Physiological changes of cortisol and oxytocin following manual therapy: a scoping review
Andy T. Cao, Murdi S. Alanazi, Rebecca Billings, William R. Reed

TL;DR
This review maps how manual therapy affects cortisol and oxytocin levels, highlighting inconsistent findings and the need for standardized research methods.
Contribution
The study provides a comprehensive scoping review of cortisol and oxytocin responses to manual therapy, identifying gaps and variability in the literature.
Findings
Cortisol and oxytocin responses to manual therapy were highly variable across studies.
Fewer studies focused on oxytocin compared to cortisol, revealing a gap in the evidence.
Heterogeneity in study design and methods complicates interpretation of results.
Abstract
Neuroendocrine responses to manual therapy (MT), including changes in cortisol and oxytocin, have long been proposed as potential physiological mechanisms of MT-related effects. Over the past three decades, a growing body of literature has examined hormonal/neuropeptide responses following MT; however, findings remain heterogeneous and unevenly distributed across outcomes and MT intervention types. The objective of this scoping review was to map and characterize the existing evidence for changes in cortisol (CORT) and/or oxytocin (OXT) levels in response to three commonly used MT interventions and to identify patterns and gaps within the literature. Five databases [Cumulated Index to Nursing and Allied Health Literature (CINAHL), Embase, PubMed, Scopus, and Web of Science] were searched from inception to July 2025. Eligible studies included those which were (a) in English, (b) in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
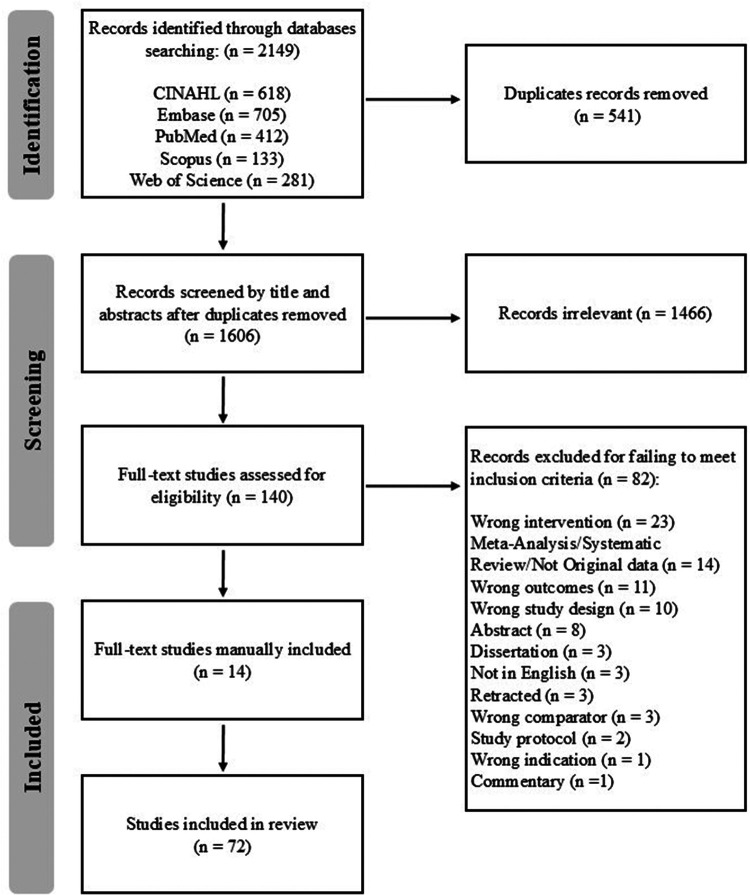 Figure 1
Figure 1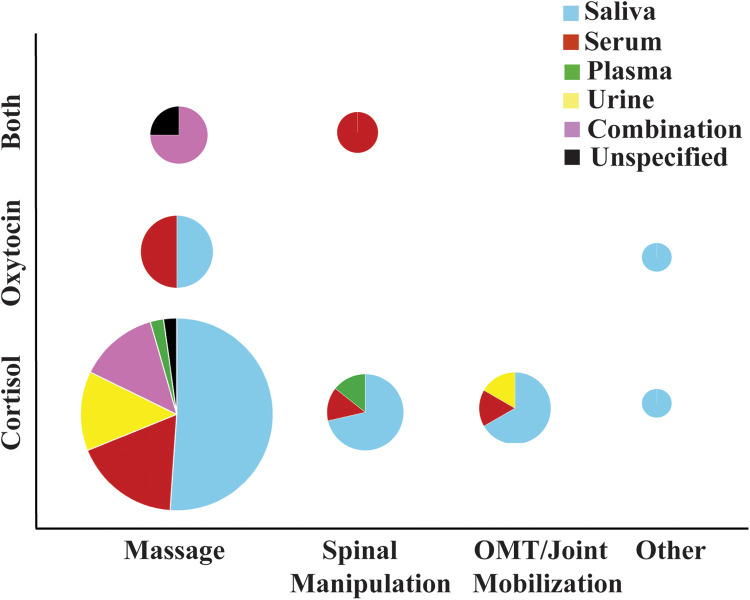 Figure 2
Figure 2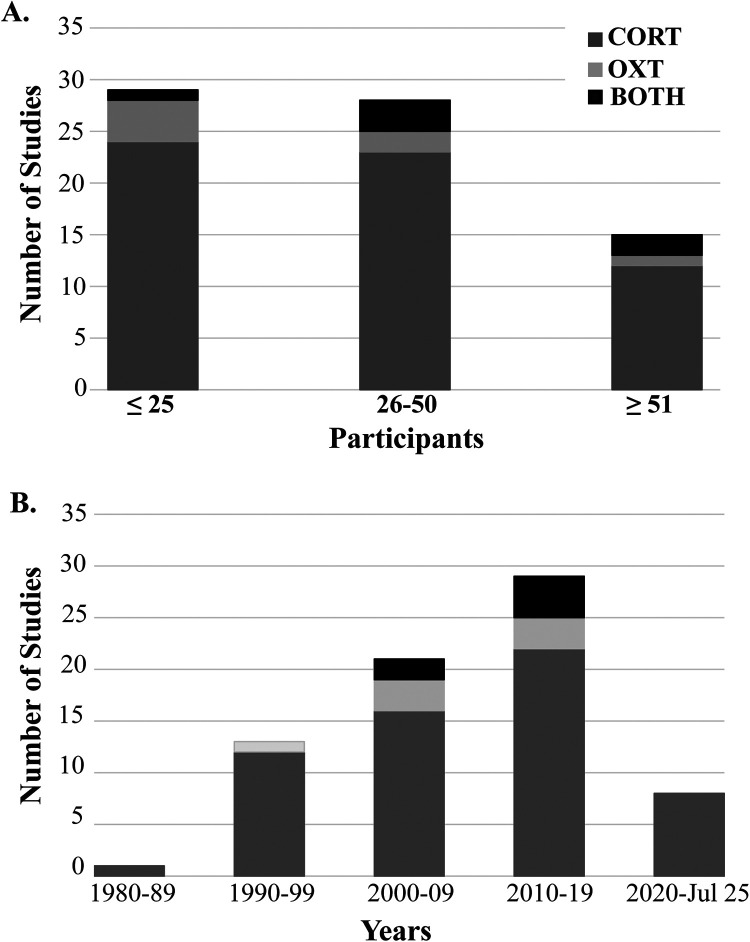 Figure 3
Figure 3| Author/s | Sample size | Intervention | Duration | Symptoms | Biological Measures | Outcome |
|---|---|---|---|---|---|---|
| Adib-Hajbaghery et al. (2013) ( | 60 adults | Whole body massage | 60 min—1 session | Patients in coronary care unit | Serum | CORT N.S. |
| Arroyo-Morales et al. (2009 ( | 60 adults | Massage | 40 min—single session | Healthy | Saliva | CORT N.S. |
| Bennett et al. (2016) ( | 36 students | Massage—Thai | 90 min—1 session | Stress | Saliva | CORT ↓ but so did the control |
| Bost and Wallis (2006) ( | 60 | Massage—Swedish | 15 min—1/wk—5 wks | Healthy | Urine | CORT N.S. |
| Christian et al. (1988) ( | 40 males | Spinal manipulative therapy | 1 session | Acute spinal pain | Plasma | CORT N.S. |
| de Oliveira et al. (2018) ( | 24 adult females | Massage—Swedish | 40 min—2/wk—3 months | Fibromyalgia | Saliva | CORT N.S. |
| Donoyama et al. (2010) ( | 15 females | Massage—Anma | 40 min—2/wk—4 wks | Healthy | Saliva | CORT N.S. |
| Donoyama and Shibasaki (2010) ( | 8 females | Massage—Anma | 40 min—1 session | Muscle stiffness | Saliva | CORT ↓ but so did control |
| Donoyama and Norio Toyomi. (2011) ( | 10 females | Massage—Japanese | Eight 40 min/2 wks | Cancer survivors vs. Healthy | Saliva | CORT N.S. |
| Henderson et al. (2010) ( | 17 adults | Rib raising | 5 min | Healthy | Saliva | CORT N.S. |
| Hernandez-Reif et al. (2001) ( | 24 | Massage | 30 min—2/wk—5 wks | Low back pain | Urine | CORT N.S. |
| Hernandez-Reif et al. (2002) ( | 16 adults | Massage | 30 min—2/wk—5 wks | Parkinson’s disease | Urine | CORT N.S. |
| Hernandez-Reif et al. (2004) ( | 34 women | Massage | 30 min—3/wk—5 wks | Stage 1/2 breast cancer | Urine | CORT N.S. |
| Khilnani et al. (2003) ( | 30 adolescents | Massage | 20 min—2/wk -1 month | ADHD | Saliva | CORT N.S. |
| Kim et al. (2001) ( | 59 adults | Hand massage | 20 min | Cataract surgery | Blood (not specified) | CORT N.S. |
| Kovanur-Sampath et al. (2017) ( | 24 males | Thoracic manipulation | 1 session | Healthy | Saliva | CORT N.S. |
| Kucuk Alemdar et al. (2023) ( | 99 adolescents | Hand massage | 20 min | Pediatric ICU | Serum | CORT N.S. |
| Lindgren et al. (2013) ( | 20 | Touch massage | 60 min—1 session | Anxiety | Serum | CORT N.S. |
| Lohman et al. (2019) ( | 28 females | Cervical spine manipulation | 1 session | Non-specific mechanical neck pain | Serum | CORT N.S., OXT ↑ |
| Lovas et al. (2002) ( | 2 female adults | Massage—Swedish | 2x—1 hour—1/wk, 4 wks | Healthy | Serum | CORT N.S. |
| McRee et al. (2003) ( | 42 adults | Massage—Swedish | 1 session—30 min | Surgery patients | Serum | CORT N.S. |
| Noto et al. (2010) ( | 25 young females | Back massage | 10 min | Healthy | Saliva | CORT N.S. |
| Nuno et al. (2019) ( | 2 adults | Osteopathic manipulative treatments | 30 min—3 session/7 wks | Healthy | Urine | N/A |
| Post-White et al. (2009) ( | 23 children | Massage | ∼30 min—4/wk | Cancer—chemotherapy | Saliva | CORT N.S. |
| Rapaport et al. (2010) ( | 53 adults | Massage—Swedish | 45 min—1 session | Healthy | Saliva + Serum | CORT N.S. |
| Rapaport et al. (2012) ( | 45 young adults | Massage—Swedish | 45 min | Healthy | Saliva + Plasma | CORT N.S. |
| Schaub et al. (2018) ( | 40 | Hand massage | 16-20 min—7 sessions over 3 wks | Agitated patients with dementia | Saliva | CORT N.S. |
| Silva et al. (2020) ( | 40 | Suboccipital fascial release | 5 min—1 session | Healthy | Saliva | CORT ↓ but so did the control |
| Taylor et al. (2003) ( | 105 females | Massage—Swedish | 45 min—3 consecutive evenings | Postsurgical pain, negative affect, and stress | Urine | CORT N.S. |
| Wändell et al. (2010) ( | 53 adults | Tactile massage | 1 hour | Type 2 diabetes | Urine | CORT N.S. |
| Whelan et l. (2002) ( | 30 males | Cervical spine manipulation | 1 session | Healthy | Saliva | CORT N.S. |
| Author/s | Sample size | Intervention | Duration | Symptoms | Biological Measures | Outcome |
|---|---|---|---|---|---|---|
| Adib-Hajbaghery et al. (2015) ( | 90 males | Massage | 60 min—1 session | CVD | Serum | CORT ↓ |
| Andersson, K. (2004) ( | 11 females | Tactile massage | 60 min—1/wk—10 wks | Type 2 diabetes | Blood (nots specified) | OXT N.S. but CORT ↓ |
| Boghrabadi et al. (2017) ( | 24 females with type 2 diabetes | Massage | 30 min—3/week—1 month | Diabetic | Serum | CORT ↓ in the experimental group after 12 sessions ( |
| Aparecida Martins (2023) ( | 41 | Massage—Shiatsu | Limb fracture | Saliva | CORT ↓ | |
| Ditzen et al. (2007) ( | 67 females | Massage | 10 min—1 session | Stressed | Saliva (CORT) + Plasma (OXT) | CORT ↓, OXT N.S. |
| Farrell et al. (2023) ( | 20 adults | Cervical spine mobilization | 12 min (6 min/segment—2 segments) | Healthy | Saliva | CORT ↓ |
| Farrell et al. (2024) ( | 19 adult males | Cervical spine mobilization | 12 min (6 min/segment—2 segments) | Persistent-concussion symptoms | Saliva | CORT ↓ |
| Field et al. (1992) ( | 72 children | Massage | 30 min—1/ day—5 days | Depressed + adjustment disorder | Saliva + Urine | sCORT ↓, uCORT ↓, but only in the depressed group |
| Field et al. (1996) ( | 32 females | Massage | 30 min—2/wk—5 wks | Depressed | Saliva + Urine | CORT ↓ |
| Field et al. (1997) ( | 20 children | Massage—stroking | 15 min/day—1 month | Juvenile rheumatoid arthritis | Saliva | CORT ↓ |
| Field et al. (1997) ( | 20 females | Massage | 30 min—2/week—1 month | Sexual abuse | Saliva | CORT ↓ but only on the last day |
| Field et al. (1998) ( | 32 children | Massage | 20 min/day—30 days | Asthma | Saliva | CORT ↓ after massage in younger children (4-8 years old) but not older children (9-14 years old) compared to control |
| Field et al. (1998) ( | 28 adults | Massage | 20 min—daily for 1 wk | Burn injuries | Saliva | CORT ↓ |
| Field et al. (1998) ( | 24 female adolescents | Massage | 30 min—2/wk—5 wks | bulimic inpatients | Saliva + Urine | CORT ↓ in massage group but only in urine |
| Field et al. (1998) ( | 10 geriatric | Massage—Swedish | 30 min—3/wk—3 wks | Healthy | Saliva + Urine | CORT ↓ but only long term (urine) |
| Garner et al. (2008) ( | 32 young adults | Massage | 20 min—daily—7 wks | Psychiatric young adults | Saliva | CORT ↓ |
| Hart et al. (2001) ( | 19 females | Massage | 30 min—2/wk—5 wks | Anorexia | Saliva + Urine | CORT ↓ |
| Hernandez-Reif et al. (2000) ( | 30 adults | Massage | 30 min- 2/wk—5 wks | High BP | Saliva + Urine | CORT ↓ |
| Hodgson and Lafferty (2012) ( | 18 geriatric | Massage—Swedish | 20 min—1 session | Cancer | Saliva | CORT ↓ |
| Ironson et al. (1996) ( | 29 gay males | Massage | 45 min—5/wk—4 wks | HIV+, HIV- | Saliva | CORT ↓ |
| Lawler and Cameron (2006) ( | 47 | Massage | 45 min—1/wk—6 wks | Migraine | Saliva | CORT ↓ |
| Leivadi et al. (1999) ( | 30 females | Massage | 30 min—2/wk—5 wks | Healthy | Saliva | CORT ↓ |
| Maratos et al. (2017) ( | 139 females | Hand massage | 7 min—1 session | Healthy | Saliva | CORT ↓ |
| Padayachy et al. (2010) ( | 30 adult males | Spinal manipulative therapy | Unspecified | Low back pain | Serum | CORT ↓ |
| Pala et al. (2024) ( | 39 youth | Osteopathic sympathetic harmonization | 1 session | Major depressive disorder | Saliva | CORT ↑ at 20 min after intervention |
| Pinar and Afsar (2016) ( | 44 | Massage | 15 min—7/wk—1 wk | Cancer | Plasma | CORT ↓ |
| Plaza-Manzano et al. (2014) ( | 30 adults | Cervical vs thoracic manipulation | 1 session | Healthy | Serum | OXT ↑ |
| Stringer et al. (2008) ( | 39 patients | Massage | 20 min | Chemotherapy | Serum | CORT ↓ |
| Sunshine et al. (1996) ( | 30 adults | Massage | 30 min—2/wk—5 wks | Fibromyalgia | Saliva | CORT ↓ |
| Törnhage et al. (2013) ( | 45 adults | Tactile massage | 52 min (Avg) — 10 sessions over 8 wks | Parkinson's disease | Saliva | CORT ↓ within both groups but N.S. between group |
| Tuchin (1998) ( | 9 | Chiropractic manipulation | 4 treatments over 2 wks | Healthy | Saliva | CORT ↓ but after the exclusion of 1 outlier participant |
| Valencia et al. (2025) ( | 10 medical students | Osteopathic manipulative treatments | 15 min—1/wk—6 wks | Stressed | Saliva | CORT ↓ |
| Valera-Calero et al. (2019) ( | 83 adults | Cervical manipulation vs cervical mobilization | 1 session manipulation/3 min mobilization | Healthy | Saliva | CORT ↑ |
| Wojcik et al. (2022) ( | 57 males | Craniosacral therapy | 20 min—1/wk—5 wks | Healthy | Serum | CORT ↓ |
| Author/s | Sample size | Intervention | Duration | Symptoms | Biological Measures | Outcome |
|---|---|---|---|---|---|---|
| Andersson et al. (2004) ( | 11 females | Tactile massage | 60 min—1/wk—10 wks | Type 2 diabetes | Serum | OXT N.S. but CORT ↓ between week 1 + week 2 |
| Bello et al. (2008) ( | 14 males | Massage | 20 min | Healthy | Serum | OXT N.S. |
| Ditzen et al. (2007) ( | 67 females | Massage | 10 min—1 session | Stressed | Saliva (CORT) + Plasma (OXT) | OXT N.S. but CORT↓ |
| Henricson et al. (2008) ( | 44 adults | Tactile touch | 1 hour—1/day—5 days | ICU patients | Serum | OXT N.S. changes |
| Rapaport et al. (2010) ( | 53 adults | Massage—Swedish | 45 min—1 session | Healthy | Saliva + Serum | Both N.S. |
| Rapaport et al. (2012) ( | 45 young adults | Massage—Swedish | 45 min | Healthy | Saliva + Plasma | Both N.S. |
| Turner et al. (1999) ( | 24 females | Massage—Swedish | 15 min—1 session | Healthy | Plasma | OXT N.S. |
| Wikström et al. (2003) ( | 22 adults | Massage—Swedish | 30 min | Healthy | Plasma | OXT N.S. |
| Author/s | Sample size | Intervention | Duration | Symptoms | Biological Measures | Outcome |
|---|---|---|---|---|---|---|
| Li et al. (2019) ( | 40 adult males | Foot massage | 10 min | Healthy | Plasma | OXT ↑ in both hand-administered ( |
| Lohman et al. (2019) ( | 28 females | Cervical spine manipulation | 1 session | Neck pain | Serum | OXT ↑, CORT N.S. |
| Morhenn et al. (2012) ( | 95 adults | Massage | 15 min—1 session | Healthy | Serum | OXT ↑ |
| Plaza-Manzano et al. (2014) ( | 30 adults | Cervical vs thoracic manipulation | 1 session | Healthy | Serum | OXT ↑, |
| Tsuji et al. (2015 | 7 children | Massage—touch therapy | 20 min/day—3 months | Autistic | Saliva | OXT ↑ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine regulation and behavior · Pediatric Pain Management Techniques · Stress Responses and Cortisol
Introduction
1
Manual therapy (MT) is a commonly used non-pharmacological passive intervention applied by clinicians and therapists to relieve musculoskeletal pain, restore optimal movement and physiological function in targeted musculoskeletal tissues (1). The American College of Physicians along with several other clinical practice guidelines recommend nonpharmacological MT as a conservative first line of treatment for musculoskeletal pain (2–4). Common MT techniques include massage, joint or spinal mobilization/manipulation, and myofascial release. Beyond its biomechanical and soft tissue effects, MT has been long argued to modulate certain hormones and neuropeptides (e.g., cortisol, oxytocin, etc.) as well as other neuroimmune signaling pathways, including inflammatory mediators and cytokines due to the inherent nature of mechanical touch involved, the resultant soft tissue relaxation, and musculoskeletal pain reduction associated with MT treatment (5–8).
Within the MT literature, neuroendocrine-related outcomes have often focused on cortisol (CORT) and/or oxytocin (OXT); albeit oxytocin has been examined much less despite being closely associated with touch-based interventions. However, the high heterogeneity in MT study design, biological sampling methods, MT treatment parameters, and timing of neuroendocrine physiological release/response and outcome measurement have resulted in mixed findings with the inability to draw definitive conclusions regarding potential mechanistic roles or neuroendocrine-related contributions to clinical efficacy of MT. Therefore, a scoping review approach which aims to describe the extent and characteristics of the available CORT/OXT evidence and identify gaps in knowledge is warranted to serve as an update of evidence existing within the MT literature and a resource for future MT-related neuroendocrine investigations with goals of achieving more definitive conclusions as to potential neuroendocrine-related mechanisms involved in MT.
CORT is an end product of the hypothalamic-pituitary-adrenal axis (HPA-axis) that is involved in regulating the stress response and is an essential mediator between psychological states and health-related outcomes (9). Increased stress and disrupted sleep patterns have been implicated in driving systemic inflammation via upregulating the sympathetic nervous system and HPA-axis activity (i.e., disrupting cortisol levels and receptor sensitivity) which carries the potential of sensitizing peripheral and central neurons resulting in hyperalgesia (10, 11). The relationship between acute and/or chronic pain and dysregulation of the HPA-axis has been well documented in the literature (12–15). CORT plays a critical role in analgesia as it is released during the initial stages of the stress response and functions to suppress inflammation, edema, and reduce pain. More specifically, it decreases local edema and discomfort by inhibiting the early stages of the inflammatory cascade (16). Therefore, any MT interventions that act to reduce stress and/or systemic inflammation biomarkers may reflect broader effects of MT on stress regulation and/or peripheral/central pain-processing.
Multiple reviews investigating changes of various biomarkers have reported low or moderate quality of evidence that spinal manipulation results in immediate CORT level changes (8, 19, 20). However, it is important to note that a majority of these reviewed CORT studies involved healthy (asymptomatic) participants, studies with small sample sizes, and/or presented high heterogeneity that prevented pooling of the data. In a 2021 systematic review and meta-analysis of neuroimmune responses in animals and humans with neuromuscular conditions (7), three studies (n = 140 patients) assessed the change in CORT in people with neck and/or back pain following joint mobilization/manipulation treatment and reported increased serum CORT in those with acute back pain (17), increased salivary CORT in those with chronic neck pain (18), and no significant CORT changes in individuals with acute neck pain receiving spinal manipulation compared with sham treatment (16). Data from these three studies could not be pooled because of high heterogeneity in methodology and/or MT interventions, yet they provide sufficient motivation to continue a MT-related line of neuroendocrine investigation.
For massage, a 2011 comprehensive quantitative review of 18 articles (704 individuals) pertaining to massage therapy effects on CORT levels (blood, saliva, urine) reported that massage effects on CORT levels were indeed very small and nonsignificant in the vast majority of studies with a lone exception being a multiple dose effect in children (19). The authors of this review noted at the time that their findings refuted the common assertion that massage significantly reduces cortisol, but they were quick to note that these review findings did not negate massage's sizable and proven reductions of trait anxiety, depression, and certain types of pain, but that mechanisms other than CORT were most likely responsible (19). Despite the findings of this older review, three narrative reviews on massage (19–21), mentioned changes in CORT as a potential physiological mechanism of massage therapy and several recent investigations into changes in CORT levels related to MT interventions reported positive findings warranting further investigation.
In addition to CORT, OXT is a neuropeptide that functions both as a neurotransmitter within the brain and as a hormone released into the bloodstream from the posterior pituitary (neurohypophysis) (22, 23). OXT is synthesized primarily in magnocellular neurons of the bilateral supraoptic (SON) and paraventricular nuclei (PVN) of the hypothalamus and is released into the bloodstream via the posterior pituitary. Of note, both OXT and corticotropin-releasing hormone are produced in the PVN, where reciprocal interactions allow OXT signaling to influence stress-related HPA-axis activity, including attenuation of CORT release under certain conditions (24). OXT also interacts with many other neuropeptides including but not limited to angiotension IV, cholecystokinin octapeptide, opiods, orexin, and leptin, as well as other neurotransmitters such as serotonin and dopamine (24). While OXT primary effects are mediated in the brain, parvocellular OXT neurons of the PVN project extensively toward the brainstem and spinal cord where they form synaptic contacts with neurons involved in autonomic function, pain and analgesia (25, 26). Inhibition of paravocellular OXT neurons in the PVN projecting toward the spinal cord decreased pain thresholds thus increasing pain sensitivity, while activation of these neurons repressed nociception and promoted analgesia. Among peripheral organs with OXT receptor expression and binding are the renal cortex, heart, nociceptive dorsal root ganglion (DRG) neurons, adipocytes and adrenal medulla cells (24). The expression of OXT and its receptor has also been demonstrated in fibroblasts and keratinocytes of human skin (27). It is the nociceptive DRG, connective tissue, and skin-related expression that is of particular interest in potential OXT mechanisms related to MT interventions as evidence for OXT's role in peripheral inflammatory processes is increasing. Among its centrally-mediated behavioral and physiological effects, OXT is released during labor, breastfeeding, sexual activity, physical touch, maternal interaction and bonding, as well as during social interactions (anxiety, trust, sociability) between adults and/or animals (24, 28, 29); but it also serves as a neuromodulator with anxiolytic and analgesic properties (30, 31). OXT release has been associated with cutaneous stimulation such as gentle touch, stroking, massage, and exposure to warmth (32, 33). Given its established involvement in touch-mediated and affiliative processes, MT has been hypothesized to influence OXT release through sustained physical contact and related sensory input inherent to MT-related interventions. However, compared to CORT, substantially fewer MT studies have examined OXT responses, and existing findings remain very limited and mixed thereby warranting additional investigation.
While the purpose of this MT-related scoping review is not to provide a theoretical or physiological mechanistic explanation, broader physiological evidence supports the plausibility of neuroendocrine involvement in clinical MT responses. Various techniques of MT have been shown to influence autonomic nervous system activity, inflammatory mediators, and neuroimmune signaling pathways, all of which are closely linked to regulation of the HPA-axis and OXT signaling (5, 7, 8, 34). Within this broader physiological context, CORT and OXT are integrative neuroendocrine mediators that are influenced by autonomic nervous system activity, inflammatory processes, and neuroimmune signaling pathways involved in stress regulation and pain modulation. Framing these hormones within the established manual therapy evidence base therefore provides a clearer physiological context for their continued investigation to arrive at definitive conclusions. Differences in MT intervention type, treatment duration, study population, sampling methods and varied timing of hormone measurement have resulted in substantial heterogeneity across studies. This high variability across different MT techniques complicates interpretation of findings across studies highlighting the need to better describe, characterize and standardize how the data is collected, where research activity is concentrated, and where neuroendocrine MT-related gaps remain. A strength of this scoping review is to focus on three distinct techniques of MT and not just one MT approach (35–38) to provide a more complete picture of MT-related CORT and OXT studies and evidence.
Methods
2
Design
2.1
This scoping review was performed following the framework and guidelines of Arksey and O'Malley, with reporting guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews, along with more contemporary methodological guidance by Mak and Thomas and the Joanna Briggs Institute Scoping Reviews Methodology Group (36, 38–41). The review process followed the core stages outlined in the Arksey and O'Malley and others, including identification of the research question, identification and selection of relevant studies, data charting, and collation and synthesis of findings (35, 36, 39, 42). MT interventions were defined according to Bearne and Hurley as “a skilled application of passive movement to a joint [and/or muscles] either within (‘mobilization’) or beyond its active range of movement (‘manipulation’)” (43), allowing inclusion of diverse techniques such as spinal manipulation, massage, Anma massage, rib raising, suboccipital fascial release, among others.
Search strategy
2.2
A reproducible search strategy was developed from inception through July 2025, in collaboration with a research librarian (RB), and was applied across five databases: PubMed, CINAHL, Embase, Scopus, and Web of Science. These databases were selected to provide broad coverage of biomedical and rehabilitation literature most relevant to MT interventions and physiological outcome measures. While changes in CORT and OXT are often examined within psychological and behavioral research, studies directly investigating MT as a clinical intervention are rarely indexed in these databases; therefore psychological databases such as PsycINFO were not included in this review. Keywords and indexing terms related to CORT and OXT responses, MT interventions, and human subjects were used (see Supplementary Appendix 1). Search results were managed using EndNote 21 and Covidence, with duplicates removed, and the study selection was documented using a PRISMA flow diagram (Figure 1). A review protocol was created through Open Science Framework. In line with several current scoping review recommendations, decisions about the search strategy were shaped by feasibility and focused on peer-reviewed studies to map the published MT evidence base, rather than to comprehensively attempt to capture all possible sources (i.e., grey literature).
The PRISMA flow chart outlining the study selection process.
Inclusion criteria
2.3
Peer-reviewed studies were included if they were published in English, involved non-cadaveric human subjects, reported original data, implemented MT or simulated MT interventions (e.g., massage, osteopathic manipulative treatment, manipulation), and reported at least one physiological outcome related to CORT and/or OXT. Case reports and small case series were also included if they met these criteria. These criteria were applied to facilitate consistent extraction of study characteristics within the scope of this review.
Exclusion criteria
2.4
Studies were excluded if they were categorized at practice guidelines, unpublished manuscripts, dissertations, reviews, expert commentaries, books or book chapters, government reports, or conference proceedings. Additional exclusions included studies relating to pregnancy, lactation, newborn/infants, as well as those involving combination treatments where MT was delivered in combination with another therapeutic intervention. However, if studies with multiple interventions had a group receiving only MT, then the results pertaining to this particular subgroup were included in the review.
Screening procedure
2.5
A two-phase screening process was conducted. Phase I involved title and abstract screening to remove irrelevant studies. Phase II involved full-text screening to assess eligibility. Both phases were performed independently by two reviewers (ATC, MSA), with disagreements resolved by a third reviewer (WRR).
Data extraction
2.6
The following data were extracted from each eligible study: author(s), year of publication, study purpose, keywords, language, population, type of MT or simulated MT, intervention parameters, and primary physiological outcomes. Data extraction parameters were defined a priori by two authors (ATC, MSA). Extraction was conducted by one author (ATC) and verified by a second (WRR) to minimize error.
Data synthesis
2.7
Findings were summarized descriptively according to several domains. Numerical mapping was used to summarize the total number of included studies, examine trends by year of publication, and describe the distribution of evidence according to hormone measured and choice of biological sampling, MT intervention type, and population characteristics. Intervention-level summaries captured reported delivery parameters and associated physiological responses within each MT approach. Consistent with scoping review methodology, formal appraisal of study quality or risk of bias was not conducted. The scoping review optional consultation stage to generate practice recommendations or stakeholder consensus as described by Arksey and O'Malley and/or others was not undertaken for this review.
Results
3
Cortisol—thrust manipulation
3.1
Manual therapy studies demonstrating non-significant and significant changes in cortisol post-intervention are shown in Tables 1, 2. The following text summarizes key studies and significant findings. Valera-Calero et al., compared the effects of cervical manipulation (n = 28), cervical mobilization (n = 28), and cervical sham treatment (n = 27) on saliva cortisol (sCORT) levels in 83 adults with chronic mechanical neck pain. sCORT was assessed at baseline, immediately after treatment, and at one week follow-up. A significant and comparable increase in sCORT was found immediately after the intervention in both the cervical manipulation and cervical mobilization group. In contrast, a significant decrease was yielded in the sham manipulation group (18). Other studies also report short-term increases in CORT release following spinal manipulation (17).
In contrast to spinal manipulation studies reporting significant changes in CORT post-intervention, several spinal manipulation studies failed to demonstrate CORT changes (16, 48, 71, 104). Lohman et al. investigated serum CORT changes immediately following cervical manipulation on 28 females with non-specific neck pain and reported no significant changes compared to baseline. Similar results of a lack of serum CORT changes were reported following thoracic manipulation of 40 males (20 symptomatic) at 5- or 30-minutes post-manipulation (48). In addition, no sCORT changes were reported in 24 men receiving thoracic manipulation at 5 min, 30 min, and 6 h post-intervention when compared to baseline. Whelan et al. (71) reported significant decreases in sCORT after a single manipulation; however, decreases were present in all three study groups (control, sham-manipulation, manipulation) and were attributed to diurnal rhythms as opposed to the manual therapy intervention itself.
Studies examining CORT responses following thrust spinal manipulation demonstrated variable outcomes across study designs and populations. Reported differences were observed with respect to participant symptomatology, intervention protocols, and the timing and medium of CORT sampling. Collectively, studies of thrust manipulation more frequently report short-term increases in CORT, although findings remain inconsistent across studies that differ in sampling time points, methodologies, and participant populations.
Cortisol—non-thrust MT
3.2
Among non-thrust MT studies in adults, participants that received tactile massages (60 min, 1/week, 10 weeks) and had blood collected before massage treatment, one week after, and 12 weeks after found CORT levels significantly decreased only between pre-intervention and 1 week after the intervention (73). Adib-Hajbaghery et al. compared the differences between massage applied by a nurse specialist versus a patient's relative on serum CORT levels. Participants were all male hospital patients and were split into three groups: massage by nurse, massage by patient's relative, and control (routine care). Each massage group received a single session 60 min massage. Serum CORT levels significantly decreased only when the massage was administered by a nurse specialist (72). Leivadi et al. examined the effects of 30 min massages (2x/week for 5 weeks) on sCORT in 30 female dancers with sCORT significantly decreasing between pre and post intervention on both first and last day with the control group not reporting any significant changes (93). Other massage studies reporting decreases in sCORT include studies: in individuals with migraine (92), in psychiatric inpatient adults (87), cancer patients (90), healthy adults (6), females (94), in gay men (91), couples (76), companions of individuals in a coronary care unit (44), individuals undergoing chemotherapy (98), caregivers of cancer patients (96), juveniles with mild-to-moderate rheumatoid arthritis (81), in retired volunteers delivering Swedish massage to infants (86), in bulimic, inpatient females (85), in burn patients (84), in suboccipital release (68), craniosacral therapy (103), in medical students (102), in individuals with post-concussion symptoms (78), in sexually abused women (82), in diabetic women (105), in children psychiatric patients (79), in children with asthma (83), and in individuals post-operatively [(75), (Table 2)]. It is noteworthy that in healthy males receiving either upper or lower cervical mobilization, that a significant reduction of sCORT was reported 30 min only after the lower cervical mobilization for both within and between groups, suggesting anatomical location of mobilization may perhaps influence sCORT response (77). In a study of similar design by the same investigators in people with post-concussion symptoms receiving either upper or lower cervical mobilization, only lower cervical mobilization resulted in a significant within group reduction (5 min before compared to 30 min after intervention) in sCORT, however no significant between group differences were found at post 5 or 30 min (78).
It is also noteworthy that several studies report significant decreases in sCORT in both the intervention and control groups including studies in individuals with Parkinson's disease (100), and in 50-year-old women who received Anma massage from different proficiency level practitioners (50). Significant decreases in sCORT in the intervention and relaxation control groups were similarly reported following a single Thai massage session in 36 self-perceived academically stressed students (46). Participants were randomized into the intervention group (1 session, 5 min, n = 15) or control (laid down). sCORT was analyzed with the first five minutes preceding the intervention and during the first 5 min immediately after the intervention and yielded significant decreases in both groups (68).
Similar to studies involving spinal manipulation, many massage studies also reported a lack of significant changes in CORT post-intervention. Studies reporting a lack of CORT changes following massage included: adolescents in intensive care (59), children undergoing chemotherapy (65), adult cancer survivors (52), healthy adults (57, 61, 63, 66), adults with chronic muscle stiffness following Japanese massage (50), individuals post-exercise (45), individuals with fibromyalgia (49, 99), dementia (67), hypertension (89), women with anorexia nervosa (88), individuals post-op (60, 62, 69), and one study reported CORT increases in the control group but not in the hand massage group (58).
Among studies investigating changes in urinary cortisol (uCORT) levels following massage, Field et al. compared the effects of massage and relaxation on uCORT and sCORT levels in depressed adolescent mothers. Participants either received a 30-min massage intervention (2x/week, 5weeks) or participated in relaxation techniques (15-min yoga and 15-min breathing exercises, 2x/week, 5 weeks). Saliva was collected 30 min before the session, immediately after, and 30 min after the session on the first and last day of intervention. Urine was collected immediately after the intervention on the first and last day. uCORT yielded significant decreases on both first and last day and sCORT levels also significantly decreased between the first and last day. The relaxation control group did not yield any significant changes (80). Hernandez-Reif et al. (55) examined the effects of massage therapy on uCORT and sCORT in 30 adults with hypertension. sCORT was assessed before and 20 min after the intervention on the first and last day, and uCORT was assessed before the intervention on the first and last day. Compared to the control group, only the massage group showed significant decreases in both uCORT and sCORT (89). Bost et al. (47) investigated the effectiveness of Swedish massage in reducing physiological and psychological stress indicators in 60 nurses at an acute care hospital. Nurses received back massages (15 min, 1x/week, 5/weeks) with urine samples collected in the morning during the 1st, 3rd, and 5th weeks. No significant changes in uCORT levels occurred between week one and five in the massage group compared to control (47). Several other massage studies also reported no changes in uCORT levels including in a diabetic population (70), individuals with low back pain (54), Parkinson's disease (55), women with anorexia nervosa (88), and early-stage breast cancer (56).
Studies examining CORT responses following non-thrust MT reported heterogeneous outcomes across intervention types and study populations. In contrast to thrust manipulation, non-thrust MT approaches (particularly massage-based interventions), more frequently reported decreases in CORT. However, these effects were observed across diverse populations and study protocols, limiting comparability.
Oxytocin
3.3
Compared to CORT, fewer studies have investigated the effects of MT on OXT levels (Tables 3, 4). Morhenn et al. examined the effects of a single Swedish massage on OXT levels in 95 healthy adults. Participants were split into the massage group (n = 65, 1 session, 15 min) or control (n = 30, rest). Serum OXT was assessed immediately before (n = 95), with a subset (n = 24) having it assessed immediately after the massage session. The remaining participants in the massage group (n = 41) had their serum assessed after completing an economic task. This study design was implemented to ensure OXT levels were not being influenced from monetary gain. The massage group yielded a significant increase in serum OXT levels (33). Tsuji et al., examined the effects of massage on salivary OXT levels in mothers and children after massage. Children were massaged by their mothers for 20 min/day, every day, for 3 months. After the massage phase, they then had a 4-month phase of no massage for 4 months. Salivary OXT assessments were made before and 20 min after the intervention every 3 weeks during the massage phase and every 4 weeks during the no-massage phase. During the massage phase, salivary OXT levels were significantly higher (but only when averaging basal OXT levels throughout the entire phase), compared to the no massage phase. Significant increases were not found after a single intervention, suggesting an accumulation effect with OXT (111). In another interesting study comparing hand-delivered versus machine-delivered 10-min foot massages, both resulted in significantly increased plasma OXT levels immediately post-intervention, but more potent OXT changes (51.8% vs 18.2%) were reported after hand massage, which was deemed more pleasurable and rewarding (110). Hand massage also demonstrated greater cortical activation of regions processing reward aspects of social touch than machine-delivered massage as accessed using functional near infrared spectroscopy (110).
Wikstrom et al., examined the effects of Swedish massage on plasma OXT in 22 healthy adults. Participants were given a single session of a Swedish massage (30 min) and had serum OXT assessed immediately before, after 60 min after the intervention. Serum OXT yielded no significant differences, although they did note that OXT were varied widely between men and women at baseline (109). In a randomized controlled trial, Henricson et al., examined the effects of five-day tactile touch intervention on serum OXT in 44 adults in the intensive care unit. Participants were split into either the tactile touch group (1 h/day, 5 days) or control (standard care). Serum oxytocin was collected before (noon) and after the intervention and standard treatment (1pm). Serum OXT levels did not significantly change in the touch group; in contrast, the standard care group saw a significant increase (107). Other studies also reported a lack of OXT changes following massage (76).
Studies measuring both cortisol and oxytocin
3.4
A small subset of studies assessed both CORT and OXT responses following MT interventions. Plaza-Manzano et al. examined the effects of cervical and thoracic spinal manipulation in asymptomatic adults and reported significant increases in OXT immediately following both interventions, with sustained elevations at two hours in the cervical manipulation. In contrast, CORT levels demonstrated a transient increase immediately post-manipulation followed by a significant decrease at two hours in the cervical manipulation group (97). Rapaport et al. compared the effects of a single session of Swedish massage to a light touch control in healthy adults and assessed both plasma and salivary CORT along with plasma OXT at multiple time points post-intervention (6, 66). No significant changes were observed in either CORT or OXT following massage compared to control (66). Lohman et al. reported increases in OXT following cervical manipulation, but no changes in CORT (16). Two studies reported a significant decrease in CORT while yielding no significant changes in OXT (73, 76).
Discussion
4
Consistent with the Arksey and O'Malley framework (39) and subsequent refinements described by others (35, 36, 41), this scoping review mapped the existing literature examining CORT and OXT responses following three distinct MT treatment approaches (spinal manipulation, joint mobilization, massage). A key strength of this review is its inclusion of multiple MT modalities rather than focusing on a single MT intervention type. Collectively, this review highlights the substantial variability in reported MT-related hormone/neuropeptide responses, underscoring the future importance of MT standardization, addressing knowledge gaps, and resolving methodological challenges noted within the existing evidence base.
Key patterns and evidence gaps in neuroendocrine responses to MT
4.1
Despite MT having been long proposed to influence CORT and OXT through inherent physical touch, resultant muscle relaxation and/or stress reduction; when the evidence is examined collectively, findings across MT studies remain mixed and highly variable. Among investigations assessing CORT, approximately half reported significant changes, while the remainder reported either no significant effects or similar changes occurring in both the intervention and control groups. Notable, studies involving thrust manipulation more often reported short-term increases in CORT, whereas non-thrust MT approaches more frequently demonstrated decreases in CORT across diverse study populations. These differences in the direction of CORT responses by different MT techniques suggest that distinct physiological processes may be engaged which warrants further investigation.
Many of the CORT studies focused on Swedish massage; a technique primarily aimed at promoting relaxation and relieving tension. This modality typically involves long, gliding strokes, kneading, and friction to warm the muscles, enhance circulation, and reduce physical stress (47, 112). If a study broadly referred to the intervention as “massage” or “standard massage” without specifying the technique, it was assumed to be Swedish. Totaling 35 of the studies, 20 of them yielded significant changes in CORT levels between pre- and post- intervention. Notable variation exists across these studies, particularly in terms of massage duration, which ranged from 10 to 90 min, and in treatment frequency, which spanned from a single session to multiple sessions per week over a 12-week period (46, 63, 113). Forty-seven percent of the CORT massage studies performed massage 16-30 min, while 33% performed massage 31-60 min. To our knowledge comparisons of CORT changes based on massage duration has not been performed. While there are far fewer OXT studies (Figure 2), they are more evenly distributed across massage durations. Figure 2 provides a visual representation of the number of CORT and OXT studies performed, and the type of biological sampling involved. The overall lack of OXT MT-related studies is clearly apparent as is the dominance of saliva sampling of neuroendocrine changes (Figure 2). Additionally, the health status and age of the participants varied considerably among CORT and OXT studies, with studies including healthy individuals as well as those with psychiatric conditions, chronic pain, cancer, and other clinical populations. However, neither treatment frequency, age, nor participant health condition appeared to consistently influence whether significant changes were reported for either CORT or OXT levels.
Illustration of the type and proportion of manual therapy intervention studies along with the biological sampling methodology of the specific neuroendocrine hormones.
The second most common intervention among the CORT studies was spinal manipulation. Within this MT subset, four studies reported either no significant changes or non-specific results. These study findings also remain inconclusive, and the type of manipulation (i.e., cervical versus thoracic) did not appear to likely influence the likelihood of yielding significant changes. Notably, Plaza-Manzano et al. (97) and Lohman et al. (16) are the only studies to date that examined the effects on both CORT and OXT levels. Both studies reported an increase in OXT but differing results for CORT.
In contrast to CORT studies, substantially fewer studies examined OXT responses following MT with 65 assessing CORT outcomes, 13 assessing OXT, and 6 measuring both hormones. Approximately two-thirds of OXT studies were conducted in healthy participants, while the remainder included symptomatic populations, with no consistent pattern of OXT response observed by participant health status. Similar to CORT, a near equal division of MT findings measuring OXT changes was also found with 5 studies reporting significant changes, while 8 studies reported a lack of significant OXT changes with MT. Both CORT and OXT studies demonstrated large variability in reported findings. This is most likely the result of the lack of standardization regarding the MT application, differences in MT applied forces and MT treatment durations, small sample sizes, and differing methodologies used to sample and process CORT and OXT in the same bodily fluids. Much greater consideration needs to be given to conducting CORT and OXT studies in symptomatic populations (acute and chronic musculoskeletal conditions), since a large number of neuroendocrine MT-related studies were performed in healthy populations. However, with that said neither treatment frequency, participant age, nor participant health condition appeared to consistently influence whether a study reported significant changes in CORT levels following an MT intervention. Studies attempting to compare CORT or OXT changes between distinct MT techniques were practically non-existent. Similarly severe lack of longitudinal CORT and OXT MT-related studies creates a large gap in knowledge, however longitudinal MT studies are extremely difficult to control due to complex neuroendocrine interactions, differences in neuroendocrine production, storage, release, and half-life of these hormones/neuropeptides.
Similar to the CORT studies, most OXT studies involved massage, and findings were mixed. Approximately one-third of the studies reported significant changes in OXT levels, while the remaining studies either found no significant changes or observed similar changes in both the intervention and control groups. The five studies that did not report significant effects involved massage and/or touch therapy; however, only studies that incorporated spinal manipulation yielded significant increases in OXT levels. Details such as treatment frequency, participant age, and health condition did not appear to consistently influence whether a study reported significant changes in OXT levels.
To address gaps in knowledge pertaining to CORT and OXT-related MT research, future research should prioritize the development of standardized protocols for MT interventions, including clearly defined MT techniques, treatment durations, and treatment frequencies, to improve consistency across studies. Efforts should also be made to increase sample size and include more diverse populations, as most existing research focuses on small, homogenous samples. As shown in Figure 3A, a majority of CORT and OXT studies were conducted with relatively small sample sizes (<50) which limits statistical power and reduces the likelihood of detecting significant effects. Figure 3B demonstrates a growing interest in hormonal-related manual therapy studies over the last four decades. Ultimately, increasing sample size, advancing methodological rigor and sample collection standardization will be key to identifying potential MT-related neuroendocrine mechanisms and clinical relevance of MT in modulating stress- and pain- related physiology.
Summaries of the included studies by (A) sample size and (B) chronological decade with the corresponding number of studies.
Methodological boundaries and sources of heterogeneity
4.2
Several important gaps in the literature limit the strength and generalizability of the current MT evidence on CORT/OXT levels. Most MT studies relied on single-session interventions with immediate or short-term follow-up, limiting assessment of delayed or sustained hormonal responses. Variability in the timing and duration of MT administration and biological sample collection further contributed to heterogeneity across studies. While some investigators reported time-of-day and sampling schedules to account for known diurnal variations in CORT, others did not, reducing comparability. Across studies, post-intervention sample collections were variable with 20 min after MT being the most common. Few studies incorporated repeated or longitudinal sampling (6, 67, 73). In addition, one must also remain mindful that OXT is stored in secretory vesicles both within hypothalamic neurons and at axon terminals in the neurohypophysis, allowing for rapid release from pre-existing pools in response to stimulation. While axonal transport contributes to replenishment of these stores, the timing of peripheral oxytocin release following mechanical or sensory stimulation is also variable (31, 114, 115). Interpretation of OXT findings is further complicated by its role as a centrally acting neuropeptide and neurotransmitter, such that peripheral measures may not consistently reflect central activity, as well as by bidirectional interactions between OXT and the HPA-axis (116–118). Support for this concept comes from basic studies, where gentle touch or massage-like stimulation has been shown to activate central OXT signaling and attenuate HPA-axis activity, with effects that depend on the timing and nature of the mechanical stimulation (119–122).
Limitations
4.3
Limitations of this review include the exclusion of non-English studies and those examining OXT/CORT in the context of pregnancy, labor, lactation and infancy. The latter decision was made because OXT plays a distinct physiological role in reproductive processes, and including such studies could have only confounded the interpretation of findings related to MT interventions (123). In addition, the inclusion of only peer-reviewed clinical literature may have excluded certain grey literature, which could potentially further inform the hormonal/neuropeptide scope of MT research. Future reviews may also wish to increase the number of databases searched such as PsycINFO to ensure capture of psychological and behaviorally-related studies. The amount of CORT and OXT-related knowledge and insight to be gained from animal studies is large and is deserving of its own review.
Conclusions
5
This scoping review mapped the existing literature examining CORT and OXT responses following MT to characterize the scope and nature of the available evidence. While CORT has been examined across a range of MT approaches with mixed results, the evidence base for OXT remains severely limited. Both CORT and OXT MT-related studies demonstrated substantial variability in intervention type, study population, and sample collection/processing, and outcome assessment. This review also helps to identify the extent and shortcomings of MT-related neuroendocrine research and identifies areas where further investigation is needed, particularly with respect to OXT-related studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bishop MD Torres-Cueco R Gay CW Lluch-Girbés E Beneciuk JM Bialosky JE. What effect can manual therapy have on a patient’s pain experience? Pain Manag. (2015) 5(6):455–64. 10.2217/pmt.15.3926401979 PMC 4976880 · doi ↗ · pubmed ↗
- 2Qaseem A Wilt TJ Mc Lean RM Forciea MA Denberg TD Barry MJ Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med. (2017) 166(7):514–30. 10.7326/M 16-236728192789 · doi ↗ · pubmed ↗
- 3Blanpied PR Gross AR Elliott JM Devaney LL Clewley D Walton DM Neck pain: revision 2017. J Orthop Sports Phys Ther. (2017) 47(7):A 1–83. 10.2519/jospt.2017.030228666405 · doi ↗ · pubmed ↗
- 4Zhou T Salman D Mc Gregor AH. Recent clinical practice guidelines for the management of low back pain: a global comparison. BMC Musculoskelet Disord. (2024) 25(1):344. 10.1186/s 12891-024-07468-038693474 PMC 11061926 · doi ↗ · pubmed ↗
- 5Kovanur Sampath K Tumilty S Wooten L Belcher S Farrell G Gisselman AS. Effectiveness of spinal manipulation in influencing the autonomic nervous system—a systematic review and meta-analysis. J Man Manip Ther. (2024) 32(1):10–27. 10.1080/10669817.2023.228519638044657 PMC 10795624 · doi ↗ · pubmed ↗
- 6Rapaport MH Schettler P Bresee C. A preliminary study of the effects of repeated massage on hypothalamic-pituitary-adrenal and immune function in healthy individuals: a study of mechanisms of action and dosage. J Altern Complement Med. (2012) 18(8):789–97. 10.1089/acm.2011.007122775448 PMC 3419840 · doi ↗ · pubmed ↗
- 7Lutke Schipholt IJ Coppieters MW Meijer OG Tompra N de Vries RBM Scholten-Peeters GGM. Effects of joint and nerve mobilisation on neuroimmune responses in animals and humans with neuromusculoskeletal conditions: a systematic review and meta-analysis. Pain Rep. (2021) 6(2):e 927. 10.1097/PR 9.000000000000092734104836 PMC 8177878 · doi ↗ · pubmed ↗
- 8Valencia P He LM Wippert Y MP. The changes of blood-based inflammatory biomarkers after non-pharmacologic interventions for chronic low back pain: a systematic review. BMC Musculoskelet Disord. (2024) 25(1):209. 10.1186/s 12891-024-07289-138459458 PMC 10921684 · doi ↗ · pubmed ↗