Oral Health and Social Isolation After 6 Years: Mediation of Oral Functions
Hazem Abbas, Kenji Takeuchi, Taro Kusama, Sakura Kiuchi, Ken Osaka

TL;DR
Poor oral health, like tooth loss and difficulty chewing, may lead to social isolation in older adults over six years.
Contribution
This study identifies potential mediating effects of oral functions on the link between oral health and social isolation in older adults.
Findings
Limited oral functions like speaking, smiling, and chewing partially mediated the association between tooth loss and social isolation.
The mediation effect was observed in participants with 10–19 teeth, but not in those with fewer teeth.
Dental prosthesis use had a minor impact on the mediation effect of oral functions.
Abstract
Tooth loss was longitudinally associated with social isolation. The absence of dental prosthesis use was an additional risk factor. However, the mediating pathways for this association are unknown. The aim of this cohort study was to estimate the mediating effect of three oral functions: speaking, smiling and chewing observed at baseline on the association between oral health at baseline and social isolation after 6 years of follow‐up. The 2010–2016 panel data from 6103 functionally independent participants aged ≥ 65 years who were not socially isolated at baseline was used from the Japan Gerontological Evaluation Study (JAGES). Causal mediation analysis using parametric logistic regression models was used to calculate the natural direct effect (NDE), the natural indirect effect (NIE), and the total effect. Social isolation was derived from a 5‐point index and dichotomised (0/3 = not…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
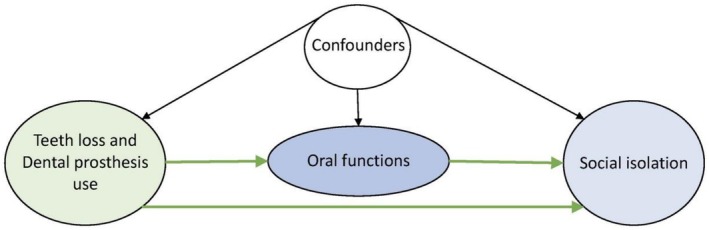 FIGURE 1
FIGURE 1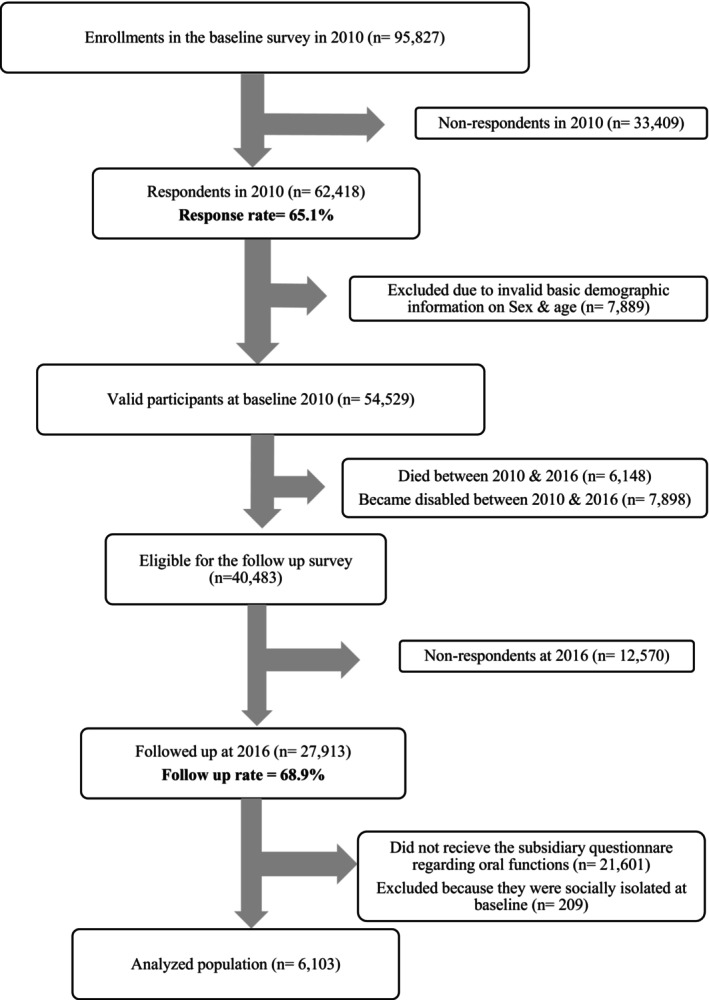 FIGURE 2
FIGURE 2| Total | ≥ 20 teeth | 10–19 teeth with dental prosthesis | 10–19 teeth without dental prosthesis | 0–9 teeth with dental prosthesis | 0–9 teeth without dental prosthesis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | |
|
| ||||||||||||
| No | 5756 | 94.3 | 2425 | 42.1 | 977 | 17.0 | 577 | 10.0 | 1276 | 22.2 | 501 | 8.7 |
| Yes | 347 | 5.7 | 30 | 8.6 | 73 | 21.0 | 19 | 5.5 | 156 | 44.9 | 70 | 20.0 |
|
| ||||||||||||
| No | 5743 | 94.1 | 2413 | 42.0 | 976 | 17.0 | 565 | 9.8 | 1286 | 22.4 | 504 | 8.8 |
| Yes | 360 | 5.9 | 42 | 11.6 | 74 | 20.5 | 32 | 8.8 | 146 | 40.5 | 67 | 18.5 |
|
| ||||||||||||
| No | 5692 | 93.3 | 2434 | 42.8 | 992 | 17.4 | 566 | 9.9 | 1245 | 21.9 | 456 | 8.0 |
| Yes | 411 | 6.7 | 21 | 5.2 | 58 | 14.0 | 31 | 7.5 | 187 | 45.4 | 115 | 28.0 |
|
| ||||||||||||
| 65–69 years | 2115 | 34.7 | 1014 | 47.9 | 395 | 18.7 | 210 | 9.9 | 370 | 17.5 | 127 | 6.0 |
| 70–74 years | 2104 | 34.5 | 881 | 41.9 | 368 | 17.5 | 211 | 10.0 | 466 | 22.1 | 178 | 8.5 |
| 75–79 years | 1249 | 20.5 | 417 | 33.4 | 189 | 15.1 | 131 | 10.5 | 343 | 27.4 | 170 | 13.6 |
| 80–84 years | 510 | 8.4 | 125 | 24.4 | 86 | 16.8 | 36 | 7.1 | 188 | 36.9 | 76 | 14.9 |
| ≥ 85 years | 125 | 2.0 | 19 | 15.2 | 12 | 9.9 | 8 | 6.5 | 65 | 52.1 | 20 | 16.2 |
|
| ||||||||||||
| Male | 2727 | 44.7 | 1112 | 40.8 | 494 | 18.1 | 252 | 9.3 | 624 | 22.9 | 245 | 9.0 |
| Female | 3376 | 55.3 | 1343 | 39.8 | 556 | 16.5 | 344 | 10.2 | 807 | 23.9 | 326 | 9.7 |
|
| ||||||||||||
| ≥ 13 years | 1126 | 18.4 | 573 | 50.9 | 212 | 18.8 | 76 | 6.8 | 212 | 18.8 | 53 | 4.7 |
| 10–12 years | 2251 | 36.9 | 962 | 42.7 | 420 | 18.7 | 226 | 10.0 | 500 | 22.2 | 144 | 6.4 |
| ≤ 9 years | 2726 | 44.7 | 921 | 33.8 | 418 | 15.3 | 294 | 10.8 | 720 | 26.4 | 374 | 13.7 |
|
| ||||||||||||
| < 20 000 USD/Year | 2848 | 46.7 | 1002 | 35.2 | 440 | 15.4 | 309 | 10.8 | 729 | 25.6 | 368 | 12.9 |
| 20 000–39 999 USD/Year | 2568 | 42.1 | 1111 | 43.2 | 483 | 18.8 | 243 | 9.5 | 565 | 22.0 | 167 | 6.5 |
| > 40 000 USD/Year | 687 | 11.2 | 342 | 49.9 | 127 | 18.5 | 44 | 6.5 | 137 | 20.0 | 36 | 5.2 |
|
| ||||||||||||
| IADL score 0–12 (dependent) | 3036 | 49.7 | 1141 | 37.6 | 493 | 16.2 | 322 | 10.6 | 750 | 24.7 | 330 | 10.9 |
| IADL score 13 (independent) | 3067 | 50.3 | 1314 | 42.8 | 557 | 18.2 | 274 | 8.9 | 681 | 22.2 | 241 | 7.8 |
|
| ||||||||||||
| Urban | 1211 | 19.8 | 570 | 47.1 | 212 | 17.5 | 114 | 9.4 | 248 | 20.5 | 66 | 5.5 |
| Sub‐urban | 2424 | 39.7 | 1030 | 42.5 | 426 | 17.6 | 224 | 9.2 | 550 | 22.7 | 195 | 8.0 |
| Rural | 2468 | 40.4 | 856 | 34.7 | 411 | 16.7 | 258 | 10.4 | 633 | 25.7 | 310 | 12.6 |
|
| ||||||||||||
| No (0–4) | 4699 | 77.0 | 1968 | 41.9 | 822 | 17.5 | 445 | 9.5 | 1056 | 22.5 | 407 | 8.7 |
| Yes (≥ 5) | 1404 | 23.0 | 487 | 34.7 | 227 | 16.2 | 151 | 10.8 | 375 | 26.7 | 164 | 11.7 |
|
| 6103 | 100.0 | 2455 | 40.2 | 1050 | 17.2 | 596 | 9.8 | 1431 | 23.5 | 571 | 9.4 |
| Total | Not isolated | Isolated | ||||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
|
| ||||||
| ≥ 20 teeth | 2455 | 40.2 | 2384 | 97.1 | 71 | 2.9 |
| 10–19 teeth with dental prosthesis | 1050 | 17.2 | 1016 | 96.8 | 34 | 3.2 |
| 10–19 teeth without dental prosthesis | 596 | 9.8 | 575 | 96.5 | 21 | 3.5 |
| 0–9 teeth with dental prosthesis | 1431 | 23.5 | 1378 | 96.3 | 54 | 3.7 |
| 0–9 teeth without dental prosthesis | 571 | 9.4 | 530 | 92.8 | 41 | 7.2 |
|
| ||||||
| No | 5756 | 94.3 | 5550 | 96.4 | 206 | 3.6 |
| Yes | 347 | 5.7 | 333 | 95.9 | 14 | 4.1 |
|
| ||||||
| No | 5743 | 94.1 | 5539 | 96.5 | 204 | 3.5 |
| Yes | 360 | 5.9 | 344 | 95.5 | 16 | 4.5 |
|
| ||||||
| No | 5692 | 93.3 | 5502 | 96.7 | 190 | 3.3 |
| Yes | 411 | 6.7 | 381 | 92.7 | 30 | 7.3 |
|
| ||||||
| 65–69 years | 2115 | 34.7 | 2054 | 97.1 | 61 | 2.9 |
| 70–74 years | 2104 | 34.5 | 2037 | 96.8 | 67 | 3.2 |
| 75–79 years | 1249 | 20.5 | 1192 | 95.4 | 57 | 4.6 |
| 80–84 years | 510 | 8.4 | 484 | 94.8 | 26 | 5.2 |
| ≥ 85 years | 125 | 2.0 | 117 | 93.4 | 8 | 6.6 |
|
| ||||||
| Male | 2727 | 44.7 | 2599 | 95.3 | 128 | 4.7 |
| Female | 3376 | 55.3 | 3284 | 97.3 | 92 | 2.7 |
|
| ||||||
| ≥ 13 years | 1126 | 18.4 | 1093 | 97.1 | 33 | 2.9 |
| 10–12 years | 2251 | 36.9 | 2173 | 96.5 | 78 | 3.5 |
| ≤ 9 years | 2726 | 44.7 | 2617 | 96 | 110 | 4 |
|
| ||||||
| < 20 000 USD/Year | 2848 | 46.7 | 2715 | 95.3 | 133 | 4.7 |
| 20 000–39 999 USD/Year | 2568 | 42.1 | 2492 | 97 | 77 | 3 |
| > 40 000 USD/Year | 687 | 11.2 | 677 | 98.6 | 10 | 1.4 |
|
| ||||||
| IADL score 0–12 (dependent) | 3036 | 49.7 | 2860 | 94.2 | 176 | 5.8 |
| IADL score 13 (independent) | 3067 | 50.3 | 3023 | 98.6 | 44 | 1.4 |
|
| ||||||
| Urban | 1211 | 19.8 | 1149 | 94.9 | 62 | 5.1 |
| Sub‐urban | 2424 | 39.7 | 2348 | 96.9 | 76 | 3.1 |
| Rural | 2468 | 40.4 | 2387 | 96.7 | 81 | 3.3 |
|
| ||||||
| No (0–4) | 4699 | 77.0 | 4571 | 97.3 | 127 | 2.7 |
| Yes (≥ 5) | 1404 | 23.0 | 1312 | 93.4 | 93 | 6.6 |
|
| 6103 | 100.0 | 5883 | 96.4 | 220 | 3.6 |
| Number of remaining teeth (ref. ≥ 20) | Mediators | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Difficulty in speaking | Problems in smiling | Difficulty in chewing | |||||||
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | ||||
|
| |||||||||
| Natural direct effect | 1.09 | 0.56 | 1.61 | 1.10 | 0.56 | 1.65 | 1.04 | 0.51 | 1.57 |
| Natural indirect effect | 1.02 | 0.93 | 1.11 | 1.02 | 0.93 | 1.10 | 1.04 | 0.94 | 1.14 |
| Total effect | 1.11 | 0.59 | 1.63 | 1.12 | 0.59 | 1.65 | 1.08 | 0.56 | 1.61 |
| Proportion mediated | 19.5% | 18.0% | 51.0% | ||||||
|
| |||||||||
| Natural direct effect | 1.13 | 0.33 | 1.94 | 1.13 | 0.34 | 1.93 | 1.12 | 0.34 | 1.90 |
| Natural indirect effect | 1.02 | 0.94 | 1.10 | 1.02 | 0.93 | 1.11 | 1.02 | 0.93 | 1.11 |
| Total effect | 1.15 | 0.34 | 1.96 | 1.16 | 0.35 | 1.96 | 1.15 | 0.35 | 1.94 |
| Proportion mediated | 14.8% | 14.8% | 15.7% | ||||||
|
| |||||||||
| Natural direct effect | 1.18 | 0.70 | 1.67 | 1.16 | 0.69 | 1.63 | 1.17 | 0.68 | 1.66 |
| Natural indirect effect | 0.99 | 0.91 | 1.07 | 1.00 | 0.93 | 1.07 | 1.00 | 0.91 | 1.09 |
| Total effect | 1.17 | 0.70 | 1.64 | 1.16 | 0.69 | 1.62 | 1.17 | 0.70 | 1.64 |
| Proportion mediated | — | — | — | ||||||
|
| |||||||||
| Natural direct effect | 2.41 | 1.36 | 3.46 | 2.19 | 1.16 | 3.21 | 2.49 | 1.57 | 3.41 |
| Natural indirect effect | 0.94 | 0.87 | 1.01 | 1.01 | 0.90 | 1.12 | 0.94 | 0.83 | 1.06 |
| Total effect | 2.27 | 1.31 | 3.23 | 2.20 | 1.26 | 3.14 | 2.34 | 1.45 | 3.24 |
| Proportion mediated | — | 1.8% | — | ||||||
- —Futoku‐kai foundation
- —Lion Corporation Ltd
- —Japan Society for the Promotion of Science10.13039/501100001691
- —Research Institute of Science and Technology for Society10.13039/501100009028
- —the Japan Science and Technology (JST)
- —Japan Health Promotion and Fitness Foundation10.13039/100019434
- —National Research Institute for Earth Science and Disaster Resilience
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Health disparities and outcomes · Food Security and Health in Diverse Populations
Introduction
1
Social isolation is a pressing global health concern due to its severe negative effects on physical and mental well‐being [1, 2]. Previous studies have linked social isolation to increased all‐cause mortality and other adverse health outcomes, including cognitive decline, depression, dementia, higher risk of rehospitalisation, decreased resistance to infections, and a greater likelihood of falls among older adults [1, 3, 4, 5]. These health impacts are particularly pronounced in aging societies such as Japan and Korea [6, 7]. Given the projected increase in the global population aged 65 years or older to 1.5 billion by 2050 (16% of the world's population), social isolation is expected to become a significant global health burden [8]. Recently, the World Health Organization (WHO) commission on social connection recommended community and individual‐level strategies to tackle social isolation and loneliness [2]. The commission advocates for integrating social connection strategies into policies, urban planning, and health systems, while also investing in research and public awareness to address the issue [2].
A decline in oral health status was associated with social isolation among the older population in the Japanese, English, and Brazilian contexts [9, 10, 11]. A previous longitudinal study from Japan using the same waves of the dataset used for this study showed that a fewer number of remaining teeth was associated with social isolation after 6 years of follow‐up, and no dental prosthesis use was an additional risk factor [9]. However, to date, the mechanism for this association was unknown. Previous studies suggested that tooth loss and not using dental prosthesis have a negative effect on conversational ability (speaking) [12], self‐esteem, and facial attractiveness (smiling with confidence) [13, 14], and subsequently, it might contribute to withdrawal from the surrounding society and eventually lead to social isolation [9, 10]. Additionally, tooth loss compromises chewing abilities, influences food intake [15], and quality of nutrients [16] leading to malnutrition, which was associated with underweight and frailty, a precursor for social isolation among the older population [9, 10, 17, 18].
The aim of this study was to examine the effect of three oral functions (speaking, smiling, and chewing) observed at baseline as mediators between oral health status represented by the number of teeth and dental prosthesis use at baseline and social isolation at follow‐up in an older Japanese population.
Methods
2
In this cohort study, the 2010–2016 panel data collected through a postal survey from the Japan Gerontological Evaluation Study (JAGES) was used. The JAGES is an ongoing study targeting functionally independent community‐dwelling adults aged 65 years or older to study their social, behavioural, and health‐related factors. Between 2010 and 2016, a combination of simple random sampling and complete survey for all 65 years or older residents was conducted alternatively in 13 municipalities across Japan [19]. The JAGES has a core questionnaire distributed to all eligible targeted participants and a set of subsidiary questionnaires distributed randomly to one in four of the eligible targeted participants. The questions related to the deterioration of the three oral functions used as mediators in this study were part of the subsidiary questionnaire. The inclusion criteria for this study were answering the subsidiary questionnaire, being functionally independent, and not socially isolated at baseline to have an outcome‐free cohort.
Exposure Variables (Independent Variables)
2.1
Based on previous studies, self‐reported number of remaining teeth and dental prosthesis use at baseline represented oral health status [9, 10]. The question “How many natural teeth do you have in your mouth?” was used to identify the number of remaining teeth. Its four responses were “20 or more teeth”, “10–19 teeth”, “1–9 teeth” and “no natural teeth”. However, the last two categories were combined into the “0–9 teeth” category due to the small proportions of these participants. While the question “Do you wear dentures or bridges (non‐removable dentures)?” was used to determine dental prosthesis use. Its four responses were “No”, “Yes, in the upper jaw”, “Yes, in the lower jaw” and “Yes, in both jaws”. These answers were dichotomised into (dental prothesis use vs no dental prosthesis use). Then, based on previous studies, these two variables were combined to derive the main exposure variable with its five categories: “≥ 20 natural teeth”, “10–19 natural with dental prosthesis”, “10–19 natural teeth without dental prosthesis”, “0–9 natural teeth with dental prosthesis” and “0–9 natural teeth without dental prosthesis” [9, 10]. In the sensitivity analyses, number of remaining teeth and dental prosthesis use were used as two separate exposures in separate analytical models. Self‐reported number of teeth of the older adults in Japan was previously validated [20, 21].
Outcome Variable (Dependent Variable)
2.2
Social isolation is an objective multidimensional concept that encompasses withdrawal from the surrounding society in the form of lack of social contacts and interactions with family members, friends, and the surrounding community [22, 23, 24]. However, there is no consensus on a clear definition of social isolation [25]. In this study, an objective comprehensive multidimensional variable was used to measure social isolation [9, 26, 27]. A 5‐point index was derived from the binary responses to the following five domains of questions collected at follow‐up in 2016: (1) being married or cohabitating with a partner; (2) living with one's own children or grandchildren or having someone to provide emotional or instrumental social support; (3) having immediate family members or relatives who could provide emotional or instrumental social support; (4) having face‐to‐face contact with friends more than once a month or having friends who could provide emotional or instrumental social support; and (5) participation in any volunteer group, leisure activity group, senior citizen club, neighbourhood or residents' association, and industrial or trade association [24, 27]. A score of zero indicated no social isolation, and a score of five indicated severe social isolation. Based on previous studies and using a data‐driven approach, a binary variable was derived from this 5‐categorical variable as follows: Scores 0 to 3 were not socially isolated, and scores 4 and 5 were socially isolated [9, 10]. The predictive and convergent validities of the social isolation index have been confirmed in previous studies [10, 28, 29].
Mediators
2.3
The deteriorations in three oral functions observed at baseline were used as hypothesised mediators for the association between oral health status and social isolation. They were having difficulty in speaking, having problems in smiling, and having difficulty in chewing.
Two questions derived from the short version of the Oral Impacts on Daily Performance (OIDP) questions in the JAGES subsidiary questionnaire were used. Participants were asked, “Have you had any problems related to your teeth, gums, and/or dentures during the past 6 months?” and were able to choose a binary answer (yes/no) regarding the following two items: “Difficulty in speaking clearly” and “Hesitated to show teeth when laughing or talking”. While for having difficulty in chewing, the following question regarding subjective chewing ability was used: “How well can you eat hard food?” and its five categorical answers were “I can chew and eat anything I want.”, “I have trouble chewing some foods, but I can eat most foods.”, “I can't chew well, and can only eat limited foods.”, “I can hardly chew at all.” and “I cannot chew at all, and I am on a liquid diet.” Those who chose one of the first two answers were categorised as not having difficulty in chewing, while those who chose one of the last three answers were categorised as having difficulty in chewing.
Confounders
2.4
A directed acyclic graph (DAGitty version 3.0) was used to structure the theoretical framework of this study (Figure 1). Based on previous studies and by following a conservative approach for selecting the confounders [9], the data collected at the baseline in 2010 for demographics, socioeconomic status (SES), health and lifestyle, and area of residence were included as confounders. Age and sex were included as demographic confounders. Educational attainment expressed by years of formal education and the equivalised household income (i.e., annual pretax household income/square root of the number of family members) were included as SES confounders [30]. The reported income in Japanese Yen (JPY) was converted to United States Dollar (USD) at the common average rate of (100 JPY = 1 USD) at the time of data collection in 2010. For health and lifestyle, the 13‐question version of instrumental activities of daily living (IADL) was used. One point of the score was assigned to each question. A score of zero indicated complete dependence on others for daily‐life activities, and a score of 13 indicates complete independence [31]. The IADL score was dichotomised into dependent (IADL score = 0–12) and independent (IADL score = 13). Area of residence was determined by calculating population density based on 2010 national census data and was categorised into three categories: urban (≥ 4000 people/km^2^), suburban (1000–3999 people/km^2^), and rural (0–999 people/km^2^) [32]. Having depressive symptoms was assessed using the geriatric depression scale (GDS‐15) and was included as a psychological confounder [33]. Using the cut‐off value (GDS score = 5) as suggested by previous studies, the GDS‐15 scores were dichotomised to indicate having depression symptoms [33, 34].
The hypothesised directed acyclic graph (DAG) for the mediation analysis of the association between the number of remaining teeth and dental prosthesis use with social isolation. Confounders were age, sex, educational attainment, equivalised income level, independent ability of daily living, area of residence and depressive symptoms. The three mediating oral functions were difficulty in speaking, problems in smiling and difficulty in chewing.
Statistical Analysis
2.5
Descriptive analyses examined the baseline characteristics of the sample as well as the cumulative incidence rate of social isolation at follow‐up. Causal mediation analysis using paramed command with logistic regression was used to calculate the odds ratios (ORs) and 95% confidence intervals (95% CIs) of the natural direct effect (NDE), the natural indirect effect (NIE), and the total effect (TE) for the deterioration of the three oral functions on the association between oral health and social isolation [35]. The proportion mediated (PM) was also calculated as it indicated the proportion of TE through a given mediator. Causal mediation analyses address biases in the classical and traditional methods (product or difference methods) by using the counterfactual framework allowing for exposure–mediator interaction through calculating the direct and indirect effects [35]. Paramed command in Stata accommodates binary variables. The exposure was a five‐categorical variable; consequently, four datasets were created to allow for analysis of each oral health category in comparison to the reference (≥ 20 teeth); thus, the analyses were conducted four times for each mediator. In addition, dummy variables for the confounders were created. Multiple imputation method with chained equations was used to address potential biases due to missing data in the panel dataset.
For sensitivity analyses, first, the two variables representing oral health (number of teeth and dental prosthesis use) were used as two separate exposures in supplementary causal mediation analyses. Second, to assess the effect of the unmeasured confounders, the E‐values were calculated. The E‐value represents the minimum strength of association that an unmeasured confounder would need to have with both the exposure and outcome to explain away the observed association conditional on the measured confounders [36]. Third, logistic regression was used to calculate the odds ratio for the incidence of social isolation at follow‐up using a combined variable for the number of remaining teeth and dental prosthesis use in two regression models, a crude model and a fully adjusted model. Fourth, the interaction and effect modification between dental prosthesis use and the number of remaining teeth on social isolation were also examined. Fifth, the relationship between oral health and social isolation was examined using the inverse probability of treatment weighting (IPTW) method with multinomial regression to reduce bias resulting from the heterogeneity in the distribution of measured confounders among the participants by creating a pseudo‐population where the treatment assignment was independent of the observed confounders through applying weights based on the inverse of the propensity score. Sixth, the descriptive and the logistic regression data analyses using the complete data without multiple imputation were reported in the Tables S1–S9. Stata/SE 16 software from StataCorp LP (College Station, Texas, USA) was used for statistical analyses, and the STROBE guidelines for cohort studies were followed. No content of this study was created using Artificial Intelligence (AI).
Ethics Statement
2.6
Ethical approval for the JAGES project 2010 was obtained from the Ethics Committee of Nihon Fukushi University (approval number: 10‐05). Ethical approval for the study of the JAGES project 2016 was obtained from the Ethics Committee of the National Center for Geriatrics and Gerontology (approval number: 992) and Chiba University (approval number: 2493). Participants were notified that participation was voluntary, and returning an answered survey was considered a consent to participation.
Results
3
Figure 2 shows the flow chart of the study participants. The total number of participants who replied to both waves of the postal survey was 27 913 participants, with a follow‐up rate of 68.9%. In total, 6103 participants were eligible as study participants according to the inclusion criteria. Table 1 shows the baseline characteristics of the participants according to their oral health. The mean age of the study participants was 72.4 years (SD = ±5.1), and 44.7% were males. Social isolation was observed at follow‐up in 3.6% of participants (n = 220). While Table 2 showed the breakdown of the cumulative incidence rate of social isolation status at the follow‐up as follows: 71 participants (2.9%) had ≥ 20 teeth (with or without using dental prosthesis), 34 (3.2%) had 10–19 teeth and used dental prosthesis, 21 (3.5%) had 10–19 teeth and did not use the dental prosthesis, 54 (3.7%) had 0–9 teeth and used dental prosthesis, and 41 participants (7.2%) had 0–9 teeth and did not use the dental prosthesis. The cumulative incidence of social isolation was higher among those who had difficulty in speaking, problems in smiling, and difficulty in chewing. Those with fewer teeth and no dental prosthesis use, males, older age groups, less educated, lower income groups, dependent on others for their daily life activities, living in urban areas, and those who had depressive symptoms showed higher cumulative incidence rates of being socially isolated at follow‐up. Tables S1 and S2 showed the baseline characteristics of the study participants and the proportions of social isolation at follow‐up before multiple imputation. The findings of ST1 and ST2 showed similar pattern direction and magnitude compared with the main analyses.
Flow chart of the participants from baseline in 2010 to follow‐up in 2016.
Table 3 shows the findings of the causal mediation analyses. Considering the observed wide (95% CIs) of most of the NDE and TE, the findings did not reject the null hypothesis; however, the TE of oral health status on social isolation tended to be higher among those with worse oral health status in all mediation models of the three oral functions. In addition, compared with those with 20 or more teeth, having difficulty in speaking (NIE OR = 1.02, 95% CI = 0.93–1.11), problems in smiling (NIE OR = 1.02, 95% CI = 0.93–1.10), and difficulty in chewing (NIE OR = 1.04, 95% CI = 0.94–1.14) might have mediated the association between tooth loss at baseline and social isolation at follow‐up for those with 10–19 teeth and used dental prosthesis as well as for those with 10–19 teeth without dental prosthesis (NIE OR = 1.02, 95% CI = 0.94–1.10), (NIE OR = 1.02, 95% CI = 0.93–1.11), and (NIE OR = 1.02, 95% CI = 0.93–1.11), respectively. While they might not have mediated the association for those with 0–9 teeth with and without dental prosthesis, the proportion mediated through having difficulty in chewing was higher than the other two oral functions among those having 10–19 teeth with and without dental prosthesis. Overall, these three mediators explained 18%–51% of the relationship between oral health and social isolation for those with 10–19 teeth and used dental prosthesis, while this proportion was 14.8%–15.7% for those with 10–19 teeth and did not use dental prosthesis.
In the sensitivity analyses, a similar pattern, direction, and magnitude of the mediation findings were observed. Table S3 shows the mediating effect of oral functions decline when only the number of teeth was used as an exposure. Oral functions might have mediated the association for those with 10–19 teeth but might not have for those with 0–9 teeth. While Table S4 showed the findings when only dental prosthesis use was used as an exposure, oral functions might not have mediated the association in this model. Table S5 shows the estimated E‐values. E‐values' estimates were relatively large and varied from 1.37 to 4.11 in odds ratio scales, suggesting robust estimates of this study even if there were unmeasured confounders. Tables S6 and S7 show the estimates of the association between oral health (using a combined variable for the number of remaining teeth and dental prosthesis use) and social isolation using logistic regression on both the imputed data and the complete case scenarios. A similar pattern, direction, and magnitude of the estimates were observed in both scenarios. Table S8 showed the interaction and effect modification between dental prosthesis use and the number of remaining teeth on social isolation. The findings were contrasting depending on the number of remaining teeth. Dental prosthesis use seemed to mitigate the odds of incidence of social isolation at follow‐up for those with 0–9 remaining teeth (i.e., synergistic effect) but not for those with 10–19 remaining teeth (i.e., antagonistic effect) using both the interaction additive and multiplicative scales. Table S9 showed the findings of the relationship between oral health and social isolation at follow‐up using IPTW. A pattern similar in direction but considerably smaller in magnitude compared to the findings of the logistic regression models was observed (i.e., in the adjusted model, the group having 0–9 teeth without dental prosthesis showed a considerably small (2%) likelihood to be socially isolated at follow‐up compared to the group with 20 or more teeth).
Discussion
4
To the best of our knowledge, this was the first study to investigate the mediation effect of three oral functions (speaking, smiling, and chewing) on the association between oral health and social isolation. Considering the low precise and high uncertain estimates, the findings did not reject the null hypothesis; however, having difficulty in speaking, problems in smiling, and difficulty in chewing might have mediated the association between oral health status and social isolation among those having 10–19 teeth with and without dental prosthesis but might not have among those having 0–9 teeth with and without dental prosthesis. The proportions mediated through having difficulty in chewing were higher than those of the other two oral functions among those having 10–19 teeth with and without dental prosthesis.
These findings were consistent with the hypothesised mechanisms explaining the association between oral health and social isolation in previous studies [9, 10]. Tooth loss and not using dental prosthesis had adverse effects on conversational ability (speaking) [12], self‐esteem, and facial attractiveness (smiling with confidence) [13, 14], and subsequently, it might contribute to withdrawal from the surrounding society and eventually lead to social isolation [9, 10]. In addition, compromised chewing abilities resulting from tooth loss influence food intake [15], and quality of nutrients [16] leading to malnutrition, which was associated with underweight and frailty, a precursor for social isolation among the older population [9, 10, 17, 18].
To explain the variation in the findings among oral health groups, those with 10–19 teeth with and without dental prosthesis use (moderate oral health deterioration group) tended to be younger, more educated, wealthier, more independent, and had fewer depressive symptoms. Thus, it's highly likely that their communication ability, facial appearance, and eating ability were of major importance, and the decline of these oral functions had a higher impact on them and led to their social isolation. On the contrary, those with 0–9 teeth with and without dental prosthesis use (severe oral health deterioration group) tended to be older, less educated, less wealthy, dependent on others for their daily activities, living in rural areas, and had more depressive symptoms. Thus, it's highly likely that their communication ability, facial appearance, and eating ability were of minor importance, and non‐oral health‐related mediators such as depression, social anxiety, chronic stress, reduced self‐esteem, and unhealthy diet had a higher impact on them and led to their social isolation status. According to previous studies, more tooth loss was associated with having more depressive symptoms [37] and reduced self‐esteem [13], and having depressive symptoms was associated with social isolation [38]. Thus, depression resulting from tooth loss, especially in the case of anterior teeth loss among other psychological factors, might mediate the association between oral health and social isolation, especially for those with severe tooth loss (0–9 teeth groups).
The findings of this study emphasised the importance of social functions of oral health as it showed that the decline in speaking and smiling as chief communication tools could be a pathway to future social isolation, a relatively less emphasised importance in the literature [9] compared to the already emphasised importance of the decline in eating abilities (in the form of compromised chewing ability) as the nutritional function of oral health [39]. Interventions aiming for retention of natural teeth and the provision of dental prosthesis might help reduce the oral health‐related burden on social isolation.
The findings of this study should be interpreted with caution considering its limitations. First, the wide confidence intervals observed suggested high uncertainty and low precision of the estimates. This could be attributed to the smaller sample size compared to the previous study (almost 1/5 of the sample of the previous study) as the mediators' questions were part of the subsidiary, not the core questionnaire of JAGES [9]. This calls for caution in interpreting the findings and potentially for further research with a larger sample size to help narrow the confidence interval and provide a more precise estimate of the effect. Second, despite the conservative approach to adjust for potential confounders, the possibility of the existence of unmeasured confounders could not be ruled out. However, E‐values were calculated to assess the magnitude of the unmeasured confounders, and their findings showed that the magnitude of unmeasured confounders was relatively small. Third, although the three included oral functions mediated between 14.8% and 51% of the association between oral health and social isolation, the role of other oral health‐related mediators, such as dental pain and discomfort, could not be estimated due to data limitations. Fourth, selection bias due to dropouts during the 6 years of follow‐up might have led to the underestimation of the findings. Those who dropped out as non‐respondents were 12 570 participants; other dropouts died or became disabled (Follow‐up rate = 68.9%). Dropouts are usually considered to have worse health and oral health statuses. Thus, if dropouts were included, the findings might have been larger.
Fifth, time‐varying confounding such as income fluctuations, changes in independence in activities of daily living (IADL), changes in living area, and having depressive symptoms over the 6 years of follow‐up may have influenced the findings. However, the income data showed similar income levels at follow‐up (mean 35 800, standard deviation 28 000 and median 27 500 USD/Year) compared to baseline (mean 39 600, standard deviation 28 100 and median 35 000 USD/Year), and the baseline equivalised income was adjusted in the analyses, in addition to the fact that the participants of this study were aged 65 years and older and their main source of income tended to be their pension; thus, income fluctuations within this age group are believed to be low in Japan [40, 41]. Similarly, the proportions of those living in urban, suburban, and rural areas as well as for those having versus not having depressive symptoms were similar at follow‐up compared to baseline. However, the changes in independence in activities of daily living (IADL) between baseline and follow‐up could not be assessed in a similar manner due to the absence of some IADL‐related questions in the follow‐up survey. Thus, the effect of time‐varying confounding in the analyses was assessed to be small. Sixth, the generalisability of the findings was limited because JAGES data is not nationally representative. On the other hand, the major strength of this study was that it was the first study to explain to some extent the mechanism of the relationship between oral health and social isolation. In addition, causal mediation analysis was used to estimate the magnitude of the mediated pathways through the three included oral functions, allowing for mediator‐exposure interaction. The findings of this study could be used as a foundation for future causal mediation studies that need to investigate remaining potential oral health‐related mediators (dental pain and discomfort) as well as the potential non‐oral health‐related mediators (depression, social anxiety, chronic stress, reduced self‐esteem and unhealthy diet) for the association between oral health and social isolation.
Conclusion
5
Considering the low precise and high uncertain estimates, the findings did not reject the null hypothesis; however, the mediation effect of oral functions varied by oral health status. Compared with those with 20 or more teeth, oral functions might have mediated the association between oral health and social isolation for those with 10–19 teeth with and without dental prosthesis, but might not have for those with 0–9 teeth with and without dental prosthesis. The proportion mediated through having difficulty in chewing was higher than the other two oral functions among those having 10–19 teeth with and without dental prosthesis. These findings suggested the presence of non‐oral health related mediators for the association between oral health and social isolation, especially among those with severe tooth loss (0–9 teeth groups). Further research exploring more mediating pathways using larger datasets to help narrow the confidence interval and provide more precise and significant estimates of the effect is required.
Author Contributions
Hazem Abbas contributed to the conception of the study, study design, project administration, data acquisition, data analysis, interpretation of the findings and drafted the manuscript; Kenji Takeuchi, Taro Kusama and Sakura Kiuchi contributed to the study design, data acquisition, data analysis and interpretation of the findings; Ken Osaka contributed to the data acquisition. All authors critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of the work, ensuring integrity and accuracy.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: Baseline characteristics of the participants by oral health status showing the missing data before multiple imputation (n = 6103). Table S2: The proportion of incidence of social isolation at follow up showing the missing data before multiple imputation (n = 6103). Table S3: The mediating effect of oral functions decline in the association between tooth loss and social isolation after multiple imputation (n = 6103). Table S4: The mediating effect of oral functions decline in the association between dental prosthesis use and social isolation after multiple imputation (n = 6103). Table S5: Robustness to unmeasured confounding (E‐values) for the total effect (TE) of the association between oral health and social isolation. Table S6: The association between oral health and social isolation at follow‐up after multiple imputation (n = 6103). Table S7: The association between oral health and social isolation at follow‐up using complete data analysis. Table S8: The interaction and effect modification between dental prosthesis use and number of remaining teeth on social isolation at follow‐up after multiple imputation (n = 6103). Table S9: The association between oral health and social isolation at follow‐up using inverse probability of treatment weighting (IPTW) after multiple imputation (n = 6103).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization , “Social Isolation and Loneliness Among Older People: Advocacy Brief,” (2021, accessed July 22, 2024), https://www.who.int/publications/i/item/9789240030749.
- 2World Health Organization , “WHO Commission on Social Connection,” (2025, accessed August 6, 2025), https://www.who.int/groups/commission‐on‐social‐connection.
- 3J. Holt‐Lunstad , T. B. Smith , M. Baker , T. Harris , and D. Stephenson , “Loneliness and Social Isolation as Risk Factors for Mortality: A Meta‐Analytic Review,” Perspectives on Psychological Science 10, no. 2 (2015): 227–237, 10.1177/1745691614568352.25910392 · doi ↗ · pubmed ↗
- 4R. Mistry , J. Rosansky , J. Mc Guire , C. Mc Dermott , and L. Jarvik , “Social Isolation Predicts Re‐Hospitalization in a Group of Older American Veterans Enrolled in the UPBEAT Program,” International Journal of Geriatric Psychiatry 16, no. 10 (2001): 950–959, 10.1002/gps.447.11607938 · doi ↗ · pubmed ↗
- 5K. A. Faulkner , J. A. Cauley , J. M. Zmuda , J. M. Griffin , and M. C. Nevitt , “Is Social Integration Associated With the Risk of Falling in Older Community‐Dwelling Women?,” Journals of Gerontology. Series A, Biological Sciences and Medical Sciences 58, no. 10 (2003): 954–959, 10.1093/gerona/58.10.m 954.14570865 · doi ↗ · pubmed ↗
- 6E. Klinenberg , “Social Isolation, Loneliness, and Living Alone: Identifying the Risks for Public Health,” American Journal of Public Health 106, no. 5 (2016): 786–787, 10.2105/AJPH.2016.303166.27049414 PMC 4985072 · doi ↗ · pubmed ↗
- 7E. Courtin and M. Knapp , “Social Isolation, Loneliness and Health in Old Age: A Scoping Review,” Health & Social Care in the Community 25, no. 3 (2017): 799–812, 10.1111/hsc.12311.26712585 · doi ↗ · pubmed ↗
- 8World Health Organization , “Global Health and Aging. Global Health and Aging,” (2011, accessed January 13, 2021), https://www.who.int/ageing/publications/global_health.pdf.