalence of 24% for chlamydia, gonorrhea, or early syphilis at PrEP initiation and a pooled incidence rate of 72.2 per 100 person-years during the first three months of PrEP use [43]. In another study conducted among men who have sex with men, the proportion of participants diagnosed with any STI in the past 6 months was high among PrEP users compared to those who were not using PrEP (17.4% versus 8.4%) [44]. On the other hand, studies among female sex workers [45] and women who inject drugs [46] found no evidence and limited evidence for risk compensation, respectively. In sub-Saharan Africa, HIV transmission is predominantly through sexual exposure, and thus, it is not surprising to find a high STI burden in study populations with behavioral factors associated with an increased HIV risk. With the global rise in rates of STIs, the role of PrEP in driving changes in sexual behavior and increased risk for STI acquisition has been a source of substantial scientific and public health debate [47–49]. Some studies have suggested that PrEP use may alter an individual’s perceived risk and sexual behavior, potentially increasing exposure to other STIs if condom usage declines among PrEP users due to risk compensation [24,25]. On the contrary, PrEP users may be more cautious overall and consider themselves to be at a higher risk of HIV and STIs; the increased frequency of PrEP-related medical visits and counseling could offset this increased risk of STIs. Importantly, despite the high frequency of condomless sex and etiological diagnoses of infection with C. trachomatis or N. gonorrhoeae in this study population, we reassuringly found no evidence to suggest that PrEP use is associated with increased risk for STIs among African women at elevated risk for HIV accessing family planning clinics in Kenya.
Oral FTC/TDF PrEP is an effective, recommended, and impactful strategy for HIV prevention when taken with sufficient adherence. Even with self-reported adherence, a clear relationship was observed in this study between higher reported adherence and lower risk of HIV acquisition. In this study population, 78% of women did not know the HIV status of their sexual partners, and 75% of all new HIV acquisitions occurred in women who were offered but declined to initiate oral PrEP. The above results not only represent a missed opportunity but also highlight an urgent need to accelerate access to new PrEP choices for HIV prevention for people for whom daily oral PrEP is challenging or may not be the right prevention option for them. PrEP is an important prevention option for individuals at substantial risk for HIV, including sexual partners of people living with HIV who have not yet achieved full viral suppression. However, because oral PrEP and any currently approved PrEP option are not designed to prevent bacterial STIs, a potential increase in risk taking behavior among those using PrEP has the potential to increase exposure to STIs that can also offset benefits of PrEP. Thus, WHO has called for renewed efforts to provide integrated HIV and STI services [50].
This study included several secondary outcomes and exploratory analyses. These secondary findings should be interpreted cautiously and viewed as hypothesis-generating rather than definitive. Future studies with larger samples and confirmatory analytic designs are needed to validate these associations. There are several strengths and limitations to our study. The study’s strengths include a large prospective cohort of sexually active women, including those on PrEP as well as those at elevated risk of HIV but who declined oral PrEP, extensive etiological N. gonorrhoeae and C. trachomatis testing at multiple time points, and testing in real-world family planning clinic settings, which increases the representativeness of our study population. There are also several limitations to our study. First, this was an observational study, and groups were formed based on self-selection and self-reported oral PrEP use. Secondly, the urine GeneXpert CT/NG NAAT test is a practice testing strategy, particularly for large-scale STI screening programs, but it is not as sensitive for women as self-collected vaginal swab or provider-collected endocervical swabs. In addition, there was no testing for syphilis and Trichomonas vaginosis, and thus, there is a potential for underestimation of the overall STI prevalence. However, there is no impact on the primary question, as the non-testing syphilis or Trichomonas vaginosis applied uniformly across study exposure groups. Thirdly, the data is from family planning clinics, and this may reduce generalizability to other settings. Furthermore, women’s access to STI prevention advice in family planning clinic settings might have affected the outcome. Fourthly, PrEP use exposure was ascertained through a combination of visit attendance, PrEP prescription and dispensing data based on programmatic records extracted by the Ministry of Health staff, and client self-report PrEP use, which is prone to recall and social desirability bias. Fifthly, no objective measure of PrEP use was available, but the observation of a clear relationship between self-reported adherence and risk of HIV acquisition lends confidence to our findings. This was not an efficacy study, and it was not powered to test differences in HIV incidence between PrEP use categories. Recruitment into the nested study was not through random selection, and participants received IRB-approved compensation for their time, which could have introduced the potential for selection bias and reduced the generalizability of findings. Lastly, residual confounding is possible, particularly for covariates that were excluded from adjusted models due to concerns about measurement reliability. Despite these limitations, our large prospective data provides some of the most comprehensive empirical evidence on the association between PrEP use and the risk of bacterial STI infections.
In this large prospective cohort study among Kenyan women with provider-assessed elevated risk for HIV acquisition, 65.7% initiated PrEP. Despite high rates of condomless sex in this study population, we found no evidence to suggest that PrEP use is associated with increased risk for STIs among African women at elevated risk for HIV. No HIV acquisition occurred among women consistently on oral PrEP, but 75% of all new HIV acquisitions occurred in women who declined to initiate PrEP, representing a missed opportunity for HIV prevention.
Supporting information
S1 TableBaseline characteristics stratified by preexposure prophylaxis (PrEP) initiation status.(DOCX)
S2 TableSTI infection at 12 months by PrEP use consistency through month 6 since PrEP initiation (3 categories).(DOCX)
S3 TableAssociation between baseline covariates and STI diagnosis through 12 months.(DOCX)
S1 ChecklistThis checklist is licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0; https://creativecommons.org/licenses/by/4.0/).(DOC)
S1 FileFP Plus Protocol_V3.0.PrEP-aring family planning clinics to streamline integration of HIV prevention services for young women in Kenya. The Family Planning plus HIV prevention (FP-Plus) Project.(PDF)
S2 FileFP Plus Statistical Analysis Plan_V1.0.(PDF)
S3 FileS1 Supplementary materials.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torrone EA, Morrison CS, Chen P-L, Kwok C, Francis SC, Hayes RJ, et al. Prevalence of sexually transmitted infections and bacterial vaginosis among women in sub-Saharan Africa: an individual participant data meta-analysis of 18 HIV prevention studies. P Lo S Med. 2018;15(2):e 1002511. doi: 10.1371/journal.pmed.1002511 29485986 PMC 5828349 · doi ↗ · pubmed ↗
- 2US Preventive Services Task Force, Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, et al. Preexposure prophylaxis for the prevention of HIV infection: US preventive services task force recommendation statement. JAMA. 2019;321(22):2203–13. doi: 10.1001/jama.2019.6390 31184747 · doi ↗ · pubmed ↗
- 3Antiretroviral TS. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. World Health Organization. 2015.26598776 · pubmed ↗
- 4Blackwell CW. Preventing HIV infection in high-risk adolescents using preexposure prophylaxis (Pr EP). J Assoc Nurses AIDS Care. 2018;29(5):770–4. doi: 10.1016/j.jana.2018.06.001 30146018 · doi ↗ · pubmed ↗
- 5Hosek SG, Rudy B, Landovitz R, Kapogiannis B, Siberry G, Rutledge B, et al. An HIV preexposure prophylaxis demonstration project and safety study for young MSM. J Acquir Immune Defic Syndr. 2017;74(1):21–9. doi: 10.1097/QAI.0000000000001179 27632233 PMC 5140725 · doi ↗ · pubmed ↗
- 6AVAC. The future of ARV‐based prevention and more. 2024. [cited 2024 July 29]. Avilable from: https://avac.org/resource/infographic/the-future-of-arv-based-prevention-and-more/
- 7Grulich AE, Guy R, Amin J, Jin F, Selvey C, Holden J, et al. Population-level effectiveness of rapid, targeted, high-coverage roll-out of HIV pre-exposure prophylaxis in men who have sex with men: the EPIC-NSW prospective cohort study. Lancet HIV. 2018;5(11):e 629–37. doi: 10.1016/S 2352-3018(18)30215-7 30343026 · doi ↗ · pubmed ↗
- 8Grant R, et al. Scale-up of pre-exposure prophylaxis in San Francisco to impact HIV incidence. Seattle, WA; 2015.