Unusual Case of Extensor Indicis Attachment: Cadaveric Observation and Clinical Relevance
Donovan B Turpin, Garrett T Folds, Caleb T Lee, Alexandra G Nolen, Andrew M Schwartz, Adegbenro Fakoya, Hosne Ara

TL;DR
This paper reports a rare anatomical variation in the extensor indicis muscle found during dissection and discusses its potential impact on medical treatment.
Contribution
The paper presents a previously undocumented anatomical variation of the extensor indicis brevis muscle.
Findings
An unusual attachment of the extensor indicis brevis muscle was identified during dissection.
The variation had an irregular origin and insertion, which could affect surgical procedures.
Abstract
Variations in anatomical structure present challenges to patients as well as medical professionals. In reference to patients, it could affect their lifestyle in terms of function. As for the medical professionals, treatments such as surgery could be made more difficult. Knowing the rare variations leads to better medical care and patient satisfaction and prevents unexpected complications. We discuss the extensor indicis (EI) muscle and the extensor indicis brevis (EIB), an anatomical variation we found while dissecting. The EIB had an irregular origin and insertion. We will further discuss and explore the implications of the variation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
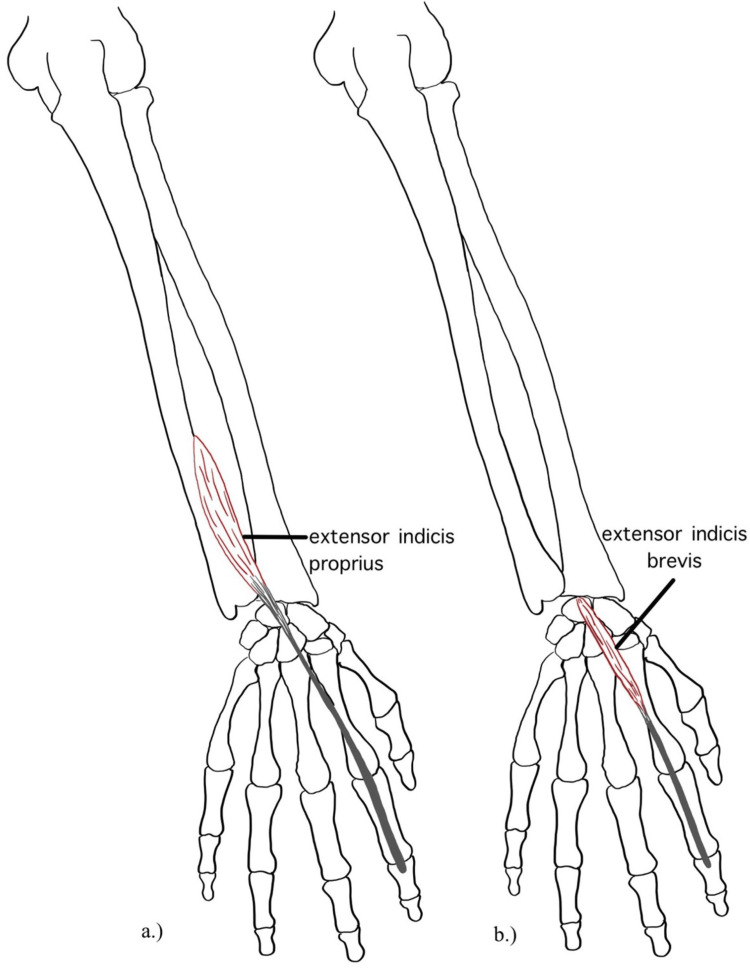 Figure 1
Figure 1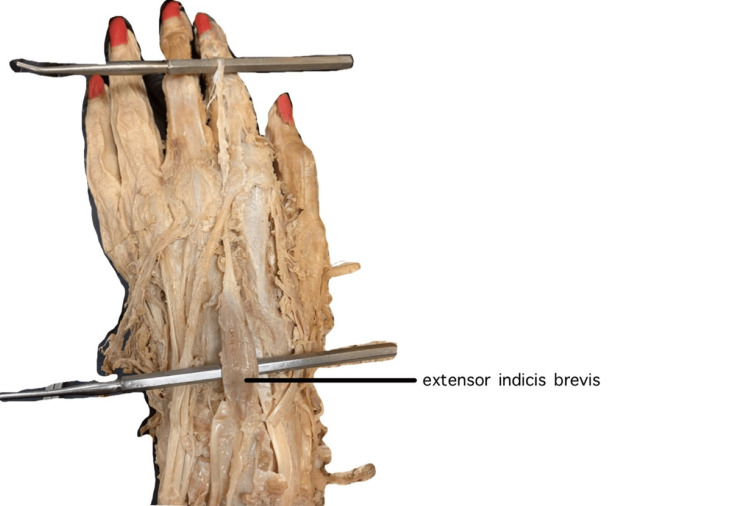 Figure 2
Figure 2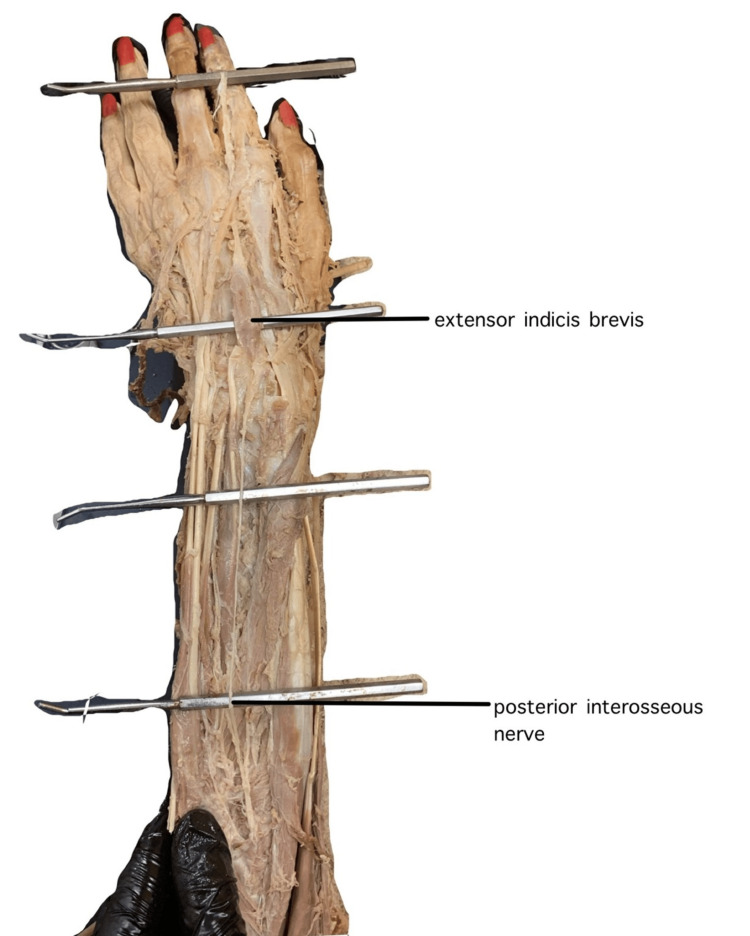 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Nerve Disorders · Myofascial pain diagnosis and treatment · Shoulder Injury and Treatment
Introduction
The extensor indicis (EI) is a slender, elongated muscle of the posterior compartment of the forearm that plays a crucial role in extension of the second digit. It is present in most individuals, with cadaveric studies estimating its prevalence at 96.5% [1]. Usually, it originates from the proximal two-thirds of the distal half of the interosseous line of the ulna, the adjacent interosseous membrane, or from fibrous septa associated with the extensor pollicis longus and the dorsal ulnar septum. The muscle fibers of the EI converge to form a tendon that courses distally through the fourth extensor compartment of the wrist, deep to the radial tendons of the extensor digitorum communis (EDC). The tendon crosses the wrist and inserts into the extensor expansion of the index finger, ulnar to the corresponding common extensor tendon [2]. The EI is innervated by the posterior interosseous nerve, a branch of the radial nerve (roots C7-C8), and functions to extend the index finger while assisting in wrist extension [3].
Anatomical variations of the EI have been extensively documented. In reference to its atypical variants, the normal EI is referred to as extensor indicis proprius (EIP). A varied EI can have multiple tendon heads, including variants with two slips (7.2%) and three slips (0.3%) [1]. In some cases, the EI tendon splits and connects to both the index finger and other digits, such as the thumb (0.75%), middle (1.6%), and ring fingers [1,4]. The EI tendon can also insert directly into the middle finger (3.7%) instead of the index finger [1]. Variations of the EI muscle can be relatively small (3%) and can have abnormal origins [2].
One such abnormal variant of the EI is the extensor digitorum brevis manus (EDBM). It is described as a short extensor with an origin in the dorsal carpal region and insertion into the index or middle fingers [4]. EDBM has a prevalence of 4% and is bilateral in 26% of cases [1]. Bernhard Siegfried Albinus first reported this variant in 1758, and it has since been classified into three categories [5,6]. EDBM type I, which is also known as extensor indicis brevis (EIB), inserts into the index finger with no accessory EI tendon present (see Figure 1). EIB makes up 31% of EDBM cases [1,6,7]. EDBM type II (46% of EDBM cases) can be divided into three subtypes, each of which includes EDBM and accessory EI tendons inserting into the index finger [6]. EDBM type III inserts into the middle finger with or without an accessory EI and makes up 23% of EDBM cases [1,6].
In this report, we describe a rare case of bilateral EIB and examine possible clinical significance. The aim of this study is to present a rare case of EIB and to explore the anatomical variations and the clinical significance of the location of the EI muscle.
Case presentation
Medical students at Louisiana State University Health Sciences Center in Shreveport underwent routine cadaveric dissection of a 90-year-old white female, fixed in formalin. During the dissection of the posterior forearm, the students noticed the absence of the EIP bilaterally from its conventional setting in the posterior antebrachial compartment. However, upon further dissection at the dorsum of the hand, an EIB was found to be present bilaterally.
Upon further inspection, the EIB appeared to originate from radial carpal bones proximally in the wrist joint. In tracing the tendon toward the index finger, it passed deep to the larger EDC tendon, inserting ulnar to it in the extensor expansion. The tendon continued to run parallel to the EDC tendon even to the middle and distal phalanges (Figures 1-2).
a) Illustration of extensor indicis proprius. b) Illustration of extensor indicis brevis, an anatomical variation of extensor indicis.
Dorsal view of extensor indicis brevis originating from radial carpal bones and inserting into extensor hood, elevated by the probes.
The innervation is most likely the posterior interosseous nerve, the same as many muscles of the posterior antebrachial compartment. Upon tracing the nerve from where it pierces the supinator muscle, it was found to travel past the wrist joint to the origin of the EIB (Figure 3). The presumed blood supply would come from the radial artery via the basal metacarpal arch.
Dorsal view of extensor indicis brevis and the posterior interosseous nerve, both originating from radial carpal bones, elevated by the probes.
Discussion
Fortuitous discovery of an EIB in the setting of cadaveric dissection gives an opportunity to discuss its importance for surgical and clinical settings. Accurate diagnosis is important to prevent misidentification as a pathologic structure, such as a ganglion cyst or other soft tissue mass [1,8]. Misdiagnosis or failure to recognize these anatomical variants can lead to unnecessary interventions, delayed treatment, or missed opportunities for more effective therapeutic strategies [1].
EIB and other EDBM variations are exceedingly rare clinically, and most cases are likely asymptomatic. However, it is possible that EIB can alter grip strength and dexterity of the affected hand, which may also play a role in a physical therapist’s evaluation and planning during rehabilitation [9,10]. EIB may also be relevant in surgical procedures such as tendon transfers or reconstructive hand surgery, where knowledge of these variations could help avoid complications [9,11]. Moreover, EIB may potentially be implicated in peripheral nerve compression disorders, along with wrist pain from swelling or inflammation [12,13].
Limitations of the study include the lack of availability of certain demographics and other measures (i.e., ethnicity and muscle/tendon measurements).
Conclusions
The EIB variant observed in this study represents a rare bilateral anatomical variation, with notable absence of the traditional EIP. Although often asymptomatic, such variants may have clinical consequences, including potential misdiagnosis as soft tissue masses, contribution to dorsal wrist pain, or complications during tendon transfers and dorsal wrist surgeries. Awareness of this variation is important for clinicians to avoid diagnostic confusion and optimize surgical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The prevalence of the extensor indicis tendon and its variants: a systematic review and meta-analysis Surg Radiol Anat Yammine K 2472543720152509650110.1007/s 00276-014-1352-0 · doi ↗ · pubmed ↗
- 2The extensor indicis proprius muscle - a study of 263 consecutive specimans Q Bull Northwest Univ Med Sch Cauldwell EW Anson BJ Wright RR 267279171943 https://link.springer.com/article/10.1007/s 00276-014-1352-0
- 3Anatomy, shoulder and upper limb, hand muscles Stat Pearls Okwumabua E Sinkler MA Bordoni B Treasure Island, FL Stat Pearls Publishing 2023 https://pubmed.ncbi.nlm.nih.gov/30725914/30725914 · pubmed ↗
- 4Bergman's Comprehensive Encyclopedia of Human Anatomic Variation Tubbs RS Shoja MM Loukas M Hoboken, NJ John Wiley & Sons, Inc.2016 https://onlinelibrary.wiley.com/doi/book/10.1002/9781118430309
- 5De extensore digitorum brevis manus Acad Annot Albinus BS 282941758 https://scholar.google.com/scholar?hl=en&as_sdt=0%2C 5&q=Albinus+BS%3A+De+extensore+digitorum+brevis+manus.+Acad+Annot.+1758&btn G=
- 6Anatomic and clinical studies of the extensor digitorum brevis manus J Hand Surg Ogura T Inoue H Tanabe G 10010712198710.1016/s 0363-5023(87)80171-53805622 · doi ↗ · pubmed ↗
- 7Extensor indicis brevis muscle: an unusual muscular variant Int J Morphol Garbelotti Junior S Yukio Fukuda T Rodrigues Pereira V Garcia Lucareli P Olave E 10711073302012
- 8Extensor digitorum brevis manus: an unusual cause of exercise-induced wrist pain Am J Sports Med Kuschner SH Gellman H Bindiger A 440441171989272949710.1177/036354658901700321 · doi ↗ · pubmed ↗