Pneumonia Risk in Institutionalized Older Adults With Severe Functional Dependency: An Exploratory Analysis Using Standardized Long‐Term Care Assessment Data
Yuichi Ohteru, Tomoyuki Kakugawa, Keita Murakawa, Masahiro Kakugawa, Tsunahiko Hirano, Kazuto Matsunaga

TL;DR
This study identifies risk factors for pneumonia in elderly nursing home residents using routine care data, showing that male sex, low albumin, poor cognition, and recent weight loss are key predictors.
Contribution
The study demonstrates that standardized long-term care assessments can identify pneumonia risk in resource-limited settings without comprehensive geriatric evaluations.
Findings
Male sex was associated with a 4.69-fold higher risk of pneumonia.
Lower serum albumin levels were linked to a 63% reduced risk of pneumonia.
Recent weight loss of ≥3% over six months increased pneumonia risk by 2.65 times.
Abstract
To identify risk factors for pneumonia among institutionalized older adults with severe functional dependency, using routinely available clinical information from the standardized “Doctor's Written Opinion” for long‐term care insurance. This retrospective observational study included 257 institutionalized older adults with severe functional dependency (median age, 88 years; 55 men and 202 women) residing in a Japanese nursing home between January 2014 and May 2020. Risk factors for pneumonia were analyzed using medical records and data from the standardized “Doctor's Written Opinion” for long‐term care insurance. During a median follow‐up of 2.1 years, 51 residents (19.8%) developed pneumonia, which was associated with lower overall survival (log‐rank test, p = 0.001). Among the 102 residents who died during this period, pneumonia was the most common cause of death (37% of deaths).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
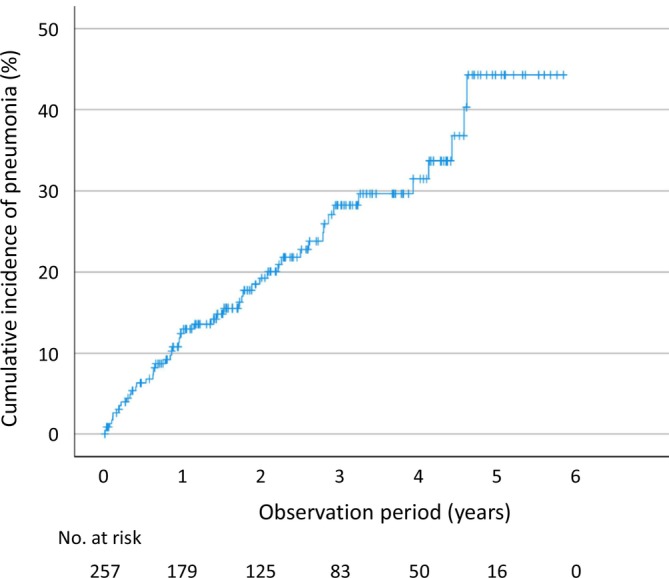 FIGURE 1
FIGURE 1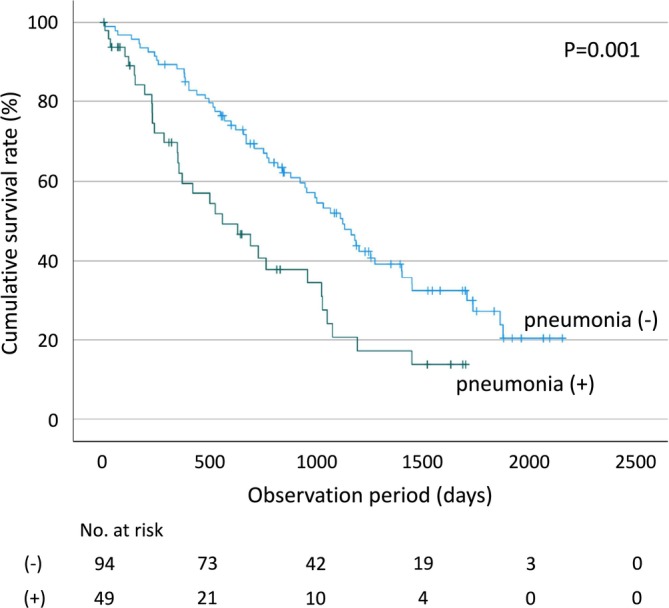 FIGURE 2
FIGURE 2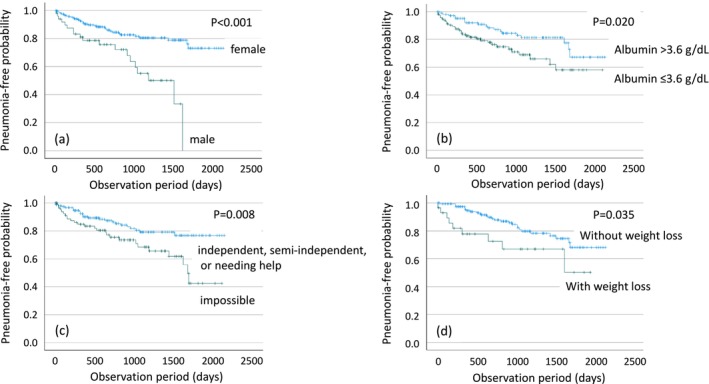 FIGURE 3
FIGURE 3| Non‐pneumonia |
| Pneumonia |
|
| |||
|---|---|---|---|---|---|---|---|
| ( | ( | ||||||
| Basic information | |||||||
| Age, median (IQR), years | 88.0 | (84.0–91.0) | 206 | 88.0 | (81.0–92.0) | 51 | 0.807 |
| Sex, | 206 | 51 | |||||
| Male | 36 | (17.5) | 19 | (37.3) | 0.002 | ||
| Female | 170 | (82.5) | 32 | (62.7) | |||
| BMI, median (IQR), kg/m2 | 19.7 | (17.9–21.5) | 205 | 19.9 | (17.9–22.2) | 51 | 0.748 |
| Comorbidities | |||||||
| HDS‐R, median (IQR) | 8.0 | (2.5–17.0) | 129 | 1.0 | (0.0–4.5) | 28 | < 0.001 |
| Charlson Comorbidity Index, median (IQR) | 2.0 | (1.0–3.0) | 202 | 2.0 | (1.0–3.0) | 51 | 0.688 |
| Cardiovascular disease, | 206 | 51 | |||||
| Yes | 31 | (15.0) | 7 | (13.7) | 0.812 | ||
| No | 175 | (85.0) | 44 | (86.3) | |||
| Cerebrovascular disease, | 206 | 51 | |||||
| Yes | 96 | (46.6) | 17 | (33.3) | 0.087 | ||
| No | 110 | (53.4) | 34 | (66.7) | |||
| Chronic lung disease, | 204 | 51 | |||||
| Yes | 5 | (2.4) | 1 | (2.0) | 0.659 | ||
| No | 201 | (97.6) | 50 | (98.0) | |||
| Hepatic disease, | 203 | 51 | |||||
| Yes | 12 | (5.9) | 4 | (7.8) | 0.536 | ||
| No | 191 | (94.1) | 47 | (92.2) | |||
| Diabetes mellitus, | 206 | 51 | |||||
| Yes | 38 | (18.4) | 9 | (17.6) | 0.895 | ||
| No | 168 | (81.6) | 42 | (82.4) | |||
| Solid tumor, | 206 | 51 | |||||
| Yes | 21 | (10.2) | 6 | (11.8) | 0.743 | ||
| No | 185 | (89.8) | 45 | (88.2) | |||
| Vaccinations | |||||||
| Pneumococcal vaccine, | 173 | 39 | |||||
| Yes | 88 | (50.9) | 17 | (43.6) | 0.412 | ||
| No | 85 | (49.1) | 22 | (56.4) | |||
| Influenza vaccine, | 201 | 14 | |||||
| Yes | 198 | (97.6) | 14 | (100.0) | 0.727 | ||
| No | 3 | (2.4) | 0 | (0.0) | |||
| Medications | |||||||
| ACE inhibitors, | 206 | 51 | |||||
| Yes | 8 | (3.9) | 2 | (3.9) | 0.624 | ||
| No | 198 | (96.1) | 49 | (96.1) | |||
| Gastric acid‐suppressive drugs, | 206 | 51 | |||||
| Proton pump inhibitor | 58 | (28.2) | 9 | (17.6) | 0.041 | ||
| Histamine H2‐receptor antagonists | 67 | (32.5) | 12 | (23.5) | |||
| No | 81 | (39.3) | 30 | (58.8) | |||
| Anticholinergic agents, | 206 | 51 | |||||
| Yes | 6 | (2.9) | 1 | (2.0) | 0.580 | ||
| No | 200 | (97.1) | 50 | (98.0) | |||
| Steroids, | 206 | 51 | |||||
| Yes | 7 | (3.4) | 1 | (2.0) | 0.506 | ||
| No | 199 | (96.6) | 50 | (98.0) | |||
| Hypnotics, | 206 | 51 | |||||
| Yes | 55 | (26.7) | 11 | (21.6) | 0.453 | ||
| No | 151 | (73.3) | 40 | (78.4) | |||
| Antipsychotics, | 206 | 51 | |||||
| Yes | 53 | (25.7) | 19 | (37.3) | 0.101 | ||
| No | 153 | (74.3) | 32 | (62.7) | |||
| Laboratory data | |||||||
| Serum hemoglobin, median (IQR), g/dL | 11.6 | (10.6–13.0) | 201 | 11.5 | (10.1–12.4) | 51 | 0.172 |
| Serum albumin, median (IQR), g/dL | 3.7 | (3.4–3.9) | 197 | 3.6 | (3.2–3.7) | 50 | 0.016 |
| Serum total protein, median (IQR), g/dL | 6.6 | (6.3–7.0) | 193 | 6.7 | (6.3–7.2) | 51 | 0.391 |
| Serum total cholesterol, median (IQR), mg/dL | 172.0 | (150.0–196.0) | 190 | 161.0 | (138.0–184.0) | 50 | 0.131 |
| eGFR, median (IQR), mL/min/1.73 m2 | 62.1 | (47.6–78.4) | 202 | 67.5 | (51.3–80.5) | 51 | 0.436 |
| Doctor's written opinion for long‐term care insurance | |||||||
| Nursing care level, | 131 | 21 | |||||
| Support Required 1 (High ADL) | 0 | (0.0) | 0 | (0.0) | 0.353 | ||
| Support Required 2 | 0 | (0.0) | 0 | (0.0) | |||
| Care Level 1 | 9 | (6.9) | 0 | (0.0) | |||
| Care Level 2 | 7 | (5.3) | 0 | (0.0) | |||
| Care Level 3 | 29 | (22.1) | 3 | (14.3) | |||
| Care Level 4 | 63 | (48.1) | 11 | (52.4) | |||
| Care Level 5 (Low ADL) | 23 | (17.6) | 7 | (33.3) | |||
| Independence degree of daily living for disabled older adults, | 206 | 51 | |||||
| Independent | 0 | (0.0) | 0 | (0.0) | 0.614 | ||
| J1 (High ADL) | 0 | (0.0) | 0 | (0.0) | |||
| J2 | 2 | (1.0) | 0 | (0.0) | |||
| A1 | 8 | (3.9) | 5 | (9.8) | |||
| A2 | 24 | (11.7) | 7 | (13.7) | |||
| B1 | 33 | (16.0) | 5 | (9.8) | |||
| B2 | 95 | (46.1) | 23 | (45.1) | |||
| C1 | 30 | (14.6) | 7 | (13.7) | |||
| C2 (Low ADL) | 14 | (6.8) | 4 | (7.8) | |||
| Independence degree of daily living for demented older adults, | 206 | 51 | |||||
| Independent | 6 | (2.9) | 1 | (2.0) | 0.102 | ||
| I (High ADL) | 18 | (8.7) | 0 | (0.0) | |||
| IIa | 15 | (7.3) | 3 | (5.9) | |||
| IIb | 31 | (15.0) | 6 | (11.8) | |||
| IIIa | 86 | (41.7) | 25 | (49.0) | |||
| IIIb | 26 | (12.6) | 5 | (9.8) | |||
| IV | 23 | (11.2) | 9 | (17.6) | |||
| M (Low ADL) | 1 | (0.5) | 2 | (3.9) | |||
| Impairment of short‐term memory, | 205 | 50 | |||||
| Yes | 183 | (89.3) | 47 | (94.0) | 0.235 | ||
| No | 22 | (10.7) | 3 | (6.0) | |||
| Cognitive ability for daily decision‐making, | 205 | 51 | |||||
| Independent | 15 | (7.3) | 2 | (3.9) | 0.030 | ||
| Semi‐independent | 52 | (25.4) | 7 | (13.7) | |||
| Needing help | 77 | (37.6) | 16 | (31.4) | |||
| Impossible | 61 | (29.8) | 26 | (51.0) | |||
| Ability to communicate intentions, | 204 | 51 | |||||
| Possible | 33 | (16.2) | 3 | (5.9) | 0.008 | ||
| A little difficult | 54 | (26.5) | 6 | (11.8) | |||
| Only specific requests | 78 | (38.2) | 25 | (49.0) | |||
| Impossible | 39 | (19.1) | 17 | (33.3) | |||
| Weight change over the past 6 months (≥ 3% change), | 169 | 37 | |||||
| Increase or stable | 144 | (85.2) | 28 | (75.7) | 0.157 | ||
| Decrease | 25 | (14.8) | 9 | (24.3) | |||
| Eating ability, | 205 | 51 | |||||
| Independent | 160 | (78.0) | 32 | (62.7) | 0.024 | ||
| Complete assistance | 45 | (22.0) | 19 | (37.3) | |||
| Social interaction, | 204 | 51 | |||||
| Independent | 31 | (15.2) | 3 | (5.9) | 0.008 | ||
| Partial assistance | 117 | (57.4) | 23 | (45.1) | |||
| Complete assistance | 56 | (27.5) | 25 | (49.0) | |||
| Univariate Cox analysis | Multivariate Cox analysis | |||
|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| |
| Basic information | ||||
| Age (years) | 1.004 (0.965–1.043) | 0.856 | ||
| Sex, male | 3.004 (1.682–5.365) | < 0.001 | 4.692 (2.352–9.357) | < 0.001 |
| Body mass index | 0.962 (0.877–1.055) | 0.412 | ||
| Medications | ||||
| ACE inhibitors, yes | 0.457 (0.110–1.898) | 0.281 | ||
| Gastric acid‐suppressive drugs, yes | 0.567 (0.324–0.991) | 0.046 | 0.612 (0.295–1.270) | 0.188 |
| Laboratory data | ||||
| Serum albumin level (g/dL) | 0.305 (0.154–0.604) | < 0.001 | 0.368 (0.151–0.898) | 0.028 |
| Serum total cholesterol level (mg/dL) | 0.991 (0.983–1.000) | 0.047 | ||
| Doctor's written opinion for long‐term care insurance | ||||
| Nursing care level | 2.063 (1.169–3.642) | 0.013 | ||
| Impairment of short‐term memory, yes | 1.676 (0.521–5.390) | 0.386 | ||
| Cognitive ability for daily decision‐making level | 1.597 (1.147–2.226) | 0.006 | 1.626 (1.082–2.444) | 0.019 |
| Body weight loss of ≥ 3% over the past 6 months, yes | 2.239 (1.056–4.748) | 0.036 | 2.645 (1.195–5.858) | 0.016 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Pneumonia and Respiratory Infections · Chronic Disease Management Strategies
Introduction
1
The global aging trend is expected to substantially increase the burden of respiratory infections [1]. Older adults face a higher risk of severe respiratory infections, with pneumonia‐related mortality disproportionately affecting those aged ≥ 65 years [2, 3, 4, 5, 6]. Moreover, community‐acquired pneumonia (CAP) is associated with sustained declines in quality of life (QOL) and activities of daily living (ADL), with many patients failing to regain pre‐disease functional status even 1 year after onset [6, 7, 8]. Pneumonia also imposes a considerable economic burden [9, 10, 11]. These factors underscore the need for effective prevention strategies. Identifying risk factors is essential, particularly through simple, practical tools that can pinpoint high‐risk individuals and enable timely, targeted interventions in resource‐limited settings.
Studies have identified several pneumonia risk factors among older residents of long‐term care facilities. Key individual‐level factors include advanced age [12, 13], male sex [13, 14], cognitive impairment [15, 16, 17, 18], swallowing dysfunction [13, 14], immobility or reduced ADL [12, 13], malnutrition [12, 19], and poor oral hygiene [20, 21, 22, 23, 24, 25, 26]. Evidence also links sarcopenia—characterized by reduced skeletal muscle mass and strength—to lower tongue pressure and respiratory muscle weakness, which increases pneumonia risk in older nursing home residents [27, 28, 29]. These muscle impairments are associated with dysphagia, diminished cough efficacy, and compromised airway protection, the key mechanisms underlying aspiration pneumonia.
Previous studies often relied on complex, time‐consuming assessments requiring specialized equipment, such as videofluoroscopic swallowing studies, respiratory muscle strength testing, and detailed cognitive evaluations (e.g., the Global Deterioration Scale). Similarly, sarcopenia assessment typically involves objective measurements of muscle mass (e.g., bioelectrical impedance analysis or dual‐energy X‐ray absorptiometry), muscle strength (e.g., handgrip dynamometry), and physical performance (e.g., gait speed). These approaches are impractical for routine use in most long‐term care facilities. Despite robust evidence linking these factors to pneumonia risk, studies employing simple, scalable tools suitable for resource‐limited settings are lacking. Addressing this methodological gap is essential for timely prevention in older adults with severe functional dependency residing in institutional care settings.
To address this gap, we used the “Doctor's Written Opinion for Long‐Term Care Insurance” (hereafter referred to as the “doctor's written opinion”)—a standardized and mandatory document in Japan, completed by physicians for all older adults applying for long‐term care services [30, 31]. This form records physical function, cognitive status, nutritional condition, and comorbidities, and determines care levels nationwide. Its simplicity makes it a practical source of information for pneumonia risk assessment among institutionalized older adults with severe functional dependency, especially in resource‐limited settings. We investigated whether information from this document, together with routinely available clinical data, could support the identification of individuals at increased risk of pneumonia without requiring complex clinical assessments.
Methods
2
Study Population
2.1
This retrospective observational study included all residents admitted to the Hofu Akari‐en Special Nursing Home, a government‐licensed long‐term care facility in Yamaguchi, Japan, between January 2014 and May 2020. In Japan, Special Nursing Homes primarily accommodate older adults with substantial physical and/or cognitive impairments who require 24‐h assistance with nearly all ADL. Admission is generally restricted to individuals certified as Care Level 3–5 under the national long‐term care insurance system, reflecting a high degree of functional dependency and care needs. The facility admission date was defined as the start of the observation period. Residents unable to tolerate oral or enteral feeding were excluded from the study. The study protocol complied with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Yamaguchi University Hospital, Ube, Japan (Approval No. 2020‐100). In accordance with the ethical guidelines set by the Japanese Ministry of Health, Labour and Welfare, the requirement for individual informed consent was waived for this retrospective study. Instead, residents' right to refuse participation was communicated via a notice posted on the facility's bulletin board.
Covariates
2.2
The characteristics of the study population were obtained from medical records and routinely available clinical data, including age, sex, body mass index (BMI), cognitive function assessed using the Hasegawa Dementia Scale‐Revised (HDS‐R) scores [32], medical history, comorbidities, vaccination status for pneumococcal vaccines (23‐valent pneumococcal polysaccharide vaccine and 13‐valent pneumococcal conjugate vaccine), influenza vaccine, medication history, and laboratory parameters (hemoglobin, albumin, total protein, total cholesterol, and creatinine). Information regarding smoking history could not be obtained because of impaired cognitive abilities or the absence of relevant documentation in medical records. Additional data related to long‐term care insurance included nursing care level, classified into seven categories from Support Required 1 (indicating high ADL function) to Care Level 5 (indicating low ADL function); independence degree of daily living for disabled older adults (Table S1); independence degree of daily living for demented older adults (Table S2); impairment of short‐term memory (present or absent); cognitive ability for daily decision‐making (independent, semi‐independent, needing help, or impossible); ability to communicate intentions (possible, a little difficult, only specific requests, or impossible); weight change over the past 6 months (“increase,” “stable,” or “decrease,” with a change exceeding 3% considered clinically significant based on guidelines from the Ministry of Health, Labour and Welfare in Japan); eating ability (independent or requiring complete assistance); and social interaction (independent, requiring partial assistance, or requiring complete assistance). The Charlson Comorbidity Index [33] was calculated based on medical history and comorbidities. The first pneumonia event, including the date of diagnosis and associated outcomes during the observation period, was recorded for each patient.
Clinical and Outcome Assessments
2.3
The primary outcome was the time to the first episode of pneumonia during the observation period. Residents were followed from the date of facility admission until the occurrence of the first pneumonia event, hospital admission for any condition other than pneumonia, or loss to follow‐up by May 31, 2020, whichever occurred first. Hospital admission for conditions other than pneumonia and loss to follow‐up were treated as censoring events in the time‐to‐pneumonia analysis.
For survival analysis, residents were followed from the date of facility admission until death from any cause. Residents were censored if they were alive as of May 31, 2020, or lost to follow‐up.
Statistical Analysis
2.4
Baseline characteristics—including age, sex, BMI, HDS‐R score, medical history, complications, vaccination history, medication history, laboratory data, and information related to long‐term care insurance—were compared between the pneumonia onset and non‐onset groups. Summary statistics are presented as frequencies for categorical variables or medians and IQR for quantitative variables. Inter‐group differences were evaluated using Fisher's exact test for categorical variables and the Wilcoxon rank‐sum test for quantitative variables. Time to the first episode of pneumonia was assessed using Kaplan–Meier analysis, and pneumonia‐free survival curves were estimated. Differences between Kaplan–Meier curves were assessed using the log‐rank test. For multivariate analysis of pneumonia risk, Cox's proportional hazards regression model was used to explore multiple factors associated with pneumonia development. Adjusted hazard ratio (HR) and 95% confidence intervals (95% CI) were calculated for each risk factor. To ensure reproducibility, no more than five explanatory variables (each with > 50 cases) were included owing to the limited sample size (N = 257). Hence, in the multivariate Cox regression modeling, a stepwise selection method with a threshold p‐value of 0.05 was performed. The goodness‐of‐fit of the Cox regression model was evaluated using the concordance index (C‐index). The log‐rank test was used to evaluate differences in Kaplan–Meier curves for pneumonia risk factors identified by Cox analysis. In this analysis, numerical variables were treated as binary variables using cutoff values estimated by receiver operating characteristic (ROC) analysis.
All statistical analyses were performed using IBM SPSS Statistics for Windows version 27 (IBM, Armonk, NY, USA).
Results
3
Residents' Characteristics
3.1
Table S3 presents the baseline characteristics of the nursing home residents included in this study. The study cohort comprised 257 residents (55 men and 202 women) with a median age of 88.0 years (IQR, 84.0–91.5). The median follow‐up duration was 2.1 years (IQR, 1.0–3.7); the median survival time (MST) was 2.7 years from the start of observation.
Overall, 89.5% of residents had a “nursing care level” rating of Care Level 3–5, and 82.1% had an “independence degree of daily living for disabled older adults” rating of B–C. Based on these functional assessments, > 80% of residents were estimated to have an Eastern Cooperative Oncology Group Performance Status of 3 or 4 [34], indicating marked functional impairment and advanced care needs.
Pneumonia Incidence
3.2
During follow‐up, pneumonia occurred in 51 residents (19.8%), while 2 residents (0.8%) were lost to follow‐up. Kaplan–Meier analysis estimated pneumonia incidence rates of 12.4% at 1 year, 19.2% at 2 years, and 28.2% at 3 years (Figure 1).
Cumulative incidence of pneumonia in nursing home residents. Kaplan–Meier analysis estimated pneumonia incidence rates of 12.4% at 1 year, 19.2% at 2 years, and 28.2% at 3 years.
Impact of Pneumonia on Overall Survival
3.3
Pneumonia was significantly associated with overall survival among nursing home residents. Those who developed pneumonia had a significantly shorter MST (558 days) compared with those who did not (1120 days) (log‐rank test, p = 0.001) (Figure 2). During the follow‐up period, 102 residents died. According to recorded causes of death, pneumonia was the most common cause, accounting for 37% of all deaths (Figure S1).
Comparison of cumulative survival rates in pneumonia and non‐pneumonia groups. Nursing home residents who developed pneumonia during the observation period exhibited a significantly shorter median survival time (MST, 558 days) compared with those who did not (1120 days) (log‐rank test, p = 0.001).
Comparison of Baseline Characteristics Between Nursing Home Residents With and Without Pneumonia
3.4
Table 1 presents a comparison of the baseline characteristics between residents who developed pneumonia and those who did not. Significant differences were observed between the two groups in sex (p = 0.002), HDS‐R score (p < 0.001), use of gastric acid‐suppressive drugs (p = 0.041), serum albumin levels (p = 0.016), cognitive ability for daily decision‐making (p = 0.030), ability to communicate intentions (p = 0.008), eating ability (p = 0.024), and social interaction (p = 0.008).
Risk Factors for Pneumonia
3.5
In the univariate Cox analysis (Table 2), male sex, no gastric acid‐suppressive drug use, lower serum albumin level, lower serum total cholesterol level, higher nursing care level, impaired cognitive ability for daily decision‐making, and weight loss of ≥ 3% over the past 6 months were associated with an increased risk of pneumonia. For the multivariate Cox analysis, five risk factors for pneumonia were selected using stepwise selection: sex, use of gastric acid‐suppressive drugs, serum albumin level, cognitive ability for daily decision‐making level, and weight loss of ≥ 3% over the past 6 months. In the final multivariate model, male sex, lower serum albumin levels, impaired cognitive ability for daily decision‐making, and weight loss of ≥ 3% over the past 6 months were independently associated with pneumonia development, with respective HR [95% CI], 4.692 [2.352–9.357], 0.368 [0.151–0.898], 1.626 [1.082–2.444], and 2.645 [1.195–5.858] (Table 2). Here, the HR for “cognitive ability for daily decision‐making” indicates that with each one‐level decline in evaluation (e.g., from independent to semi‐independent), the risk of pneumonia increases by a factor of 1.626. The overall goodness‐of‐fit of the regression model, calculated using the C‐index, was 0.724, indicating moderate discriminative ability of the model. The associations between these four variables and pneumonia‐free probability, as evaluated by the log‐rank test, are shown in Figure 3. ROC curve analysis revealed 3.6 g/dL as a cutoff level for serum albumin in relation to pneumonia risk. The log‐rank test demonstrated that male sex, serum albumin levels ≤ 3.6 g/dL, impaired cognitive ability for daily decision‐making, and weight loss of ≥ 3% over the past 6 months were significantly associated with decreased pneumonia‐free survival probability (p < 0.001, p = 0.020, p = 0.008, and p = 0.035, respectively).
Associations between risk factors for pneumonia and pneumonia‐free probability. Kaplan–Meier curves illustrate pneumonia‐free probability based on the following risk factors: (a) sex, comparing males and females; (b) serum albumin levels, categorized as > 3.6 g/dL and ≤ 3.6 g/dL; (c) cognitive ability for daily decision‐making, divided into two groups: “impossible” and “independent, semi‐independent, or needing help”; and (d) weight loss of ≥ 3% over the past 6 months, categorized into groups with and without such weight loss.
Discussion
4
Older adults with severe functional dependency are at high risk of pneumonia, which is associated with adverse outcomes [2, 3, 4, 5, 6, 7, 8, 19, 22, 35]. In our cohort, nearly one‐fifth of residents developed pneumonia, which was the leading recorded cause of death (37% of fatalities). Those with pneumonia had a markedly shorter MST compared with those who did not. These findings indicate that pneumonia is not only a frequent complication but is also associated with reduced survival in this population. Identifying high‐risk individuals using feasible, time‐efficient methods is therefore critical. In this study, male sex, lower serum albumin levels, impaired cognitive ability for daily decision‐making, and ≥ 3% weight loss over the past 6 months were independently associated with the occurrence of pneumonia among institutionalized older adults with severe functional dependency.
Importantly, these risk factors can be assessed using simple measures routinely available in long‐term care settings. Cognitive ability for daily decision‐making was rated on a four‐point scale during standard physician–patient interactions, avoiding complex tools such as the Global Deterioration Scale [18, 36, 37, 38, 39]. Similarly, weight loss can be identified through brief patient interviews or routine care documentation, and serum albumin levels are readily available from standard blood tests. Together, these findings may inform a pragmatic, context‐specific approach to pneumonia risk stratification among institutionalized older adults with severe functional dependency, particularly in resource‐limited long‐term care settings.
Sarcopenia is associated with an increased risk of pneumonia in older adults [27, 28, 29, 40, 41]. Weakness of the respiratory and swallowing muscles may reduce cough efficacy and airway protection, thereby predisposing individuals to aspiration [28, 29, 42, 43]. Low BMI, particularly in the underweight range, has been consistently associated with sarcopenia and is frequently regarded as an indirect marker of nutritional and functional vulnerability in older adults [44, 45, 46, 47]. Low BMI is independently associated with an increased risk of pneumonia and pneumonia‐related mortality [17, 48]. Beyond static BMI, prior studies have highlighted the prognostic relevance of weight change itself. Both low body weight and recent weight loss are independent risk factors for CAP in community‐dwelling older adults [49], and substantial changes in body weight over 5 years have been associated with higher pneumonia‐related mortality in a large Japanese cohort [50].
Our findings extend previous observations to a highly vulnerable population—very old institutionalized residents with severe functional dependency—by demonstrating that even modest short‐term weight loss (≥ 3% over 6 months) was associated with a higher likelihood of pneumonia than a persistently low but stable BMI. This finding suggests that tracking trajectories of body weight, rather than relying solely on static BMI values, may provide a dynamic and clinically meaningful marker for pneumonia risk in geriatric care settings. In our cohort, both the pneumonia and non‐pneumonia groups exhibited low median BMI values (19.9 and 19.7, respectively), indicating chronic undernutrition. In this context, further declines in BMI may reflect loss of lean body mass, particularly skeletal muscle, rather than reductions in adiposity. Therefore, unlike community‐dwelling older adults with more heterogeneous body composition, serial declines in BMI among institutionalized older adults with severe functional dependency may serve as a practical surrogate marker of progressive muscle loss, including sarcopenia‐related changes. Prospective studies incorporating direct assessments of muscle mass and function are warranted to validate these observations and to further elucidate the biological pathways linking muscle loss and pneumonia risk in institutionalized older populations.
Malnutrition is a risk factor for pneumonia. In our study, hypoalbuminemia and ≥ 3% weight loss over 6 months were independently associated with pneumonia occurrence among institutionalized older adults with severe functional dependency. Malnutrition increases infection susceptibility through multiple immune impairments [51, 52, 53, 54, 55, 56, 57]. Severe nutritional deficits may also lead to thymic atrophy and attenuated vaccine‐induced antibody production [54]. Taken together, our findings suggest that weight loss and hypoalbuminemia reflect overlapping domains of nutritional and physiological vulnerability that may contribute to increased susceptibility to pneumonia.
Progressive weight loss may also reflect involvement in a vicious cycle: malnutrition increases the risk of dysphagia, which, in turn, reduces dietary intake and worsens nutritional status [58, 59, 60, 61]. Videofluorographic studies have identified malnutrition as an independent risk factor for high‐risk dysphagia [59], while older adults with dysphagia are nearly five times more likely to be undernourished [61]. Poor oral hygiene may further accelerate this cycle [60]. For individuals with ongoing weight loss, tailored nutritional and supportive interventions—such as texture‐modified diets, high‐calorie supplements, and appropriate dental care—may help interrupt this cycle and potentially limit further decline, although prospective interventional studies are needed to confirm their effectiveness.
Hypoalbuminemia, while often considered a marker of malnutrition, also reflects chronic inflammation, which suppresses hepatic albumin synthesis and accelerates protein catabolism [62, 63]. In older adults with CAP, inflammation—rather than nutritional deficits—has been reported to be a major contributor to hypoalbuminemia [64]. Chronic inflammation promotes immunosuppressive pathways and may increase susceptibility to infection [65]. Hypoalbuminemia is associated with diminished humoral immune responses to coronavirus disease 2019 mRNA vaccination in older adults, highlighting its broader relevance to immune dysfunction [66]. In the present study, lower serum albumin level was independently associated with pneumonia occurrence, consistent with earlier reports [67, 68]. Taken together, these findings suggest the importance of disentangling the relative contributions of malnutrition and inflammation. Further investigation is warranted into whether strategies targeting inflammation, in addition to nutritional support, may potentially reduce pneumonia risk among institutionalized older adults with severe functional dependency.
This study has certain limitations. First, the relatively small sample size may limit the generalizability of the findings. Second, the retrospective design introduces potential selection and information biases that cannot be fully excluded. Third, the study was conducted at a single institution, potentially restricting the external validity. In addition, the use of standardized long‐term care assessment data embedded within the Japanese national long‐term care insurance system further limits the generalizability of our findings to broader or international contexts, as these instruments are not routinely used outside Japan. Fourth, although aspiration pneumonia was likely the predominant subtype given the very old age and severe functional dependency of our study population [69, 70, 71, 72], definitive classification was not feasible owing to the lack of widely accepted diagnostic criteria and limited clinical data. Therefore, all pneumonia events were analyzed as a single outcome. Fifth, the observation period was relatively short, possibly limiting the identification of long‐term risk factors. Finally, our analysis focused on the time to the first pneumonia event after admission to provide a uniform baseline and minimize confounding from prior episodes, given that a history of pneumonia is a strong predictor of recurrence [73, 74]. While this approach is methodologically appropriate for the present exploratory study design and limited sample size, it does not capture the full cumulative burden of pneumonia over time. Future multicenter, prospective studies with longer follow‐up in diverse long‐term care systems beyond Japan are warranted to validate these findings and evaluate their broader applicability before any practical application can be considered.
Conclusion
5
Male sex, lower serum albumin levels, impaired cognitive ability for daily decision‐making, and weight loss of ≥ 3% over the past 6 months were associated with an increased risk of pneumonia among institutionalized older adults with severe functional dependency. Information routinely available in standardized long‐term care assessments may support the identification of individuals at increased risk of pneumonia in resource‐limited long‐term care settings where comprehensive geriatric assessments are not feasible. In addition, our findings regarding their associations with pneumonia may provide hypothesis‐generating evidence for future prevention research in long‐term care settings.
Author Contributions
T.K. conceived the fundamental study concept and outlined the methodology. Y.O. and T.K. designed this study. Y.O. and T.K. accessed, verified, and reviewed the data. Y.O. and T.K. wrote the manuscript. All authors had full access to all the data in this study and vouched for the accuracy and completeness of the data, data analyses, and the interpretation and fidelity of the protocol. All authors have reviewed, edited, and approved the final version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
Ethics Statement
The study protocol was approved by the Institutional Review Board of Yamaguchi University Hospital, Ube, Japan (Approval No. 2020‐100).
Consent
The requirement for individual informed consent was waived for this retrospective study. Resident's right to refuse participation was communicated via a notice posted on the facility's bulletin board.
Conflicts of Interest
T.K. is an employee of the Department of Pulmonology and Gerontology, Graduate School of Medicine, Yamaguchi University, Ube, Japan, and is funded by the Medical Corporation WADOKAI. Y.O., T.K., and M.K. are employees of Hofu Rehabilitation Hospital, Hofu, Japan, which belongs to the Medical Corporation WADOKAI. M.K. is a board member of Medical Corporation WADOKAI (unpaid). The authors declare no conflicts of interest.
Supporting information
Figure S1: Cause of death among nursing home residents. Table S1: Independence degree of daily living for disabled older adults. Table S2: Independence degree of daily living for demented older adults. Table S3: Baseline characteristics of nursing home residents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. A. Kline and D. M. Bowdish , “Infection in an Aging Population,” Current Opinion in Microbiology 29 (2016): 63–67.26673958 10.1016/j.mib.2015.11.003 · doi ↗ · pubmed ↗
- 2T. N. Pham , C. B. Kramer , and M. B. Klein , “Risk Factors for the Development of Pneumonia in Older Adults With Burn Injury,” Journal of Burn Care & Research 31, no. 1 (2010): 105–110.20061844 10.1097/BCR.0b 013e 3181 cb 8c 5a PMC 3045669 · doi ↗ · pubmed ↗
- 3T. J. Marrie , “Community‐Acquired Pneumonia in the Elderly,” Clinical Infectious Diseases 31, no. 4 (2000): 1066–1078.11049791 10.1086/318124 · doi ↗ · pubmed ↗
- 4N. Miyashita and Y. Yamauchi , “Bacterial Pneumonia in Elderly Japanese Populations,” Japanese Journal of Clinical Medicine 9 (2018): 1179670717751433.10.1177/1179670717751433 PMC 580499829434484 · doi ↗ · pubmed ↗
- 5H. Igari , K. Yamagishi , S. Yamazaki , et al., “Epidemiology and Treatment Outcome of Pneumonia: Analysis Based on Japan National Database,” Journal of Infection and Chemotherapy 26, no. 1 (2020): 58–62.31353202 10.1016/j.jiac.2019.07.001 · doi ↗ · pubmed ↗
- 6M. J. Mangen , S. M. Huijts , M. J. Bonten , and G. A. de Wit , “The Impact of Community‐Acquired Pneumonia on the Health‐Related Quality‐Of‐Life in Elderly,” BMC Infectious Diseases 17, no. 1 (2017): 208.28292280 10.1186/s 12879-017-2302-3PMC 5351062 · doi ↗ · pubmed ↗
- 7T. Kato , N. Miyashita , Y. Kawai , et al., “Changes in Physical Function After Hospitalization in Patients With Nursing and Healthcare‐Associated Pneumonia,” Journal of Infection and Chemotherapy 22, no. 10 (2016): 662–666.27493023 10.1016/j.jiac.2016.06.005 · doi ↗ · pubmed ↗
- 8H. A. Glick , T. Miyazaki , K. Hirano , et al., “One‐Year Quality of Life Post‐Pneumonia Diagnosis in Japanese Adults,” Clinical Infectious Diseases 73, no. 2 (2021): 283–290.32447366 10.1093/cid/ciaa 595PMC 8282327 · doi ↗ · pubmed ↗