Immunocompetent but Not Immune: A Prolonged Course of Cryptococcal Meningitis
Carlos Fagundo, Abdul Rahman Omari, Mauricio Valenzuela

TL;DR
A healthy woman developed cryptococcal meningitis and had a prolonged recovery despite standard treatment, highlighting challenges in managing this condition in immunocompetent individuals.
Contribution
This case report presents a rare instance of prolonged culture positivity in an immunocompetent patient with cryptococcal meningitis.
Findings
The patient's cerebrospinal fluid cultures remained positive for over 6 weeks despite guideline-directed antifungal therapy.
Resolution of cryptococcal meningitis required aggressive intracranial pressure management and surgical intervention.
Prolonged antifungal therapy and VP shunt placement were critical for the patient's recovery.
Abstract
Cryptococcus neoformans is an encapsulated yeast that typically causes cryptococcal meningitis (CM) in immunocompromised hosts. However, CM can rarely occur in immunocompetent individuals, often with atypical or insidious presentations. Persistently positive cerebrospinal fluid (CSF) cultures despite guideline-directed antifungal therapy are uncommon and pose significant management challenges. In this case report, we describe a previously healthy 40-year-old immunocompetent woman who presented with seizures, progressive headaches, and elevated intracranial pressure (ICP). CSF studies confirmed CM with positive cryptococcal antigen and cultures. She was treated with liposomal amphotericin B and flucytosine and later transitioned to high-dose fluconazole due to medication intolerance. Despite >6 weeks of antifungal therapy, serial CSF cultures remained persistently positive through…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
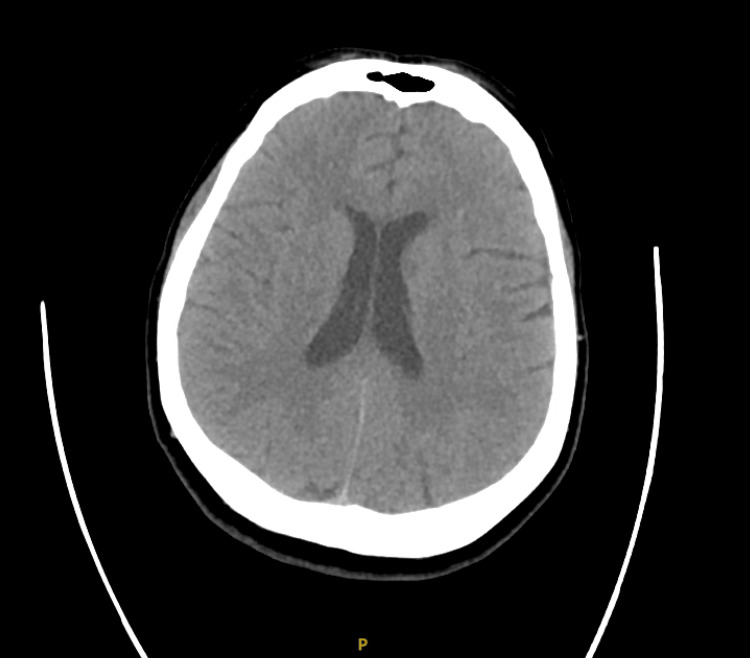 Figure 1
Figure 1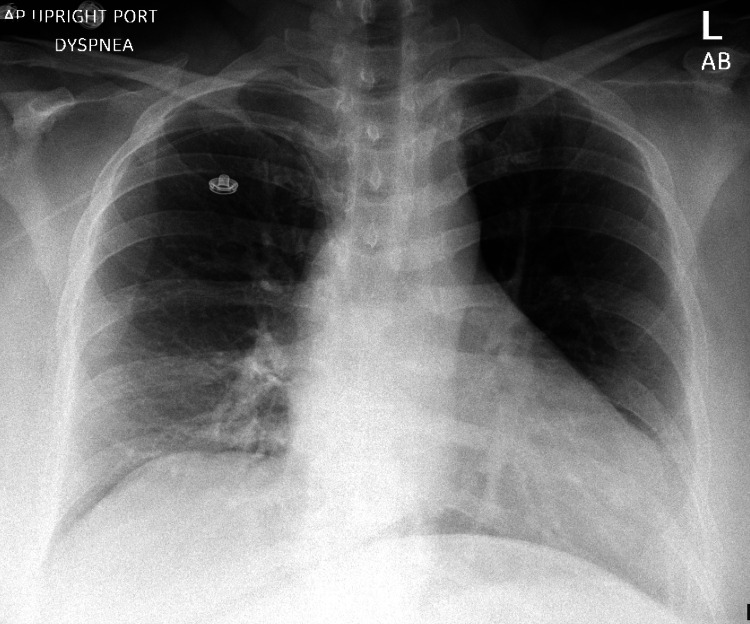 Figure 2
Figure 2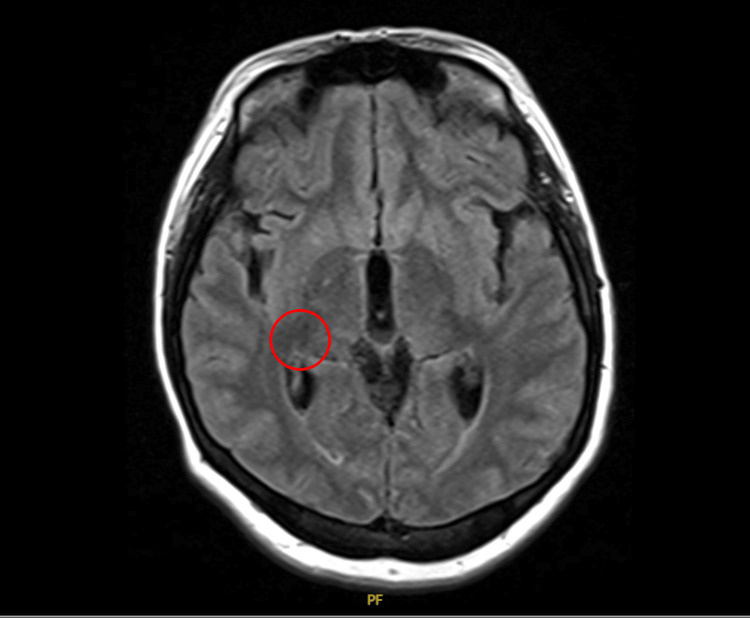 Figure 3
Figure 3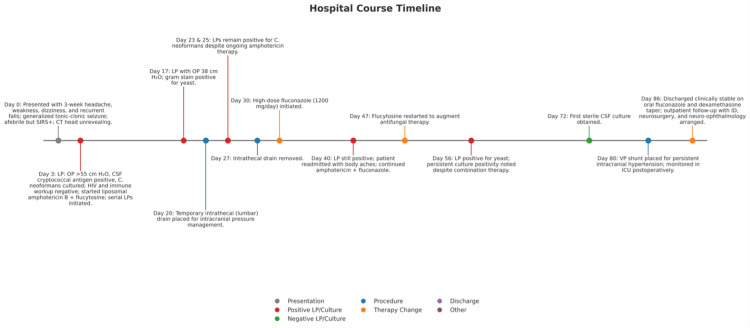 Figure 4
Figure 4| Parameter | Value | Reference range | Interpretation | Time |
| WBC | 17.2 × 10⁹/L | 4.0–10.5 × 10⁹/L | Increased (leukocytosis) | Admission |
| Sodium | 127 mmol/L | 135–145 mmol/L | Decreased (hyponatremia) | Admission |
| Serum cryptococcal Ag titer | 1:1280 | Negative | Positive | Admission |
| CSF WBC | 87 cells/µL | ≤5 cells/µL | Increased (lymphocytic) | Day 3 |
| CSF protein | 28 mg/dL | 15–45 mg/dL | Normal | Day 3 |
| CSF glucose | 50 mg/dL | 40–70 mg/dL | Normal | Day 3 |
| CSF opening pressure | >55 cm H₂O | <20 cm H₂O | Markedly elevated | Day 3 |
| CD4 count | 1258 cells/µL | 500–1500 cells/µL | Normal | Admission |
| CD4 % | 36% | 30–60% | Normal | Admission |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Infectious Diseases and Tuberculosis
Introduction
Cryptococcus neoformans is an encapsulated, opportunistic yeast that causes cryptococcosis, a potentially life‑threatening invasive fungal disease. The organism is found in soil contaminated with avian droppings and decaying wood and is acquired primarily through inhalation of desiccated yeast cells [1]. Following inhalation, C. neoformans can establish latent infection or disseminate hematogenously. It commonly invades the central nervous system (CNS), where it causes meningoencephalitis [1,2].
Cryptococcal meningitis (CM) most commonly occurs in patients with advanced HIV infection, solid‑organ transplantation, or other causes of severe cellular immunodeficiency [1,3]. Disease in immunocompetent hosts does occur and may present insidiously, leading to diagnostic delay and increased risk of neurologic morbidity [4,5]. Clinical manifestations include subacute headache, fever, altered mental status, and visual changes. Elevated intracranial pressures (ICPs) are associated with increased morbidity and mortality [1,6].
Current guidelines recommend induction therapy with amphotericin B plus flucytosine for at least four to six weeks, followed by consolidation and maintenance therapy with fluconazole, alongside aggressive ICP control when needed [1,2,6]. We present the case of an immunocompetent woman with CM and positive cerebrospinal fluid (CSF) cultures for over 70 days despite guideline‑directed antifungal therapy. The patient required a prolonged course of induction medication and ventriculoperitoneal (VP) shunting for definitive ICP control.
Case presentation
We present a previously healthy 40-year-old woman with obesity (BMI 36.7 kg/m²) and a history of bipolar disorder, anxiety, depression, post-traumatic stress disorder (PTSD), schizophrenia, hypertension, and tachycardia who presented to the emergency department with a three-week history of worsening headaches, generalized weakness, dizziness, and recurrent falls. The patient has no history of chronic corticosteroid use, immunosuppressive therapy, diabetes mellitus, or chronic liver disease. On the day of admission, she sustained a fall with minor head trauma but no loss of consciousness. In the emergency department, she developed a generalized tonic-clonic seizure that terminated after two doses of intravenous lorazepam (2 mg each).
On arrival, she was afebrile but met systemic inflammatory response syndrome (SIRS) criteria; she presented with an elevated white blood cell count and tachycardia (Table 1). Serum sodium was decreased (Table 1). Due to her initial presentation, a CT angiography of the head and neck was obtained, which was negative but limited by motion artifact (Figure 1). Chest X-ray was unremarkable (Figure 2). The patient was admitted for further evaluation. Neurology was consulted, who initiated lacosamide but later transitioned her to home divalproex sodium after electroencephalography showed no epileptiform activity.
Computed tomogrpahy (CT) without contrast of the head, transverse view. Normal brain formation. There is no hydrocephalus, acute intracranial mass, mass effect or midline shift. No intra-or extra-axial hemorrhage. No evidence of cytotoxic edema corresponding to a large vascular territory. No acute fracture.
Chest X-ray, anterior posterior view. No pneumothorax or sizable pleural effusions.
Due to the patient's prolonged headache and new-onset seizures, Interventional Radiology (IR) was consulted for an image-guided lumbar puncture (LP). The image-guided LP revealed significantly elevated opening pressure with clear CSF with increased white blood cells, normal protein, and glucose levels within CSF fluid (Table 1). CSF cryptococcal antigen was positive, and culture grew C. neoformans; the initial serum cryptococcal antigen was elevated. HIV testing, hepatitis C testing, and quantitative immunoglobulin levels were unremarkable (Table 1).
Liposomal amphotericin B and flucytosine were initiated, and serial therapeutic LPs were performed for ICP control. Ophthalmologic evaluation revealed papilledema and right-eye visual blurring. MRI of the brain demonstrated only small chronic microvascular changes without acute infarction, mass effect, or hydrocephalus (Figure 3).
Magnetic resonance image (MRI) of the head, transverse view. Small focus of hypodensity involving the right lentiform nucleus, circled in red, likely from chronic microvascular ischemic disease. No acute infarction. The brain parenchyma appears normal otherwise. No hemorrhage, mass, abnormal fluid collections, midline shift, cerebral infarction, or hydrocephalus.
Despite >6 weeks of amphotericin B (400mg/day) and flucytosine (100 mg/kg/day), serial CSF cultures on hospital days 17, 23, 25, 40, and 56 remained positive for *C. neoformans *(Figure 4). A temporary lumbar drain was placed on hospital day 20 and removed after one week. The first sterile CSF culture was obtained on hospital day 72, approximately two weeks before VP shunt placement on hospital day 80 for persistently elevated ICPs (Figure 4).
Grpahical timeline showing the patient's hospital course.Gray indicates patient presentation and symptom evolution; red denotes positive CSF studies (LP and/or cultures); green denotes sterile CSF cultures; blue represents ICP-directed procedures; orange corresponds to antifungal therapy initiation or modification; purple denotes discharge disposition; black indicates other documented clinical events.
High-dose fluconazole (1200 mg/day) was initiated on hospital day 30 (Figure 4).
Headaches resolved with supportive care; imaging confirmed shunt patency. Renal function remained stable despite prolonged amphotericin B therapy. Ophthalmology follow-up confirmed persistent right-eye blurring and bilateral peripheral microaneurysms. She was transitioned to oral fluconazole (800 mg/day) for consolidation therapy and a dexamethasone taper. She was discharged on hospital day 86 (Figure 4) with outpatient follow-up arranged with infectious disease, neurosurgery, and neuro-ophthalmology.
Discussion
This case highlights a rare presentation of CM in an immunocompetent patient. Unlike the typical population of patients with advanced HIV, solid organ transplants, or other immunodeficiencies, our patient was immunocompetent with no evidence of underlying immunodeficiency.
Current guidelines recommend induction therapy with amphotericin B plus flucytosine for four to six weeks, followed by consolidation with fluconazole [1,7]. Most patients achieve sterile CSF cultures within two to four weeks. By contrast, our patient remained culture-positive for more than 70 days, which is rarely reported in immunocompetent hosts [4,5]. Notably, our patient remained culture positive despite clinical improvement. The persistence of positive CSF cultures for over 70 days despite guideline-directed antifungal therapy gives emphasis to the challenges of managing refractory cryptococcal infections.
The unusually prolonged persistence of positive CSF cultures in this case was likely multifactorial. A high initial fungal burden, medication intolerance requiring adjustment of antifungal therapy, and markedly elevated ICP may all have contributed to delayed CSF clearance.
CM most commonly affects immunocompromised patients; however, disease in immunocompetent individuals has been widely described in the literature. In such cases, presentation may be subacute, and diagnosis is often delayed. Our patient presented with headaches, dizziness, and visual changes, which are consistent with prior reports of cryptococcosis in immunocompetent hosts [4,5].
Reviews summarizing multiple cohorts note that 70-80% of CM cases occur in immunocompromised hosts overall, patients with HIV-associated CM typically present in their mid-30s (median 35-38 years), are predominantly male (58-80%), and have profound immunosuppression with median CD4 counts ~20-90 cells/µL, with ~75% presenting below 100 cells/µL [8,9]. On presentation, CM exhibits very high antigen titers, approximately 1:1280, with higher titers being associated with higher fungal burden and mortality [10].
By contrast, our patient was a 40-year-old female who was HIV negative and had a CD4 count of 1258 cells/µL; she was also negative for hepatitis C, further supporting that she was immunocompetent. Autoimmune etiologies were considered but ruled out, as the patient had negative ANA, RF, and ds-DNA testing. DM has been postulated as a risk factor for CM [11]. DM was ruled out in our patient due to a normal hemoglobin A1C and normal blood sugars.
Elevated ICP management
Elevated ICP is a well-recognized complication of CM, associated with high morbidity and mortality [1,3,12]. Standard management includes serial lumbar punctures, temporary lumbar drains, or VP shunting in refractory cases [6,13-16]. Our patient required multiple lumbar punctures, temporary lumbar drain placement, and ultimately VP shunt placement, which led to the resolution of headaches, but not the resolution of vision. This highlights the importance of timely recognition and escalation of ICP management strategies when the standard fails to achieve the desired therapeutic outcomes.
Obesity is not a risk factor for CM. However, there have been case reports of obese patients, who are otherwise immunocompetent, developing CM [11]. While there are no studies showing that obesity is a risk factor, our case adds to the growing body of literature suggesting that obesity and metabolic dysregulation play a role in the immune response to CM.
Conclusions
This case underscores several important lessons. CM can occur in immunocompetent hosts and should remain in the differential diagnosis for patients presenting with subacute meningitis symptoms, even in the absence of traditional risk factors. Persistent positive cultures require individualized management beyond standard guidelines, particularly when antifungal intolerance or complications arise. Aggressive monitoring and timely neurosurgical intervention for ICP management are essential to prevent irreversible neurologic damage.
In summary, our case highlights the potential for severe, refractory CM in an immunocompetent host, with a prolonged and complex clinical course. These findings emphasize the importance of vigilant monitoring, tailored antifungal therapy, and proactive ICP management to optimize outcomes. Further research is warranted to better define the role of comorbidities such as obesity and diabetes in the pathogenesis and progression of cryptococcal disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america Clin Infect Dis Perfect JR Dismukes WE Dromer F 2913225020102004748010.1086/649858 PMC 5826644 · doi ↗ · pubmed ↗
- 2Cryptococcosis: a model for the understanding of infectious diseases J Clin Invest Perfect JR 1893189512420142474315210.1172/JCI 75241 PMC 4001560 · doi ↗ · pubmed ↗
- 3Global guideline for the diagnosis and management of cryptococcosis: an initiative of the ECMM and ISHAM in cooperation with the ASM Lancet Infect Dis Chang CC Harrison TS Bicanic TA 051224202410.1016/S 1473-3099(23)00731-4PMC 1152641638346436 · doi ↗ · pubmed ↗
- 4Cryptococcal meningitis in young, immunocompetent patients: a single-center retrospective case series and review of the literature Open Forum Infect Dis Stack M Hiles J Valinetz E Gupta SK Butt S Schneider JG 010202310.1093/ofid/ofad 420PMC 1045621637636518 · doi ↗ · pubmed ↗
- 5Cryptococcal meningitis in an immunocompetent individual: a case report Clin Case Rep Acharya S Yadav SK Singh PB 09202110.1002/ccr 3.4894 PMC 848939434631078 · doi ↗ · pubmed ↗
- 6Shunting in cryptococcal meningitis J Neurosurg Cherian J Atmar RL Gopinath SP 17718612520162651776610.3171/2015.4.JNS 15255 · doi ↗ · pubmed ↗
- 7Treatment strategies for cryptococcal infection: challenges, advances and future outlook Nat Rev Microbiol Iyer KR Revie NM Fu C Robbins N Cowen LE 4544661920213355869110.1038/s 41579-021-00511-0PMC 7868659 · doi ↗ · pubmed ↗
- 8Cryptococcal meningoencephalitis in phenotypically normal patients Pathogens Cumagun PM Moore MK Mc Carty TP Mc Gwin G Pappas PG 12202310.3390/pathogens 12111303 PMC 1067472438003768 · doi ↗ · pubmed ↗