Antimicrobial resistance, characterization, and knowledge practices of Salmonella spp. infection in under-five children with acute gastroenteritis at Levy Mwanawasa University Teaching Hospital, Lusaka Zambia
Namwezi Namuchimba Kapembwa, Flavien Nsoni Bumbangi, Chisanga Chipanta, Kaunda Yamba, Mike Nundwe, Misheck Shawa, John Bwalya Muma

TL;DR
This study examines Salmonella infections in young children in Zambia, finding high antibiotic resistance and risk factors like poor water and feeding practices.
Contribution
The study provides new insights into antimicrobial resistance patterns and risk factors for Salmonella infections in under-five children in Zambia.
Findings
9.76% of children had Salmonella infections, with 35% of isolates being multidrug resistant.
High resistance to trimethoprim-sulfamethoxazole was observed.
Untreated water and poor feeding practices were identified as risk factors.
Abstract
Salmonella spp. is a major cause of bacterial gastroenteritis worldwide borne from consuming contaminated food or water. The growing incidence of difficult-to-treat Salmonella infections has been heightened by increased AMR due to increased use of antibiotics posing acritical public health challenge. This was a cross-sectional study involving 205 children with AGE at Levy Mwanawasa University Teaching Hospital in Lusaka Zambia, between September 2020 and February 2021. Stool samples were collected and subjected to standard microbiological testing, serotyping, antimicrobial susceptibility testing and molecular confirmation for Salmonella spp. In addition, a questionnaire was administered to participants’ guardians to determine the level of knowledge and practices towards Salmonella infections. Data analysis was performed using Microsoft Excel, GraphPad Prism and WHONET. Twenty…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
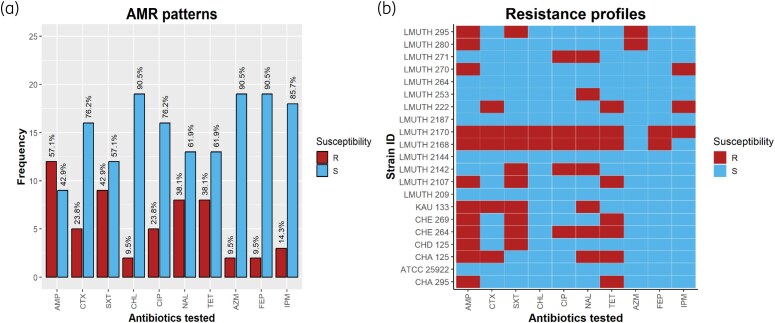 Figure 1
Figure 1| Parameter | Level | Frequency | Proportion (%) |
|---|---|---|---|
| Health status | Diarrhoeic | 187 | 91.2 |
| Non-diarrhoeic | 18 | 8.8 | |
| Gender | Male | 120 | 58.5 |
| Female | 85 | 41.5 | |
| Age (months) | 0–29 | 177 | 86.3 |
| 30–59 | 28 | 13.7 | |
| Education of guardian | Primary | 53 | 25.9 |
| Secondary | 115 | 56.1 | |
| Tertiary | 37 | 18.0 | |
| Location of household | Urban | 203 | 99 |
| Rural | 2 | 1 | |
| Urban density | High | 39 | 19.0 |
| Medium | 144 | 70.2 | |
| Low | 22 | 10.7 | |
| People per household | 0–10 | 199 | 97.1 |
| 11–20 | 6 | 2.9 |
| Potential risk factors for demography | Frequency | Positive (%) |
|
|---|---|---|---|
| Gender ( | |||
| Male | 120 | 13 (10.83) | 0.537 |
| Female | 85 | 7 (8.24) | |
| Age (months) ( | |||
| 0 to 29 | 177 | 17 (9.60) | 0.854 |
| 30 to 59 | 28 | 3 (10.71) | |
| Education of guardian ( | |||
| Primary | 53 | 6 | 0.606 |
| Secondary | 115 | 12 | |
| Tertiary | 37 | 2 | |
| Location of household ( | |||
| Urban | 203 | 19 (9.36) | 0.054 |
| Rural | 2 | 1 (50.00) | |
| Urban density ( | |||
| High | 39 | 7 (17.95) | 0.156 |
| Medium | 144 | 11 (7.64) | |
| Low | 22 | 2 (9.09) | |
| People per household ( | |||
| 0–10 | 199 | 19 (9.55) | 0.563 |
| 11–20 | 6 | 1 (16.67) | |
| Potential risk factors for knowledge | Frequency | Positive (%) | Score |
|
|---|---|---|---|---|
| Do you know antibiotics? ( | ||||
| Yes | 82 | 6 (7.32) | 40 | 0.337 |
| No | 123 | 14 (11.38) | ||
| Do you know what antibiotic resistance is? ( | ||||
| Yes | 35 | 1 (2.86) | 17.1 | 0.131 |
| No | 170 | 19 (11.18) | ||
| Is it acceptable to use antibiotics given by friends or family members as long? ( | ||||
| Yes | 13 | 2 (15.38) | 93.7 | 0.480 |
| No | 192 | 18 (9.38) | ||
| Do you know the causes of diarrhea? ( | ||||
| Yes | 136 | 11 | 66.3 | 0.259 |
| No | 69 | 9 | ||
| Average score on knowledge on | 54.3 | |||
| Potential risk factors for practices | Frequency | Positive (%) | Score |
|
|---|---|---|---|---|
| What is the household’s main source of water for drinking and cooking? ( | ||||
| Pipe | 116 | 8 (6.70) | 94.6 | 0.247 |
| Borehole | 78 | 10 (12.82) | ||
| Other | 11 | 2 (18.18) | ||
| Do you treat or filter drinking water? ( | ||||
| Yes | 68 | 5 (7.35) | 33.2 | 0.271 |
| No | 137 | 17 (12.41) | ||
| Is there livestock at your household? ( | ||||
| Yes | 70 | 6 (8.57) | 65.6 | 0.681 |
| No | 135 | 14 (10.37) | ||
| Is the child breast feeding? ( | ||||
| Yes | 93 | 11 (11.83) | 54.6 | 0.362 |
| No | 112 | 9 (8.04) | ||
| Do you wash your hands before preparing or giving food to the child? ( | ||||
| Yes | 174 | 16 (9.20) | 84.9 | 0.522 |
| No | 31 | 4 (12.90) | ||
| Do you wash hands after disposing off the child's feces? ( | ||||
| Yes | 178 | 15 (8.43) | 86.8 | 0.100 |
| No | 27 | 5 (18.52) | ||
| Where do you normally store the prepared food for the children? ( | ||||
| Store correctly | 148 | 14 (9.46) | 72.2 | 0.818 |
| Do not store | 57 | 6 (10.53) | ||
| What do you use to feed the child? ( | ||||
| Spoon | 9 | 2 (22.22) | 4.4 | 0.197 |
| Hands/fingers/breastfeeding | 196 | 18 (9.18) | ||
| What toilet facility do you have? ( | ||||
| Pit latrine/Flushable toilet | 202 | 19 (9.41) | 98.5 | 0.166 |
| No facility | 3 | 1 (33.33) | ||
| Do you wash hands after going to the toilet? ( | ||||
| Yes | 193 | 18 (9.33) | 94.1 | 0.406 |
| No | 12 | 2 (16.67) | ||
| How do you dispose of your solid waste? ( | ||||
| Bin/Pit | 155 | 15 (9.68) | 75.6 | 0.947 |
| Roadside/Openly | 50 | 5 (10.00) | ||
| Average score on practice towards | 69.5 | |||
- —African Centre of Excellence for Infectious Diseases in Humans and Animals (ACEIDHA)
- —World Bank10.13039/100004421
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalmonella and Campylobacter epidemiology · Child Nutrition and Water Access · Escherichia coli research studies
Introduction
Acute gastroenteritis (AGE) is an inflammation of the intestines causing frequently occurring diarrheal disease with symptoms such as nausea, vomiting and abdominal pain.^1^ Salmonella spp. commonly causes gastrointestinal infection, accounting for 93.8 million foodborne illnesses and 155 000 deaths per year.^2^ Enteric salmonellosis develops after ingestion of contaminated food or water and these infections remain restricted to the gastrointestinal tract.^3^ The most common serovar causing human illness are Salmonella enterica serovar Typhimurium and Salmonella enterica serovar Enteritidis.^4^ Identification of the pathogens responsible for infectious diarrheal diseases is crucial in surveillance, prevention and control.
Diarrhoea is the second largest cause of death in children under 5 years of age globally,^5,6^ and is among the leading causes of preventable deaths among children under 5 years of age in developing countries. Annual incidence (16%) of diarrheal diseases among children <5 years in Zambia ranks among the top five causes of morbidity and mortality in all ages.^7^
Research shows that antibiotic resistance (ABR) in Salmonella is a significant global public health challenge that complicates treatment and contributes to increased morbidity and mortality.^8^ Salmonella has shown increasing resistance to commonly used antibiotics such as ampicillin, chloramphenicol and trimethoprim-sulfamethoxazole.^9^ More so, the rise of MDR strains, particularly Salmonella enterica serovar Typhi and non-typhoidal Salmonella, is associated with severe systemic infections.^8,9^ Misuse and overuse of antibiotics in clinical and veterinary settings are the main factors contributing to the burden of resistant Salmonella. The spread of resistant strains through international travel, trade and the food supply chain further amplifies the problem.^10,11^
The growing incidence of Salmonella infections in Zambia has been compounded by increasing resistance to commonly used antibiotics such as ampicillin, chloramphenicol and cotrimoxazole.^12^ Salmonella MDR strains in both clinical and veterinary settings highlight the role of antibiotic misuse in humans and animals.^9^ This growing resistance threatens the effectiveness of first-line treatments leading to prolonged illness, increased healthcare costs and mortality.^12–14^ Antibiotics constitute the primary treatment for infection caused by Salmonella spp. However, because of the widespread use, there has been a rise in AMR to Salmonella in recent years.^15^ Essentially, the rise of MDR Salmonella strains has highlighted how critical AMR is in public health.
Generally, Salmonella infection places a considerable economic strain on healthcare systems.^16^ The resistance to antibiotics makes standard treatments less effective, potentially leading to prolonged illness and undesirable health outcomes, especially in children with weakened immune systems or underlying health issues.^17^ Therefore, this study aimed to analyse patterns of antimicrobial-resistant Salmonella spp. in children with AGE at Levy Mwanawasa University Teaching Hospital (LMUTH). In addition, the study aimed analyse the levels of knowledge and practices of the guardians.
Methods
Study area
This was a cross-sectional study conducted at LMUTH in children between 0 and 59 months who presented with symptoms of AGE at the outpatient from September 2020 to February 2021. The LMUTH hospital offers specialized services to >1 million people with a bed capacity of 900 and is situated in Lusaka district. The hospital is part of the newly established Levy Mwanawasa Medical University founded as a Public University in 2018.^18^
Sample size
The study population included children with an episode of diarrhoea as Population One (diarrhoeic) and from the same age category, healthy children attending the <5 years clinic as Population Two (non-diarrhoeic). Children already on antibiotics were not included in the study.
The sample size was calculated using AusvetEpi Tools software,^19^ required to detect a statistically significant difference between two proportions with specified levels of confidence and power. Assuming a 95% confidence level, a statistical power of 80% and a 5% absolute error. In addition, a prevalence of 25.5% of Salmonella spp. reported from an earlier study conducted at the University Teaching Hospital,^20^ among children under 5 with diarrheal diseases was assumed. This prevalence was used to calculate the sample size of Population One (diarrhoeic children). It was further assumed that Salmonella spp. would be isolated in Population Two (non-diarrhoeic children) at a prevalence of 1%. On the basis of these assumptions, the estimated sample size was 300.
Sampling
Stool samples of the infants were collected from nappies (fresh stool) using a scoop and placed in stool containers. While from the older children, samples were collected in the sample bottles that were provided. These specimens were then transported in cooler boxes on ice at a temperature of <4°C to the Public Health Laboratory at, University of Zambia for analysis. Unprocessed sample were stored in the fridge at −20°C for 24 hours.
Epidemiological data
In addition, a questionnaire was administered to parents or guardians to collect epidemiological data and determine the level of knowledge and practices towards Salmonella infections.
Isolations and identification of Salmonella species
Using a sterile swab, the stool sample was initially enriched in selenite cystine broth (Oxoid, UK) and aerobically incubated for 24 ± 2 h at 35–37°C. Thereafter, it was subcultured on xylose lysine deoxycholate (XLD) agar (Oxoid, UK) then incubated for 24 ± 2 h at 35–37°C in an aerobic incubator. The XLD plates were examined for presence of colonies suggestive of Salmonella i.e. pink colonies with or without black centres. Subsequently, they were purified on nutrient agar/Muller Hinton agar (Oxoid) before subjection to phenotypic characterization. Presumptive Salmonella isolates were identified using standard biochemical tests. Triple Sugar Iron agar and Lysine Iron Agar were used for biochemical characterization.
Serological typing of Salmonella isolates
Isolates were categorized into serogroups by using group specific antisera (BD Difco) by assessing the presence of distinct ‘O’ and ‘H’ antigens. Thereafter, antibiotic susceptibility testing was performed.
Determination of antimicrobial susceptibility patterns
Antimicrobial susceptibility was determined using the Kirby–Bauer disc diffusion method and interpreted according to the CLSI guidelines of 2016.^21^ The antibiotic discs (Oxoid, UK) included sulfamethoxazole/trimethoprim (1.25/23.75 µg), ciprofloxacin (5 µg), cefotaxime (30 µg), tetracycline (30 µg), nalidixic acid (30 µg), cefepime (30 µg), azithromycin (15 µg), imipenem (10 µg) and chloramphenicol (30 µg). The zones of inhibition were grouped into intermediate (I), resistant (R) and susceptible (S) was based on the M100 CLSI2016 guidelines for Salmonella species. Escherichia coli ATCC 259225922 was used as a quality control strain.
DNA extraction for Salmonella confirmation
Salmonella was confirmed by performing PCR assays to detect the invA gene specific for Salmonella. First, DNA was extracted using the boiling method.^22^ The extracted DNA was then amplified using Salmonella-invA gene specific primers, namely, S139 (5_GTG AAA TTA TCG CCA CGT TCG GGC AA-3_ and S141 (5_ TCA TCG CAC CGT CAAAGG AAC C-3_). Subsequently, the PCR amplification products were electrophoresed in 1.5% agarose gel stained with ethidium bromide for 40 minutes with a constant voltage of 100 V. Finally, the bands were visualized under ultra-violet light alongside a 100 bp DNA ladder.
Data management and analysis
All laboratory data were managed in an Excel spreadsheet. Descriptive statistics on socio-demographic characteristics were performed using GraphPad Prism (version 9.0). Antimicrobial susceptibility (AST) data for isolates and resistance gene detection were analysed, and presented as resistance patterns and profiles. AST data were analysed using WHONET 2021. Results for susceptible, intermediate and resistant strains were presented as proportions and graphs.
Further data from the questionnaire interviews were entered in Excel spreadsheets. Mean scores and percentages were used to determine the level of knowledge and practices. Correct answers were scored as one (1) whereas incorrect answers scored zero (0). The knowledge and practices levels were categorized as high, moderate or low on the basis of predetermined thresholds using Bloom’s cut-off criteria.^23^ According to these criteria, scores >60 indicate a high level of knowledge, attitudes and practices, scores between 25 and 59 represent moderate levels and scores <25 suggest a low level.
Ethical approval
Ethical clearance was sought from Excellence in Research Ethics and Science Converge Institutional Review Board (IRB) committee (IRB Number 00005948), on 31 August 2020. The approval from the National Health Research Authority was obtained (Ref. No. NHRA00010/3/09/2020) and the Provincial and District Health Offices were informed about the study. Consent from guardians was sought in the form of an oral consent script before any sampling was conducted.
Results
Socio-demographic characteristics of study participants
Two hundred and five stool samples were collected from children and evaluated for presence of Salmonella spp. Out of the 205 samples, 187 (91.2%) were diarrhoeic, of which 17 tested positive for Salmonella, while 18 samples (8.8%) were non-diarrhoeic, of which three tested positive for Salmonella. Furthermore, of the enrolled 205 participants, 120 (58.5%) were male and 85 (41.5%), were female. Almost all the participants (203 representing 99%) came from urban areas except two. Furthermore, 39 (19.0%) originated from high density areas, 144 (70.2%) from medium density areas and 22 (10.7%) from low density areas (Table 1). The educational levels of the guardians to the participants were largely at secondary school level.
Analysis of the association between Salmonella infection of the participants and the potential predictors
There was no association between various predictors and knowledge or practices related to Salmonella spp. infection. Specifically, factors such as the participants’ sex (χ^2^ = 0.3815, P = 0.537), age and likelihood of acquiring infection (χ^2^ = 0.03382, P = 0.854), guardians’ level of education (χ^2^ = 1.003, P = 0.606), residence (χ^2^ = 3.715, P = 0.054), residential density (χ^2^ = 3.717, P = 0.156) and the number of people per household (χ^2^ = 0.3353, P = 0.563) showed no significant association (Table 2).
Most guardians did not exhibit knowledge on antibiotics and the meaning of AMR (Table 3). However, a large percentage (72%) of the 205 possessed knowledge on the cause of diarrhoea in children. About 94% of the guardians acknowledged that it was not acceptable to use antibiotics given by friends or family members. Overall, the average knowledge score was moderate.
Most of the participants came from households with access to clean water for use in cooking and drinking. However, a good number, 137 (67%), did not treat or filter their water before use. Most households exhibited good practices towards food preparation, disposing of the child’s faeces, food storage, hand washing after use of the toilet and solid waste disposal bearing a good average practice score (69.5%) (Table 4).
Serotyping
After identification from bacterial culture and biochemical tests, a total of 28 isolates were subjected to Salmonella serotyping using anti-O and anti-H antisera. Out of these, 14 isolates (50%) were positive for both anti-O and anti-H antisera, whereas two isolates (7.1%) were negative for both anti-O and anti-H antisera. Finally, six isolates (21.4%) were anti-O positive, anti-H negative while another six isolates (21.4%) were anti-O negative, anti-H positive.
Antimicrobial susceptibility patterns of Salmonella spp.
The AST patterns of Salmonella spp. in stool samples are illustrated in Figure 1. Most of the isolates (42.9%) showed resistance to trimethoprim-sulfamethoxazole. However, the isolates were largely susceptible to the remaining eight antibiotics tested. According to the results of this study, Salmonella spp. exhibited the highest susceptibility to chloramphenicol, cefepime and azithromycin (90.5%), followed by imipenem (85.7%), ciprofloxacin and cefotaxime (both at 76.2%). Nalidixic acid and tetracycline were at 61.9%. Out of 20 Salmonella isolates identified, only four were susceptible to all tested antibiotics.
Antimicrobial susceptibility patterns (a) and resistance profiles (b) of Salmonella spp. from stool. Abbreviations: AZM, azithromycin; CHL, chloramphenicol; CIP, ciprofloxacin; CTX, cefotaxime; FEP, cefepime; IPM, imipenem; NAL, nalidixic acid; SXT, trimethoprim-sulfamethoxazole; TET, tetracycline (key: R, resistant; S, susceptible). Frequency on the y-axis represents the number of isolates, and percentages on the bars represent the proportion of susceptibility.
Salmonella spp. identification
The Salmonella spp. was confirmed by PCR using the invAgene (Figure S1, available as Supplementary data at JAC-AMR Online). Out of the initial 205 samples, 20 (9.8%) were confirmed Salmonella positive using PCR.
Discussion
This study aimed to analyse patterns of the antimicrobial-resistant Salmonella spp. in children <5 years as well as knowledge and practices of their guardians. This study target to sample 300 children, however, we only managed to sample 205 because it was difficult to access patients, and hospital avoidance by patients was common during the COVID-19 pandemic^24^ when the study was carried out. The prevalence of Salmonella infection was observed to be low compared with what has been observed in other studies, albeit the sample size of the current study was lower.^25,20^ The low prevalence could be possibly due to various factors such as location of the household, as most children came from urban areas where hygienic practices tend to be good. Nonetheless, the diarrhoeic population seemed to have more positive Salmonella infections compared with the non-diarrhoeic population. This observation might have been due to the smaller number of non-diarrhoeic children included in the study. It may also be influenced by the role of asymptomatic carriers in Salmonella transmission. As healthy individuals are ideally expected to have either no Salmonella or a very low prevalence, asymptomatic carriers can still harbour the pathogen and contribute to its spread without showing clinical symptoms.^15^
Salmonella infections are prevalent in communities that usually have low hygiene status and households that have meals prone to contamination.^26^ This is because Salmonella contamination of food is a major problem in such communities.^27,20^ The inadequate WASH strategies coming from limited water access, poor environmental and hygiene, lack of separate, private and secure toilets and washing facilities in LMICs still highlight the need for more interventions.^28^
About 66.8% of the participants did not treat or filter water before drinking, which posed a risk of acquiring Salmonella infection.^29,30^ Furthermore, with about 95.6% of mothers/guardians using hands to feed their children, the likelihood of infection was high since hands normally carry bacteria.^31^ There is a need for safer feeding habits and behavioural change among guardians/caregivers to reduce this risk of Salmonella infections.^32^
Most of the respondents (66.3%) were familiar with the cause of Salmonella infection. This corroborates with findings from another study with similar observations on the participants’ knowledge on the major ways of transmission.^33^ Of the respondents, 93.7% indicated that it was not acceptable to use antibiotics given by friends or family. Despite sufficient access to reliable information sources, the 7.3% gap indicates that there is still need for awareness on antimicrobial use and gene transfer of AMR genes to humans that comes with the misuse of antibiotics. Initiatives such as antimicrobial stewardships using the One-Health framework that accounts for all transmission points are also very important to curb AMR.^34^ This is withstanding the findings of this study showing a significant understanding about the disease as seen from the moderate knowledge score (54.3%) similar to earlier studies (57.8%).^35^
The observed 69.5% practice score on good infection-prevention practices was higher than only 42.3% observed elsewhere.^36^ The good average score for practices related to Salmonella infections indicates good adherence to preventive measures. Besides, studies have reported that good practices, for example, hand washing, show a general common understanding of health risks.^37^
The resistance patterns observed in this study is similar to the findings in observed in others studies, which reported Salmonella spp. being mostly resistant to nalidixic acid and tetracyclines.^38^ Previous research has also reported Salmonella spp. to be resistant to chloramphenicol, sulfamethoxazole, tetracycline and trimethoprim.^39^ There is a need for enhanced approaches for AMR surveillance on Salmonella spp. due to its resistance to multiple antibiotics,^40^ as seen in this study.
If humans become infected with resistant Salmonella, it becomes difficult to treat such infections. This becomes a public health burden as it limits drug treatment options and may result in increased disease burdens.
This study was conducted at a single hospital in Zambia. This may limit the extrapolation of the findings to other larger regions or healthcare settings. This prompts additional studies with a larger study area and sample size to better understand the risk factors contributing to Salmonella spp. infections and antibiotic resistance in children <5 years. There may also have been some bias related to self-reporting and recall.
Conclusion
We observed a low prevalence of Salmonella infection in children <5 years at LMUTH. Out of the identified 20 isolates of Salmonella spp., only four isolates were susceptible to all the drugs used. Finally, the potential risk factors for acquiring Salmonella spp. identified in this study include the failure to treat or filter drinking water and guardians’ poor feeding habits with their children.
Supplementary Material
dlag031_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Graves NS . Acute gastroenteritis. Prim Care 2013; 40: 727–41. 10.1016/j.pop.2013.05.00623958366 PMC 7119329 · doi ↗ · pubmed ↗
- 2Eng SK, Pusparajah P, Ab Mutalib NS et al A review on pathogenesis, epidemiology and antibiotic resistance. Front Life Sci 2015; 8: 284–93. 10.1080/21553769.2015.1051243 · doi ↗
- 3Kayser FH, Bienz KA, Eckert J et al Medical Microbiology. Georg Thieme Verlag, 2005.
- 4Centers for Disease Control and Prevention . Salmonella Infection | CDC. 2021. https://www.cdc.gov/salmonella/index.html.
- 5Bosomprah S, Beach LB, Beres LK et al Findings from a comprehensive diarrhoea prevention and treatment programme in Lusaka, Zambia. BMC Public Health 2016; 16: 475. 10.1186/s 12889-016-3089-727268226 PMC 4895989 · doi ↗ · pubmed ↗
- 6Joseph A, Odimayo M, Oluwayemi IO et al An overview of the aetiologic agents of diarrhoea diseases in children: how far have we gone in management and control? MJZ 2017; 44: 266–75. 10.55320/mjz.44.4.298 · doi ↗
- 7Kapaya F, Dien Mwansa F, Sakubita P et al A foodborne disease outbreak investigation experience in a college in Lusaka, Zambia, 2017. African Med J 2018; 29: 1–9. 10.11604/pamj.2018.29.100.14737 · doi ↗
- 8Nazir J, Manzoor T, Saleem A et al Combatting Salmonella: a focus on antimicrobial resistance and the need for effective vaccination. BMC Infect Dis 2025; 25: 84. 10.1186/s 12879-025-10478-539833704 PMC 11744889 · doi ↗ · pubmed ↗