Evolving Inguinal Hernia Repair Practice at the Veterans Health Administration
Emma M. Bradley, Kathryn A. Schlosser, Michael E. Matheny, Richard A. Pierce

TL;DR
This study tracks how inguinal hernia repair procedures and techniques have changed among US veterans over 20 years, showing increased use of minimally invasive surgery.
Contribution
The study provides the first comprehensive analysis of inguinal hernia repair trends in the Veterans Health Administration over two decades.
Findings
Inguinal hernia repair volume increased by nearly 50% from 2002 to 2022 in the VHA.
Minimally invasive surgery use rose from 9% to 41% during the study period.
Female veterans had higher rates of minimally invasive surgery and urgent repairs compared to male veterans.
Abstract
This cohort study examines 20 years of data for US veterans who had inguinal hernia repair to track trends and changes in volume and surgical approach. How have volume and surgical approach to inguinal hernia repair (IHR) in veterans changed within the Veterans Health Administration (VHA) over the last 20 years? This cohort study involving 308 876 veterans (2002 to 2022) found that IHR volume increased nearly 50%, with minimally invasive approaches increasing from 9% to 41%. Community-based procedures were more often urgent/emergent, and female veterans had higher rates of minimally invasive surgery and urgent repairs. These results highlight significant growth in IHR volume and a shift toward minimally invasive approaches in the VHA, illustrating evolving technical practice and veterans’ surgical needs, providing data to inform policy and resource allocation. Inguinal hernia repair…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
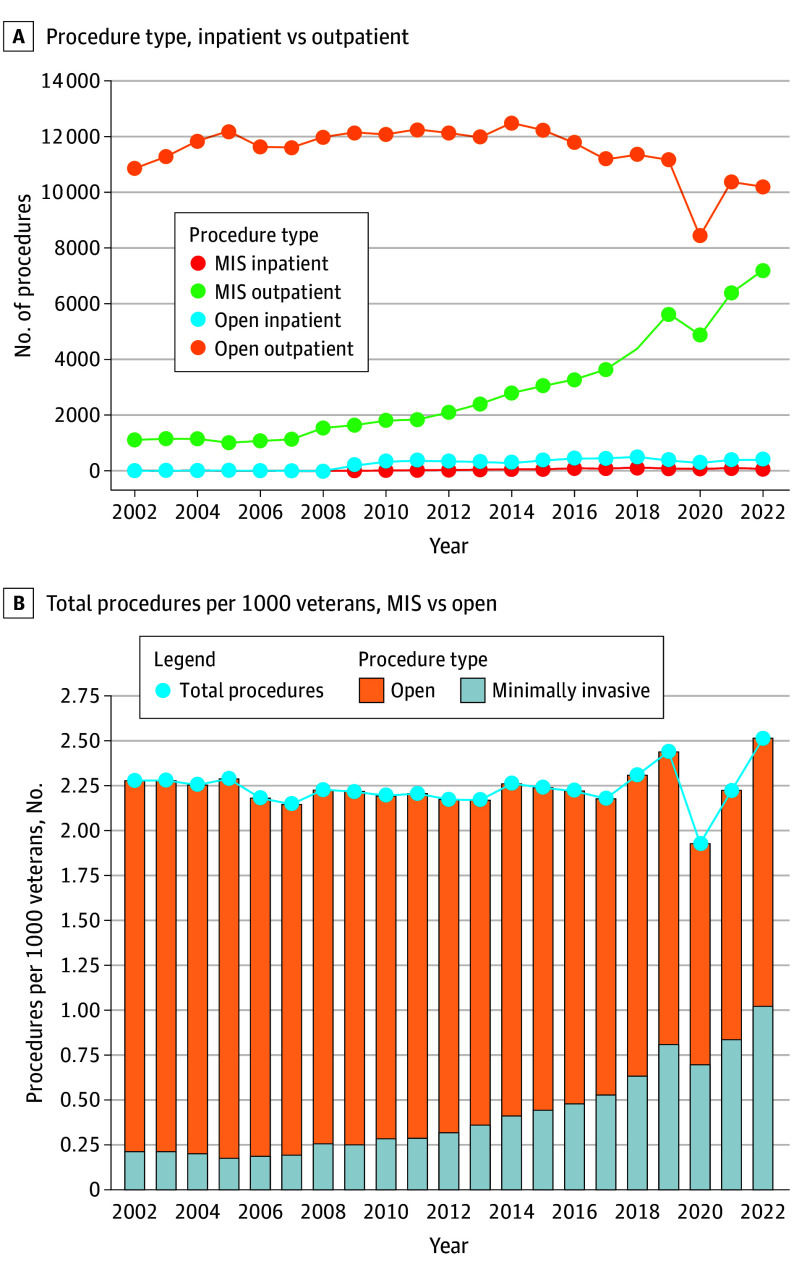 Figure 1
Figure 1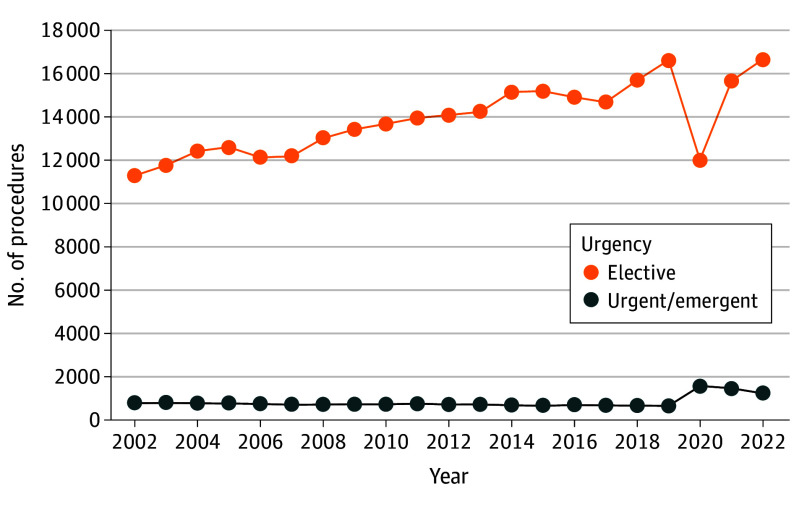 Figure 2
Figure 2| Characteristic | Outpatient (n = 300 375), No. (%) | Inpatient (n = 6116), No. (%) | ||
|---|---|---|---|---|
| MIS (n = 59 134) | Open (n = 241 241) | MIS (n = 954) | Open (n = 5162) | |
| Age, median (IQR), y | 64 (55 to 71) | 65 (57 to 73) | 68 (61 to 75) | 71 (63 to 79) |
| Gender | ||||
| Female | 426 (0.7) | 1407 (0.6) | 26 (2.7) | 72 (1.4) |
| Male | 58 708 (99.3) | 239 834 (99.4) | 928 (97.3) | 5090 (98.6) |
| Race | ||||
| American Indian or Alaska Native | 417 (0.7) | 1299 (0.5) | 5 (0.5) | 28 (0.5) |
| Asian | 206 (0.3) | 678 (0.3) | 4 (0.4) | 15 (0.3) |
| Black or African American | 7537 (12.7) | 36 158 (14.9) | 147 (15.4) | 967 (18.7) |
| Native Hawaiian or Other Pacific Islander | 315 (0.5) | 1500 (0.6) | 6 (0.6) | 38 (0.7) |
| White | 47 071 (79.6) | 185 043 (76.7) | 749 (78.5) | 3800 (73.6) |
| Unknown | 3588 (6.1) | 16 563 (6.9) | 43 (4.5) | 314 (6.1) |
| Elixhauser comorbidity score, median (IQR) | 0 (−5 to 8) | 1 (−2 to 10) | 6 (−2 to 17) | 10 (0 to 24) |
| Selected comorbidities | ||||
| Hypertension | 35 941 (60.8) | 156 298 (64.8) | 713 (74.7) | 4125 (79.9) |
| Diabetes | 10 992 (18.6) | 46 902 (19.4) | 275 (28.8) | 1631 (31.6) |
| HIV | 536 (0.9) | 2051 (0.9) | 9 (0.9) | 44 (0.9) |
| CHF | 3515 (5.9) | 21 336 (8.8) | 146 (15.3) | 1249 (24.2) |
| COPD | 13 235 (22.4) | 66 001 (27.4) | 316 (33.1) | 2104 (40.8) |
| Depression | 22 362 (37.8) | 77 143 (32.0) | 414 (43.4) | 2157 (41.8) |
| Alcohol use disorder | 14 026 (23.7) | 52 082 (21.6) | 247 (25.9) | 1485 (28.8) |
| Drug use disorder | 14 602 (24.7) | 45 103 (18.7) | 276 (28.9) | 1508 (29.2) |
| Region | ||||
| Midwest | 13 925 (23.5) | 51 192 (21.2) | 246 (25.8) | 1114 (21.6) |
| Northeast | 6245 (10.5) | 30 392 (12.6) | 130 (13.6) | 786 (15.2) |
| South | 23 898 (40.4) | 98 973 (41.0) | 325 (34.1) | 1855 (35.9) |
| Unknown | 3 (<0.1) | 4 (<0.1) | 0 | 1 (<0.1) |
| US outlying islands | 471 (0.8) | 3708 (1.5) | 49 (5.1) | 111 (2.2) |
| West | 14 592 (24.7) | 56 972 (23.6) | 204 (21.4) | 1295 (25.1) |
| Urgency | ||||
| Elective | 57 538 (97.3) | 228 064 (94.5) | 696 (73.0) | 2873 (55.7) |
| Urgent/emergent | 1530 (2.6) | 13 068 (5.4) | 257 (26.9) | 2282 (44.2) |
| Setting | ||||
| VAMC facility | 58 883 (99.6) | 240 361 (99.6) | 808 (84.7) | 4213 (81.6) |
| Community care | 251 (0.4) | 880 (0.4) | 146 (15.3) | 949 (18.4) |
| Characteristic | No. (%) | ||
|---|---|---|---|
| Female (n = 1971) | Male (n = 306 905) | ||
| Age, median (IQR), y | 56 (44 to 65) | 65 (57 to 73) | <.001 |
| Race | |||
| American Indian or Alaska Native | 22 (1.1) | 1739 (0.6) | <.001 |
| Asian | 12 (0.6) | 903 (0.3) | |
| Black or African American | 365 (18.5) | 44 861 (14.6) | |
| Native Hawaiian or Other Pacific Islander | 13 (0.7) | 1872 (0.6) | |
| White | 1421 (72) | 236 937 (77.2) | |
| Unknown | 138 (7.0) | 20 593 (6.7) | |
| Elixhauser comorbidity score, median (IQR) | −2 (−5 to 7) | 1 (−3 to 10) | <.001 |
| Selected comorbidities | |||
| Hypertension | 917 (46.5) | 197 875 (64.5) | <.001 |
| Diabetes | 257 (13.0) | 60 137 (19.6) | <.001 |
| HIV | 11 (0.6) | 2654 (0.9) | .14 |
| CHF | 93 (4.7) | 26 603 (8.7) | <.001 |
| COPD | 555 (28.2) | 82 053 (26.7) | .20 |
| Depression | 1097 (55.7) | 101 783 (33.2) | <.001 |
| Alcohol use disorder | 322 (16.3) | 68 105 (22.2) | <.001 |
| Drug use disorder | 399 (20.2) | 61 485 (20.0) | .80 |
| Region | |||
| Midwest | 356 (18.1) | 66 574 (21.7) | <.001 |
| Northeast | 219 (11.1) | 37 661 (12.3) | |
| South | 853 (43.3) | 125 206 (40.8) | |
| Unknown | 1 (<0.1) | 7 (<0.1) | |
| US outlying islands | 10 (0.5) | 4360 (1.4) | |
| West | 532 (27.0) | 73 097 (23.8) | |
| Hospitalization | |||
| Outpatient procedure | 1833 (93.0) | 298 567 (97.3) | <.001 |
| Inpatient procedure | 138 (7.0) | 8338 (2.7) | |
| Procedure type | |||
| Minimally invasive | 452 (22.9) | 59 636 (19.4) | <.001 |
| Open | 1479 (75.0) | 244 924 (79.8) | |
| Urgency | |||
| Elective | 1751 (88.8) | 289 590 (94.3) | <.001 |
| Urgent/emergent | 218 (11.1) | 17 134 (5.6) | |
| Setting | |||
| Community care | 65 (3.3) | 3545 (1.2) | <.001 |
| VAMC facility | 1906 (96.7) | 303 360 (98.8) | |
| Characteristic | Community care (n = 3610) | VAMC (n = 305 266) | |
|---|---|---|---|
| Age, median (IQR), y | 70 (62 to 78) | 65 (57 to 73) | <.001 |
| Gender | |||
| Female | 65 (1.8) | 1906 (0.6) | <.001 |
| Male | 3545 (98) | 303 360 (98.8) | |
| Race | |||
| American Indian or Alaska Native | 24 (0.7) | 1737 (0.6) | <.001 |
| Asian | 22 (0.6) | 893 (0.3) | |
| Black or African American | 510 (14.1) | 44 716 (14.6) | |
| Native Hawaiian or Other Pacific Islander | 47 (1.3) | 1838 (0.6) | |
| White | 2695 (74.7) | 235 663 (76.8) | |
| Unknown | 312 (8.6) | 20 419 (6.7) | |
| Elixhauser comorbidity score, median (IQR) | 10 (−1 to 24) | 1 (−3 to 10) | <.001 |
| Selected comorbidities | |||
| Hypertension | 2764 (76.6) | 196 028 (63.9) | <.001 |
| Diabetes | 1056 (29.3) | 59 338 (19.3) | <.001 |
| HIV | 24 (0.7) | 2641 (0.9) | .20 |
| CHF | 834 (23.1) | 25 862 (8.5) | <.001 |
| COPD | 1401 (38.8) | 81 207 (26.5) | <.001 |
| Depression | 1484 (41.1) | 101 396 (33.0) | <.001 |
| Alcohol use disorder | 1014 (28.1) | 67 413 (22.0) | <.001 |
| Drug use disorder | 1109 (30.7) | 60 775 (19.8) | <.001 |
| Region | |||
| Midwest | 774 (21.4) | 66 156 (21.6) | <.001 |
| Northeast | 414 (11.5) | 37 466 (12.2) | |
| South | 1492 (41.3) | 124 567 (40.6) | |
| Unknown | 8 (0.2) | 0 | |
| US outlying islands | 25 (0.7) | 4345 (1.4) | |
| West | 897 (24.8) | 72 732 (23.7) | |
| Inpatient vs outpatient | |||
| Outpatient | 1132 (31.4) | 299 268 (97.5) | <.001 |
| Inpatient | 2478 (68.6) | 5998 (2.0) | |
| Procedure type | |||
| Minimally invasive | 397 (17.8) | 59 691 (19.6) | .04 |
| Open | 1829 (82.2) | 244 574 (79.7) | |
| Urgency | |||
| Elective | 2412 (66.8) | 288 929 (94.1) | <.001 |
| Urgent/emergent | 1015 (28.1) | 16 337 (5.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Aortic aneurysm repair treatments · Hip and Femur Fractures
Introduction
Hernia repair is one of the most commonly performed general surgery procedures worldwide. In the US, approximately 800 000 inguinal or femoral hernia repairs are conducted annually.^1^ The lifetime risk of inguinal hernia is estimated at 27% to 43% for men and 3% to 6% for women.^2^ Abdominal core disease, which includes both ventral and groin hernias, can lead to both acute and chronic health issues, significantly affecting quality of life.^3^ Management is multidisciplinary and may include surgery, medical therapy, physical rehabilitation, and preventive strategies.^3^ From a public health standpoint, abdominal core health represents a substantial financial burden, with inguinal hernia repair (IHR) accounting for nearly $2.5 billion in annual health care costs in the early 2000s.^1^
Over the past few decades, surgical techniques for IHR have evolved. Various populations undergoing IHR have been studied to generate comparative data on the relative effectiveness of surgical approaches. While initial randomized clinical trial (RCT) results found watchful waiting to be an acceptable approach for men with minimally symptomatic IHR, long-term follow-up has demonstrated that most patients (68.0%) ultimately require surgery because of the progression of symptoms.^4,5^ An RCT from 14 Veterans Affairs Medical Centers (VAMCs) published in 2004 concluded that open IHR was superior to minimally invasive surgery (MIS) for IHR in terms of recurrence and complications in a primarily male population, although MIS was associated with faster recovery.^6^ A follow-up cost-effectiveness study reported higher costs for MIS with no improvement in quality-adjusted life-years.^7^ In contrast, recent civilian studies have demonstrated favorable outcomes after MIS-IHR when compared with open IHR, including less pain; earlier return to work; equivalent postoperative mortality, morbidity, and readmission rates; and lower recurrence rates.^8,9,10^
Despite these advances, little is known about contemporary trends in overall IHR case volume and surgical approach within the Veterans Health Administration (VHA). Most national studies reflect civilian populations, and while the Veterans Affairs Surgical Quality Improvement Program (VASQIP) has examined IHR outcomes by technique, the database does not capture the full scope of IHR volume or care settings across the VHA.^1,11,12,13,14^
Veterans represent a distinct population from civilian patients: typically older, predominantly male, and with higher rates of comorbidities such as obesity, smoking, and diabetes.^9,10,11,12,13,14^ Understanding IHR trends within this group is essential to improving care delivery, informing resource allocation, and guiding public health efforts. This study aims to characterize national trends in IHR within the VHA over the past 2 decades, including procedure volume, approach, urgency, and care setting (VAMC facilities and non-VA community care settings).
Methods
We queried the VA Corporate Data Warehouse (CDW), a national repository of electronic health records for all VAMC facilities, to select all veterans who have undergone IHR from 2002 to 2022. Veterans older than 18 years who underwent open or MIS-IHR were identified based on Current Procedural Terminology (CPT) codes and administrative codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). A crosswalk of all codes used for data acquisition is included in eTable 1 in Supplement 1. As minimally invasive vs open technique is not captured in IHR ICD-9-CM codes, veterans with only ICD-9-CM codes identifying their procedure (without any corresponding CPT codes) were excluded from analyses of surgical approach (2385 patients, 0.77% of the cohort). MIS-IHR included both laparoscopic and robotic hernia repairs. This study was approved by the Tennessee Valley Healthcare System Veteran Affairs Medical Center institutional review board and research and development committees (VA IRBNet No. 321909), with approval for waived informed consent. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Preoperative demographic details and patient characteristics obtained from the CDW for each veteran included age, sex, self-reported race, and comorbidities. The Elixhauser comorbidity score was used as a composite validated weighted index of comorbidities based on ICD-9-CM/ICD-10-CM diagnosis codes.^15^ Details on select comorbidities were obtained, including hypertension, diabetes, human immunodeficiency virus status, congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), depression, and alcohol and drug use disorders. Operative characteristics encompass geographic region, urgency (elective vs urgent/emergent), inpatient vs outpatient setting, and location of service delivery (within a VAMC facility or through community care). Community care procedures include those that were performed outside of VAMC facilities but reimbursed by the VHA, classified using Fee Basis records. Data were incomplete for 48 004 Elixhauser comorbidity scores (15.5%) and 183 surgical urgency classifications (0.06%). Demographic and operative characteristics are represented by frequencies and percentages for categorial variables and median (IQR) for continuous variables.
Primary outcomes included the incidence and trends of open and minimally invasive hernia repairs performed in the inpatient and outpatient settings throughout the study period. We examined patient demographics by procedure type. Demographic characteristics, changes in surgical approach, urgency, and care setting were detailed over time. We report both the absolute number of groin hernia repairs and the IHR rate standardized to the annual population of veterans receiving VHA care, defined as the number of unique individuals with at least 1 VHA visit per year. Additional analyses compared patient and operative characteristics by sex and by site of care (VAMC facility vs community care). To explore changes in VAMC facility vs community care IHR volume and procedure type, we also performed comparisons of procedures performed before and after the passage of the MISSION Act of 2018, which expanded access to community-based care.^16^
χ^2^ Tests were used to compare categorical variables, and Wilcoxon rank sum tests were applied to continuous variables for nonparametric distributions. All data analysis was performed using R Studio version 2023.12.1 + 402 (R Foundation) during the period January to April 2025.
Results
From 2002 to 2022, a total of 308 876 veterans underwent IHR performed through the VHA. On average, throughout the study period, more than 14 700 IHRs of any kind were performed each year. Of these, 60 088 (19.5%) were minimally invasive while 246 403 (79.8%) were open surgeries, with 2385 (0.8%) unknown because of ICD-9-CM coding alone. Among MIS procedures, 49 802 (82.9%) were laparoscopic and 10 286 (17.1%) robotic. Most of these operations were performed on an elective basis (291 341 [94.4%]), while 17 352 (5.6%) took place in urgent or emergent settings. IHRs were predominantly outpatient procedures (300 400 [97.3%]) vs inpatient procedures (8476 [2.7%]). The median (IQR) age of the cohort was 65 (57-73) years, and the majority of veterans were male (306 905 [99.4%] vs 1971 female veterans [0.6%]) and White (238 358 [77.2%] compared with 1761 [0.6%] American Indian or Alaska Native, 915 [0.3%] Asian, 45 226 [14.6%] Black or African American, and 1885 [0.6%] Native Hawaiian or Other Pacific Islander veterans and 20 731 [6.7%] with unknown race). Veterans had high rates of hypertension (198 792 [64.4%]), depression (102 880 [33.3%]), COPD (82 608 [26.7%]), and alcohol use disorder (68 427 [22.2%]). The highest proportion of IHR were performed in the South (126 059 [40.8%]), followed by the West (73 629 [23.8%]) and Midwest (66 930 [21.7%]).
Demographic characteristics for veterans who underwent MIS vs open IHR in the inpatient vs outpatient settings are detailed in Table 1. Patients who underwent inpatient IHR tended to be older (median [IQR] age, 69 [62-78] years vs 65 [57-73] years; P < .001) and have higher Elixhauser comorbidity scores (median [IQR] score, 8 [−2 to 22] vs 1 [−4 to 10]; P < .001). The most common procedure performed was the outpatient open IHR (241 241 [78.7%]), followed by MIS outpatient surgery (59 134 [19.3%]). In the urgent/emergent setting, only 1787 IHRs (10.0%) were performed MIS vs 58 234 elective procedures (20.0%). Veterans requiring urgent/emergent IHR were more likely to have comorbidities, including diabetes (4420 [25.5%] vs 55 933 [19.2%]; P < .001), CHF (3085 [17.8%] vs 23 584 [8.1%]; P < .001), and COPD (5874 [33.8%] vs 76 690 [26.3%]; P < .001). Most IHRs performed at VAMC facilities were open outpatient (240 361 [78.9%]) or MIS outpatient (58 883 [19.3%]), while most IHRs through community care were open inpatient (949 [42.6%]) or open outpatient (880 [39.5%]) procedures.
Patient and operative characteristics were stratified by sex (Table 2). Female veterans were more likely to undergo IHR on an inpatient basis (138 [7.0%] vs 8338 male veterans [2.7%]) and more likely to undergo surgery in the community (65 [3.3%] vs 3545 male veterans [1.2%]). Women undergoing IHR had nearly double the incidence of requiring urgent/emergent intervention (218 [11.1%] vs 17 134 male veterans [5.6%]; P < .001). Women were slightly more likely to undergo MIS-IHR than men (452 [22.9%] vs 59 636 [19.4%], respectively; P < .001), including both laparoscopic (348 [17.7%] vs 49 454 [16.1%], respectively) and robotic (104 [5.4%] vs 10 182 [3.3%], respectively) approaches. Compared with their male counterparts, women veterans who underwent IHR were younger (median [IQR] age, 56 [44-65] vs 65 [57-73] years for men), and less likely to have hypertension (917 [46.5%] vs 197 875 men [64.5%]), diabetes (257 [13.0%] vs 60 137 men [19.6%]), CHF (93 [4.7%] vs 26 603 men [8.7%]), and more likely to have depression (1097 [55.7%] vs 101 783 men [33.2%]).
Throughout the study period, overall IHR volume increased from 12 086 IHR in 2002 to 17 897 in 2022, yielding an increase of approximately 48.1% throughout the study period. Figure 1A demonstrates the annual trends in IHR technique and admission status over 21 years. Use of MIS-IHR increased substantially from 1102 (9.2%) in 2002 to 7286 (41.0%) in 2022. Use of robotic IHR techniques also increased from 9 (<0.1%) in 2007 to 2781 (16%) in 2022. When adjusted for the total number of veterans receiving VHA care per year, the number of IHRs ultimately increased incrementally from 2.28 IHRs per 1000 veterans in 2002 to 2.51 in 2022 (Figure 1B).
Dot Plot and Bar Graph Showing Inguinal Hernia Repair Procedure Type for US Veterans, 2002-2022A, Total number of minimally invasive surgery (MIS) vs open groin hernia repair in the inpatient and outpatient settings over 20 years. B, Total number of groin hernia repairs per 1000 veterans receiving care through the Veterans Health Association per year.
Procedure volume temporarily declined during the COVID-19 pandemic, with the most pronounced decrease seen in open repairs (Figure 1A). As shown in Figure 2, the proportion of urgent or emergent cases increased from 13 061 (5.0%) prepandemic to 4291 (8.8%) from 2020 to 2022. IHR volumes rebounded after 2020, increasing from 1.93 per 1000 veterans in 2020 to 2.51 in 2022, surpassing the prepandemic rate of 2.43 in 2019 (Figure 1B).
Dot Plot Showing Urgency of Inguinal Hernia Repairs for US Veterans, 2002-2022
After the implementation of expanded community care access in 2018, the proportion of procedures performed outside VAMC facilities more than doubled (1855 [0.8%] to 1755 [2.1%]). Differences in patient and operative characteristics between VAMC facilities and community-based surgeries are outlined in Table 3. Veterans treated in the community were older (median [IQR] age, 70 [62-78] vs 65 [57-73] years for the VAMC-treated group; P < .001), more likely to be female (65 [1.8%] vs 1906 [0.6%] for the VAMC-treated group; P < .001), and had greater comorbidity burdens (median [IQR] Elixhauser score, 10 [−1 to 24] vs 1 [−3 to 10] for the VAMC-treated group; P < .001), particularly with higher rates of diabetes (1056 [29.3%] for community care vs 59 338 [19.3%] for the VAMC-treated group) and CHF (834 [23.1%] vs 25 862 [8.5%] for the VAMC-treated group). Community-based IHRs were more often performed urgently or emergently (1015 [28.1%] vs 16 337 [5.4%] for the VAMC-treated group; P < .001). When comparing community care vs VAMC IHR by procedure type, 1829 (82%) vs 244 574 (80%) were open; 366 (16%) vs 49 436 (16%) laparoscopic; and 31 (1.4%) vs 10 255 (3.4%) robotic, respectively.
Discussion
This study offers a contemporary overview of IHR practice patterns across the VHA. Over the past 2 decades, IHR volume increased by 48.1%, with a 4.5-fold increase in MIS-IHR. Emergency repairs were more common among women and in community care. IHR represents a substantial and growing source of health care utilization for veterans.
While IHR trends are well documented in civilian populations, data for veterans remain limited. In England, inguinal hernias comprise approximately 71% of abdominal wall hernia repairs, with men facing a 9-fold higher lifetime risk.^2,17^ US estimates reported about 800 000 groin hernia repairs in 2003 and an 18.4% increase in groin and abdominal hernia burden from 1990 to 2019.^1,18^ Although our study covers a more contemporary time period and is specific to IHR, growth within the VHA exceeds this national trend, increasing 48.1% over 21 years.
Early VA Hernia Cooperative Study trials favored open repair based on recurrence, complications, and cost, though subsequent analyses suggested surgeon experience in MIS and older age may have contributed to these findings.^6,7,19^ Another RCT including 2 VAMCs initially supported watchful waiting for minimally symptomatic IHR, with a hernia accident rate of 0.0018 events per patient-year. However, long-term follow-up demonstrated that 68.0% of patients ultimately required surgery because of symptom progession.^4,5^ Our data reflect these shifts: MIS usage initially declined after the 2004 RCT but then rose steadily, even after the 2006 cost-effectiveness study favoring open repair. Similarly, total IHR volume dipped after the 2006 watchful-waiting RCT but rebounded following the 2013 long-term results. This suggests that VA-specific evidence does influence VA practice, but broader shifts in surgical innovation and training also play a role.
MIS adoption in the VHA has rapidly expanded despite earlier studies supporting open techniques. According to the Americas Hernia Society Quality Collaborative, MIS-IHR increased from 14% in 2003 to 58% in 2019.^1,12^ A National Surgical Quality Improvement Program (NSQIP) study from 2006 to 2017 demonstrated increase in MIS-IHR from 23.1 to 37.8%.^13^ Our data show a parallel rise of MIS-IHR within the VHA, from 9.2% in 2002 to 41.0% in 2022, as well as an increase in robotic IHR from 0.1% in 2007 to 16% in 2022, reflecting broader national trends in the VA and US.^20^ While the majority of IHRs in the VHA remain open, a decline from 91% to 59% in 2022 demonstrates substantial MIS adoption and improving alignment with contemporary guideline recommendations, likely reflecting increased MIS training, evolving surgeon experience, and broader dissemination of MIS techniques and resources within the VA. Prior VA analyses using VASQIP data reported similar proportions of MIS use, though VASQIP does not reflect total procedural volume, as our study does.^14^ Continued efforts to expand MIS approaches in VA practice are likely to further benefit eligible patients.
Our findings reveal notable differences between VA and civilian populations. In Medicare data, women comprised 13.6% of groin hernia repairs, while women made up just 0.6% of our IHR cohort, reflecting national veteran demographics.^21,22^ Interestingly, women in the Medicare study had a higher prevalence of comorbidities compared with men and were less likely to undergo MIS repairs than men, while our female veterans had a decreased comorbidity burden and were more likely to undergo MIS-IHR.^21^ Women veterans have more than double the risk of requiring an emergency hernia repair. These differences may arise because of a lower average age with associated lower comorbidity profiles, differential practice patterns, missed diagnoses in women, access to equipment or operative time, surgeon or patient preferences, intrinsic differences in pelvic anatomy, or other unidentified reasons. However, it should be noted that the increased use of MIS-IHR for women through the VA is in accordance with current international guidelines.^23^
Furthermore, urgency trends diverged between the VA and civilian populations. In the National Center for Health Statistics National Hospital Discharge Survey, there was an increase in emergent groin hernia repairs from 6.1 per 100 000 person-years in 2001 to 6.4 per 100 000 person-years in 2010.^24^ In our cohort, 6.5% of veterans underwent urgent/emergent repairs in 2002, which decreased to 5.0% in 2010.
Our data reflect the significant drop in elective surgical volume and increase in urgent/emergent IHR during the COVID-19 pandemic, aligning with national directives that resulted in a 75.0% reduction in elective procedures at the VA in 2020.^25^ When compared with total veteran encounters, elective cases decreased from 2.35 per 1000 encounters in 2019 to 1.70 in 2020 and urgent/emergent encounters increased from 0.09 to 0.23. While a similar decrease in elective hernia repairs (around 21.0%) during the pandemic was seen in a population analysis in Canada, Gomez et al^26^ did not see a difference in the rate of urgent IHR performed during this time. The cause of this increase in total urgent/emergent cases could be associated with recategorization of highly symptomatic hernias from “elective” to “urgent/emergent” status to overcome barriers to care. Ultimately, IHR volume through the VHA recovered and surpassed prepandemic levels, from 13 630 IHRs in 2020 to 17 897 in 2022.
Veterans are known to be older and carry a higher burden of comorbidities than the general population, which may contribute to increased hernia-related health care utilization.^27,28,29,30,31,32^ In our cohort, medical comorbidities were notably more common than previously reported in Medicare populations of patients undergoing IHR.^21^
The VHA is the nation’s only integrated, federally operated single-payer health care system. Maintaining surgical innovation is key to delivering high-quality care. Policies like the Veterans Choice Act (2014) and MISSION Act (2018) have expanded access to community-based care, increasing the number of procedures performed outside of VAMC facilities.^16,33^ Various studies have found VAMC outcomes to be comparable or better than community hospitals.^34,35,36,37^ While Graham et al^34^ found that veterans referred to non-VA care were typically younger and White with fewer comorbidities, our findings reveal that community-based IHRs tended to involve more urgent cases and medically complex patients. This may reflect referrals of complex cases to academic centers or triage decisions for urgent treatment at closest geographic facilities. Nevertheless, the majority of elective IHRs among veterans are performed at VAMC facilities, a trend consistent with prior research demonstrating veterans’ preferences to remain in the VA system.^38,39^
Understanding shifts in surgical practice is vital given implications for cost and quality. In 2003, repair of abdominal wall hernias cost nearly 2.5 billion annually.^[1](#soi260010r1)^ More recent estimates according to NSQIP in 2016 placed the average cost at 4360 for open and 5105 for MIS-IHR repairs.^[40](#soi260010r40)^ Applying these costs to our observed volumes over this 20-year period, the projected cost of veteran IHRs would exceed 1.38 billion if delivered in the private sector. These figures highlight the importance of improving hernia prevention and reducing recurrence, both to contain costs and enhance quality of care.
Although this study did not directly evaluate prevention or recurrence strategies, the high IHR burden observed underscores the importance of actionable opportunities to improve quality and reduce costs. Evidence-based interventions, including smoking cessation, weight optimization, glycemic control, risk stratification, and prehabilitation, reduce complications and recurrence and can integrate into existing VHA preoperative pathways.^41,42,43,44,45,46,47,48,49,50,51^ Guideline-concordant use of MIS techniques and resources may further improve outcomes.^52,53,54,55^ Postoperative, structured follow-up and patient education (leveraging the VHA’s robust telehealth infrastructure) offers scalable approaches to early complication detection and recurrence mitigation.^47,56,57,58^ The VHA’s integrated data systems support longitudinal outcome tracking and continuous quality improvement.^36,59,60^ eTable 2 in Supplement 1 summarizes evidence-supported interventions and potential implementation pathways within the VA.
Limitations
Limitations of this study include potential data inaccuracies inherent to large database analyses. For veterans who received care at non-VAMC facilities funded by the VHA, missing or inconsistent data may arise due to differences in electronic medical records. For consistency, comorbidity data were gathered from the CDW, and therefore, there may be additional missing data regarding comorbidities diagnosed in patients through community care facilities. Key clinical details, such as patient outcomes, recurrence rates, wound classification, hernia size and location, mesh use, and cost, were not captured and remain important areas for future investigation.
Conclusions
This study found that over the past 20 years, the volume of IHRs performed in the VHA system has increased, along with MIS approaches. IHRs continue to represent a substantial part of the surgical workload in the veteran population, highlighting both changing surgical practices and the distinct health care needs of this group. Our findings reflect parallel growth and innovation within the VHA compared with civilian systems but also underscore the broader public health significance of abdominal core health for both veterans and civilians. Increased investment is needed to enhance care quality, support research, track treatment outcomes, and prioritize hernia prevention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am. 2003;83(5):1045-1051, v-vi. doi:10.1016/S 0039-6109(03)00132-414533902 · doi ↗ · pubmed ↗
- 2Primatesta P, Goldacre MJ. Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol. 1996;25(4):835-839. doi:10.1093/ije/25.4.8358921464 · doi ↗ · pubmed ↗
- 3Poulose BK, Adrales GL, Janis JE. Abdominal core health: a needed field in surgery. JAMA Surg. 2020;155(3):185-186. doi:10.1001/jamasurg.2019.505531851303 · doi ↗ · pubmed ↗
- 4Fitzgibbons RJ Jr, Giobbie-Hurder A, Gibbs JO, . Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA. 2006;295(3):285-292. doi:10.1001/jama.295.3.28516418463 · doi ↗ · pubmed ↗
- 5Fitzgibbons RJ Jr, Ramanan B, Arya S, ; Investigators of the Original Trial. Long-term results of a randomized controlled trial of a nonoperative strategy (watchful waiting) for men with minimally symptomatic inguinal hernias. Ann Surg. 2013;258(3):508-515. doi:10.1097/SLA.0b 013e 3182 a 1972524022443 · doi ↗ · pubmed ↗
- 6Neumayer L, Giobbie-Hurder A, Jonasson O, ; Veterans Affairs Cooperative Studies Program 456 Investigators. Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med. 2004;350(18):1819-1827. doi:10.1056/NEJ Moa 04009315107485 · doi ↗ · pubmed ↗
- 7Hynes DM, Stroupe KT, Luo P, . Cost effectiveness of laparoscopic versus open mesh hernia operation: results of a Department of Veterans Affairs randomized clinical trial. J Am Coll Surg. 2006;203(4):447-457. doi:10.1016/j.jamcollsurg.2006.05.01917000387 · doi ↗ · pubmed ↗
- 8Wauschkuhn CA, Schwarz J, Boekeler U, Bittner R. Laparoscopic inguinal hernia repair: gold standard in bilateral hernia repair? results of more than 2800 patients in comparison to literature. Surg Endosc. 2010;24(12):3026-3030. doi:10.1007/s 00464-010-1079-x 20454807 · doi ↗ · pubmed ↗