A Shared Medical Appointment Program to Improve Self-management of Metabolic Dysfunction–Associated Steatotic Liver Disease
Lisa L. Catalli, Nghiem B. Ha, Sara A. Miller, Eliana Z. Agudelo, Simone K. Madan, Asal Bastani, Riley Tan, Danielle Brandman, Jennifer C. Lai

TL;DR
A telehealth program called BRIDGE improves patients' knowledge and confidence in managing metabolic dysfunction–associated steatotic liver disease.
Contribution
BRIDGE is a novel telehealth shared medical appointment program designed to enhance self-management of MASLD.
Findings
Participants showed significant improvements in knowledge and confidence in making health behavioral changes.
Self-efficacy in managing emotions and accessing health information increased after the program.
The program was effective across diverse patient demographics, including transplant recipients and those with cirrhosis.
Abstract
Metabolic dysfunction–associated steatotic liver disease (MASLD) is the most common liver disease, with a rising global prevalence exceeding 30%. Effective lifestyle intervention programs are critically needed to enhance the self-management of individuals with MASLD. We implemented Behavioral Resources and Intervention through Digital Group Education (BRIDGE), a 6-session, group telehealth psychoeducational program in shared medical appointments in an academic outpatient hepatology clinic. The aim of this study is to evaluate the program’s impact on participants’ knowledge, confidence, and self-efficacy in managing MASLD. In a single-arm quasi-experimental study from January 2022 to May 2024, BRIDGE participants completed preintervention and postintervention surveys. We analyzed demographic and clinical data from medical records and survey responses assessing for change in knowledge…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1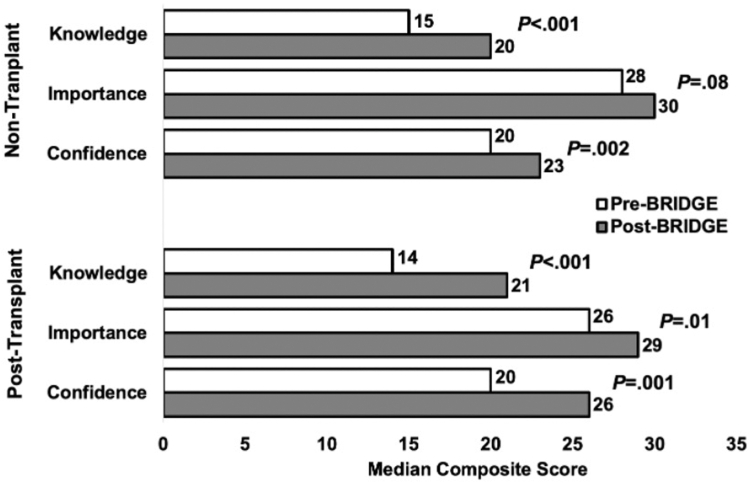 Figure 2
Figure 2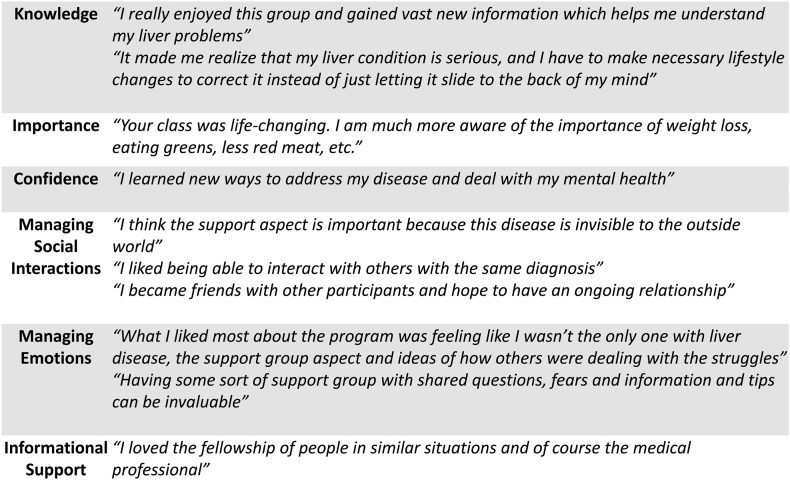 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease Diagnosis and Treatment · Diabetes Management and Education · Diabetes, Cardiovascular Risks, and Lipoproteins
Introduction
Metabolic dysfunction–associated steatotic liver disease (MASLD), involving hepatic steatosis with at least 1 cardiometabolic risk factor, affects over 30% globally and is expected to become the leading cause of liver transplantation.1^,^2 Its prevalence has risen in parallel with obesity and diabetes, significantly impacting liver and non–liver-related morbidity and mortality.3 The cornerstone of MASLD care is lifestyle counseling for clinically significant weight loss.4 Greater efforts are needed to create real-world care models that incorporate behavioral approaches to enhance self-efficacy in order to sustain behavioral changes for weight management.5 Current clinical frameworks are inadequate for addressing the structural, social, and environmental factors contributing to the public health crisis of obesity, diabetes, and MASLD.6^,^7 Barriers like lack of knowledge about MASLD, access to care, food insecurity, and obesogenic environment exacerbate inequities for socially disadvantaged populations.6, 7, 8 Calls for person-centered, team-based care and longitudinal lifestyle programs necessitate substantial health system improvements to close care gaps and reduce inequities.1^,^9^,^10
A shared medical appointment (SMA) care delivery model offers an innovative approach to bridge healthcare gaps by incorporating group-based behavioral interventions into conventional care.11 SMAs involve multiple patients attending a concurrent, extended visit while still receiving individual consultations to collaboratively develop personalized health behavior goals. Utilizing telemedicine for these programs can help mitigate structural and economic barriers, reducing patient costs and facilitating more frequent visits.12^,^13 Evidence strongly supports that SMA models lead to significant improvement in patient trust, quality of care, quality of life, and clinical outcomes, particularly in diabetes management and obesity treatment.11, 12, 13, 14, 15, 16, 17
We implemented a group telehealth SMA program—Behavioral Resources and Intervention through Digital Group Education (BRIDGE)—to support lifestyle changes in patients with MASLD. A feasibility study of this program was detailed in a previous publication.18 To expand this model, we adapted sessions for both pre- and post-liver transplant (LT) patients with and without cirrhosis. Our ongoing BRIDGE study aims to evaluate the program’s effectiveness in improving patients' knowledge, confidence, and self-efficacy in managing MASLD.
Methods
Study Design and Patient Selection
The BRIDGE research study described in this article is a single-arm quasi-experimental pre- and post-test study and is part of an ongoing, prospective longitudinal study. This study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology checklist for reporting observational studies.19 Included were adult patients who were evaluated and referred from a hepatology or LT clinic at a single academic LT center. Enrollment in BRIDGE was voluntary and occurred between January 2022 and May 2024. Eligibility included adults over 18 years with a clinical diagnosis of MASLD and/or cirrhosis based on noninvasive testing (including vibration-controlled transient elastography [VCTE] and/or elastography) and/or liver biopsy, as well as access to a smartphone, device, or computer with adequate broadband for telehealth. Post-LT patients and patients with cirrhosis were included if they had at least 1 cardiometabolic risk factor, such as obesity, diabetes, hypertension, and/or hyperlipidemia. Exclusion criteria included decompensated cirrhosis, alcohol or polysubstance use disorder, cognitive impairment, severe physical disability, pregnancy, or uncontrolled psychiatric disorders. All participants continued standard medical care as recommended by their providers (usually every 3–12 months). Due to the small number of Spanish-monolingual patients (n = 6), only English-speaking participants were included in this study.
The logistics and operations of the BRIDGE clinical program are described in our previous publication regarding the feasibility of the program.18 Approximately 1–2 weeks prior to the first BRIDGE session, patients received an invitation via the electronic health records email system to participate in the research study. Participation in the research part of the program was optional. The email included an anonymous link to a pre-BRIDGE survey hosted on Qualtrics, which contained informed consent and Health Insurance Portability and Accountability Act forms. Patients who consented completed the survey, with assurances of anonymous data collection to reduce coercion. After completing the BRIDGE program, only those who had completed the pre-BRIDGE survey were sent a post-BRIDGE survey, along with reminders at 2 weeks, 1 month, and 3 months if needed. Baseline patient demographic and clinical data were extracted from medical records.
Ethics and consent to participate
All research was conducted in accordance with both the Declarations of Helsinki and Istanbul. This study was approved by the institutional review board at the University of California, San Francisco (San Francisco, CA, USA). A waiver of signed consent was granted for this study.
Program Intervention and Theoretical Framework
BRIDGE is a video-based group telehealth program that aims to provide accessible, longitudinal psychoeducational support across health domains. The program features 90-minute SMA sessions held every 2 weeks for 12 weeks, led independently by an advanced practice provider (APP). A detailed description of the curriculum is available in a previous publication.18 Each group, with a maximum of 7 participants, is closed to new members after enrollment. Each session starts with a 10-minute check-in, followed by a 20-minute live didactic PowerPoint presentation by the APP, a 30-minute questions/answers session, and a facilitated group discussion. In the last 30 minutes, the APP meets individually with participants to support their personalized goals, while the rest of the group engages in discussions about a topic or patient activity. To ensure consistency between sessions, APP group leaders use a standardized PowerPoint slide deck with speaker notes, incorporating motivational interviewing to engage participants and encourage the development of actionable health behavioral goals aligned with their core values (Figure 1).Figure 1BRIDGE program conceptual model and characteristics.
The program was built on evidence showing that effective group lifestyle interventions include educational components, peer interaction to build community, and personalized support in self-management.5^,^9^,^15^,^20^,^21 Theoretical underpinnings of the program included Social Cognitive Theory22^,^23 and the Transtheoretical Model.24 A weight management psychologist was involved in program development to ensure program fidelity. Cognitive behavioral therapy strategies were incorporated into each session to help participants to consider the interconnections between thoughts, mood, environment, and health-related behavior. Participants developed self-directed goals on a BRIDGE goal tracker during and between sessions. Educational handouts and resources on diet and physical activity were provided for sessions on dietary habits and physical activity.
Administered Surveys
The preintervention and postintervention surveys included 3 multiple-choice knowledge questions on liver-related knowledge to objectively assess changes in participants’ understanding of their liver disease and brief psychosocial scales based on self-efficacy and social support constructs. The survey was developed in collaboration with an expert weight management psychologist who is part of the BRIDGE research team. It included 5-point Likert scales in which participants rated their knowledge about MASLD, the importance of liver health, and their confidence in making changes related to goal setting, diet, physical activity, stress management, sleep, and social support. We selected 6 validated short forms (SF) of the Patient-Reported Outcomes Measurement Information System (PROMIS), developed by the National Institutes of Health: Depression SF 4a-Adult v1.0, Anxiety SF 4a-Adult v1.0, Meaning and Purpose SF 4a-Adult v1.0, Self-Efficacy for Managing Chronic Conditions-Managing Emotions SF 4a-Adult v1.0, Self-Efficacy for Managing Chronic Conditions-Managing Social Interactions SF 4a-Adult v1.0, and Informational Support SF 4a-Adult v2.0.25^,^26 Additionally, the survey included a question adapted from Exercise in Medicine to estimate weekly exercise minutes.27 The postintervention survey included an invitation for written feedback on the longitudinal experience with the program.
Statistical Analysis
Baseline characteristics and the impact of the intervention on outcomes were analyzed using descriptive and bivariate statistical methods. Categorical variables were compared using Pearson’s chi-square test, while continuous variables were assessed with independent t-tests. For variables with non-normal distributions, data were summarized using the median and interquartile range (IQR) (Q1, Q3) and compared using the Wilcoxon signed-rank test. PROMIS scores were calculated using a publicly available scoring system which generated total raw scores and conversion into standardized T-scores. A T-score of 40 corresponds to 1 SD below the population mean, while a T-score of 60 corresponds to 1 SD above. Higher T-scores indicate a greater severity or presence of the measured construct (eg, higher depression, greater meaning, and purpose). The internal consistency reliability of each measure was evaluated using Cronbach’s alpha coefficient. A 2-sided P value < .05 was considered statistically significant. Analyses were performed using STATA, version 15.1 (StataCorp, College Station, TX, USA).
Results
Baseline Patient Characteristics
Out of the 127 patients who participated in 30 cohorts of the BRIDGE SMA program between March 2022 and May 2024, 70 patients completed pre- and post-surveys, of which 25 (or 36%) were LT recipients. Baseline patient demographics are shown in Table 1.Table 1. Baseline Patient CharacteristicsOverall n = 70Non-liver transplant n = 45Post-liver transplant n = 25Sex (female)49 (70)35 (78)14 (56)Age (y, IQR)57 (46–66)57 (45–66)60 (50–65)Race/ethnicity Non-Hispanic White31 (44)21 (47)10 (40) Hispanic White20 (29)14 (31)6 (24) Asian10 (14)7 (16)3 (12) Black3 (4)0 (0)3 (12) Native American3 (4)2 (4)1 (4) Other3 (4)1 (2)2 (8)Insurance type Medicaid/Medicare29 (41)14 (31)15 (60)Type 2 diabetes mellitus29 (41)16 (36)13 (52)Hypertension44 (63)24 (53)20 (80)Hyperlipidemia41 (59)27 (60)14 (56)Coronary artery disease5 (7)3 (7)2 (8)Cerebrovascular disease3 (4)3 (7)0 (0)Tobacco use None49 (70)34 (76)15 (60) Prior21 (30)11 (24)10 (40)Alcohol use None49 (70)28 (62)21 (84) Occasional15 (21)13 (29)2 (8) Prior heavy6 (9)4 (9)2 (8)Fibrosis stage 0–126 (60)18 (60)8 (62) 24 (9)3 (10)1 (8) 33 (7)1 (3)2 (15) 410 (23)8 (27)2 (15)Steatosis grade 0–19 (21)5 (17)4 (30) 21 (2)1 (3)0 (0) 333 (77)24 (80)9 (69)Fibrosis type Liver biopsy3 (7)3 (10)0 (0) Fibroscan40 (93)27 (90)13 (100)Values reported in number (percentage).
Among the nontransplant cohort, the majority were women (78%) with a median age of 57 years and predominately non-Hispanic White (47%) followed by 31% Hispanic and 16% Asian. About one-third of participants (31%) had public health insurance (Medicaid/Medicare). The majority were overweight/obese (84%) with a median body mass index (BMI) of 33.8 kg/m^2^. Metabolic risk factors were as follows: 36% with type 2 diabetes mellitus, 53% with hypertension, 60% with hyperlipidemia, and 14% with prior cerebrovascular events. Prior tobacco and alcohol use was present in 24% and 38%, respectively. Among patients with available VCTE (n = 30), 80% had severe steatosis with a median controlled attenuation parameter of 333 dB/m (IQR, 319–359 dB/m).
Among the post-transplant cohort, nearly half (48%) had metabolic dysfunction-associated steatohepatitis (MASH) cirrhosis as the primary transplant etiology, with a median post-transplant duration of 4 years (IQR, 2–9 years). The majority were women (56%) with a median age of 60 years and predominately non-Hispanic White (40%) followed by 24% Hispanic, 12% Asian, and 12% Black. Most participants (60%) had public health insurance (Medicaid/Medicare). Overweight/obesity was present in 60% of the cohort with a median BMI of 32.0 kg/m^2^. Metabolic risk factors were as follows: 52% with type 2 diabetes mellitus, 80% with hypertension, 14% with hyperlipidemia, and 8% with prior cerebrovascular events. Among patients with available VCTE (n = 13), 69% had severe steatosis with a median controlled attenuation parameter of 307 dB/m (IQR, 266–340 dB/m).
Attendance for the BRIDGE sessions was adequate, with low attrition rates. Among the 70 participants enrolled in the BRIDGE research study, 83% attended 5 or more sessions, and 91% attended 4 or more sessions, demonstrating high engagement and commitment to the program.
Pre- and Post-Survey From BRIDGE Program Intervention
The reliability analysis of all mental and social domains across the surveys, including each PROMIS SF, demonstrated very good to excellent internal consistency, with Cronbach’s alpha ranging from 0.88 to 0.95.
The PROMIS T-score results are summarized in Table 2. The composite T-scores at baseline ranged from 44.4 to 59.0. Within-group minimal important change from pre- and post-composite scores ranged from absolute values of 1–5.3. Among the non-LT participants, there were significant improvements in the T-scores of Meaning and Purpose (P = .01), Managing Emotions (P = .02), Managing Social Interactions (P = .01), and Informational Support (P = .02), after participating in the intervention. Among LT participants, there were significant improvements in the T-scores of Depression (P = .03), Meaning and Purpose (P = .003), Managing Emotions (P = .001), and Informational Support (P = .002).Table 2. Pre- and Post-BRIDGE Intervention Among Different PROMIS DomainsPre-BRIDGEPost-BRIDGEΔ pre-postP valueDepression Nontransplant53.8 ± 10.652.8 ± 9.6−1.0.40 Post-transplant52.6 ± 7.549.2 ± 7.1−3.4.03Anxiety Nontransplant56.7 ± 10.855.8 ± 9.7−1.2.51 Post-transplant59.0 ± 5.358.3 ± 6.6−0.7.42Meaning and purpose Nontransplant49.5 ± 10.451.7 ± 9.32.2.01 Post-transplant49.3 ± 8.554.5 ± 7.75.2.003Managing emotions Nontransplant45.6 ± 8.247.4 ± 8.11.8.02 Post-transplant48.9 ± 6.154.2 ± 7.05.3.001Managing social interactions Nontransplant44.4 ± 8.447.2 ± 7.92.8.01 Post-transplant46.6 ± 9.847.9 ± 6.31.3.31Informational support Nontransplant50.8 ± 10.453.8 ± 7.83.0.02 Post-transplant55.7 ± 7.060.2 ± 7.44.5.002Values reported in mean ± standard deviation of T-scores for each PROMIS domain; higher scores for domains indicate a higher presence of the measured construct (eg, higher depression, greater meaning, and purpose).
Survey results assessing perceived knowledge, importance, and confidence related to the management of MASLD—including dietary habits, physical activity, sleep habits, stress management, and goal-setting behaviors—are presented in Figure 2. Following the BRIDGE intervention, participants demonstrated significant improvements in perceived knowledge across all groups (P < .001), in the perceived importance of learning ways to improve MASLD among LT recipients (P = .01), and in perceived confidence to implement behavioral changes among both non-LT (P = .002) and post-LT participants (P = .001). Additionally, all BRIDGE participants showed improved scores of the 3 objective questions evaluating MASLD epidemiology, diagnosis, and management. Domain-specific results for the median composite scores of knowledge, importance, and confidence are detailed in Supplementary Tables 1 and 2.Figure 2. Impact of the BRIDGE intervention on patient knowledge, perceived importance, and confidence among nontransplant and post-transplant patients.
Among the 43 nontransplant participants who completed surveys on physical activity before and after the BRIDGE intervention, there was a notable trend toward increased frequency (days per week) and duration (minutes per day) of moderate-to-vigorous physical activity. Participants also reported a significant increase in muscle-strengthening exercises, with the median frequency rising from 1 to 2 days per week (P < .05). In contrast, data on physical activity among post-LT participants were limited due to the delayed inclusion of this section in the survey, resulting in incomplete responses from this group.
Patient feedback regarding the BRIDGE program, stratified by self-efficacy domains, is presented in Figure 3. Overall, participants reported high levels of satisfaction, consistent with the improvements observed in preintervention and postintervention survey scores. Several key themes emerged from qualitative feedback, including increased understanding of liver health, adoption of healthier behaviors, and the establishment of realistic health goals. Many participants also reported decreased anxiety, emotional distress, and social isolation related to their diagnosis. Notably, the community aspect of the BRIDGE program was frequently highlighted as a valuable component, with participants emphasizing the importance of shared experiences and mutual support in driving both behavioral and emotional change.Figure 3. Patient response and feedback after BRIDGE according to different self-efficacy domains.
Changes in Clinical Variables
Preintervention and postintervention clinical changes among the 70 BRIDGE participants are summarized in Table 3. Most participants (78%) experienced modest weight loss, with a median reduction weight loss (IQR) of 2 pounds (IQR 0–7). Among non-LT participants, the median BMI decreased from 33.5 kg/m^2^ to 32.6 kg/m^2^ (P = .001), while in transplant recipients, the median BMI decreased from 32 kg/m^2^ to 30.1 kg/m^2^ (P = .06).Table 3. Pre- and Post-BRIDGE Intervention Among Different Clinical CharacteristicsPre-BRIDGEPost-BRIDGEP valueBody mass index (kg/m^2^) Nontransplant33.8 (30.2–39.5)32.6 (29.5–38.3).001 Post-transplant32.0 (26.6–37.1)30.1 (26.1–36.5).06Liver-related labs AST (U/L) Nontransplant30 (23–44)27 (21–33).24 Post-transplant23 (18–34)22 (18–27).26 ALT (U/L) Nontransplant36 (22–56)30 (24–46).22 Post-transplant23 (18–42)23 (18–36).13 ALP (U/L) Nontransplant87 (66–105)84 (67–107).22 Post-transplant84 (68–96)75 (67–90).42 Total bilirubin (mg/dL) Nontransplant0.6 (0.5–0.8)0.6 (0.5–0.8).88 Post-transplant0.6 (0.4–0.7)0.6 (0.4–0.8).09 Creatinine (mg/dL) Nontransplant0.8 (0.7–0.9)0.8 (0.7–0.9).26 Post-transplant1.2 (1.0–1.4)1.2 (1.0–1.4).32 Platelet (10^9^/L) Nontransplant203 (161–263)202 (174–238).43 Post-transplant191 (162–236)173 (145–223).13Metabolic-related labs HbA1c (%) Nontransplant5.7 (5.4–6.4)5.9 (5.5–6.1).92 Post-transplant6.6 (5.6–6.6)6.9 (6.1–8.4).18 Total cholesterol Nontransplant170 (155–209)172 (141–189).93 Post-transplant218 (197–225)196 (175–215).18 Triglyceride Nontransplant148 (109–193)124 (80–159).20 Post-transplant230 (165–529)306 (109–343)1.00 HDL Nontransplant40 (36–52)40 (34–62)1.00 Post-transplant38 (32–51)47 (33–53).59 LDL Nontransplant105 (93–120)100 (52–114).15 Post-transplant101 (99–150)92 (78–117).11 FIB-4 Nontransplant1.69 (0.87–2.67)1.59 (0.78–2.20).89 Post-transplant1.57 (0.92–2.00)1.69 (1.08–2.14).70 VCTE CAP (dB/m) Nontransplant333 (319–359)276 (244–330).90 Post-transplant307 (266–340)301 (262–343).21 LSM (kPa) Nontransplant5.7 (4.6–11.4)4.8 (4.6–8.1).78 Post-transplant5.8 (4.5–8.4)5.5 (5.2–7.4).73Values reported in median (IQR).ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CAP, controlled attenuation parameter; FIB-4, Fibrosis-4 Index; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LSM, liver stiffness measurement.
Discussion
This preintervention/postintervention study demonstrates that the BRIDGE telehealth psychoeducation SMA program is an effective and innovative care model for improving self-efficacy and promoting meaningful health behavior changes among individuals with MASLD. The program significantly enhanced patient knowledge of MASLD, improved understanding of health-related behavioral changes, and increased confidence in implementing these changes across multiple health domains. While many intervention studies have emphasized behavior change as the primary outcome, this study focused on building self-efficacy—a key mediator of behavior change associated with achieving meaningful health outcomes, such as weight loss or improved glycemic control in metabolic syndrome.28^,^29 The BRIDGE program seeks to empower individuals living with MASLD by addressing physical, mental, and psychological barriers through peer engagement and providing self-management tools. Embracing a group motivational interviewing approach, the BRIDGE intervention encourages participants to support one another in creating personalized strategies to enhance metabolic and overall health, rather than imposing standardized outcome targets.
Most patients (77%–80%) achieved weight loss and reported increased levels of physical activities after participating in BRIDGE. While patients were educated on the benefits of weight loss for MASLD, it was not a primary endpoint of this intervention for several reasons. First, the program’s short duration was not expected to result in significant weight loss. Existing studies have demonstrated that 24 weeks of intervention are needed for clinically meaningful weight reduction.30, 31, 32 Second, insights from our BRIDGE feasibility study revealed diverse participant goals. Some participants aimed to lose weight, while others prioritized changing thinking patterns, improving their social network, increasing muscle mass, or reducing body fat. During 1:1 consultation with the APP, participants were encouraged to evaluate their satisfaction with behavioral changes rather than focusing on specific quantifiable weight lost. They were also informed that both aerobic and resistance exercises improve metabolic parameters and MASLD, even without weight loss.33 We observed a significant increase in the frequency of resistance exercise among participants.
A strength of this study is the strong representation of Hispanic participants, who comprised approximately one-third of the BRIDGE cohort, the majority of whom were English-speaking Hispanic patients. This reflects the demographic composition of Northern California and aligns with the disproportionately high prevalence of MASLD and MASH in this population. Health disparities exacerbate the risk of MASH fibrosis among Hispanic adults, underscoring the need for targeted public health initiatives to improve care delivery.7^,^34^,^35 Although Spanish-language BRIDGE sessions led by a bilingual APP were implemented to enhance access for Spanish-monolingual patients, this group was excluded from the current analysis due to the small sample size (n = 6), as well as the absence of Spanish-language consent forms and validated survey tools. Additional barriers, such as patient availability and telehealth inequities, further limited participation among Spanish-monolingual patients. Future research will prioritize bilingual consent and survey materials, as well as establishing partnerships with community-based organizations to codevelop culturally and linguistically tailored interventions.
The BRIDGE telehealth SMA program was designed as an accessible, cost-effective care model to reduce structural and economic barriers for underserved patients. Notably, the program demonstrated strong attendance rates across all participants, highlighting its acceptability and feasibility. In our prior feasibility study, 75% of participants attended at least 5 out of 6 sessions, though 34% missed more than 1 session, with lower completion rates among women and Hispanic individuals.18 In the current cohort, 85% attended at least 5 out of 6 sessions, and only 17% missed more than 1 session. Encouragingly, no significant differences in attendance were observed based on sex and ethnicity, indicating the program’s broad reach and ability to engage diverse populations effectively.
Importantly, these findings suggest that the BRIDGE model is generalizable beyond health systems with telehealth reimbursement. Although lack of coverage remains a barrier in some regions, the program can be implemented through alternative mechanisms such as value-based care arrangements, institutional population health initiatives, or bundled care pathways for MASLD. Group-based care delivery enhances efficiency by allowing a single multidisciplinary team to care for multiple patients simultaneously, reducing per-patient resource utilization compared to individual visits. Hybrid models incorporating in-person sessions or asynchronous educational content may further improve feasibility in settings with limited resources or telehealth coverage. Together, the high engagement observed across diverse populations supports the scalability of this model and provides a pragmatic framework for broader implementation, even in the absence of direct telehealth reimbursement.
The findings should be interpreted considering the limitations of this pilot study design. This study used a convenience sample of patients internally referred to the BRIDGE program by hepatology providers in our outpatient clinic. The lack of a matched comparison group limits both internal validity and generalizability. The pretest and posttest design is particularly vulnerable to confounding factors such as history, maturation, regression to the mean, and contextual effects, which may have influenced the observed outcomes. Survey completion rates were modest, with approximately 55% of participants completing both pre- and post-program surveys. This outcome was likely influenced by limited survey funding, as no incentive payments were offered, and surveys were administered separately from clinical encounters. Consequently, selection bias may have occurred, as those who completed surveys may have been more engaged with the program or perceived greater benefits from it. Although participants were assured of the anonymity of their survey responses, factors such as reactivity, recall bias, and carryover effects may have influenced the self-reported data. Additionally, reliance on self-reported measures of weight and physical activity frequency may have introduced bias, potentially overestimating or underestimating actual behavioral changes.
The BRIDGE program is an ongoing initiative with plans for future iterations and refinements. Longitudinal follow-up will assess the program's effectiveness in sustaining behavioral changes, achieving weight loss, and improving cardiometabolic health. Future iterations should address barriers faced by digitally underserved populations and incorporate strategies to improve inclusivity. In conclusion, the BRIDGE telehealth SMA program represents an innovative and cost-effective model for reducing healthcare disparities and empowering MASLD patients to improve their health. By addressing the physical, emotional, and social dimensions of MASLD care, BRIDGE has laid the groundwork for scalable and sustainable behavioral health interventions in hepatology. Moving forward, we aim to build academic-community partnerships and expand the program’s reach to better support underserved populations and advance MASLD care.
Conclusion
The BRIDGE telehealth SMA program is an innovative, accessible, and effective care model that improves self-efficacy and promotes meaningful health behavior changes for individuals with MASLD. Participants gained knowledge and confidence, with most achieving weight loss and increased physical activity. The program addresses physical, emotional, and social barriers through peer engagement and personalized strategies, showing strong feasibility and scalability across diverse populations. Future efforts will evaluate longitudinal outcomes and inclusivity, address telehealth barriers, and expand reach to underserved communities to further advance MASLD care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tacke F.Horn P.Wong V.W.S.EASL–EASD–EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD)J Hepatol 81320244925423885199710.1016/j.jhep.2024.04.031 · doi ↗ · pubmed ↗
- 2Younossi Z.M.Golabi P.Paik J.M.The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review Hepatology 7742023133513473662663010.1097/HEP.0000000000000004 PMC 10026948 · doi ↗ · pubmed ↗
- 3Xiao J.Ng C.H.Chan K.E.Hepatic, extra-hepatic outcomes and causes of mortality in NAFLD – an umbrella overview of systematic review of meta-analysis J Clin Exp Hepatol 13420236566653744094910.1016/j.jceh.2022.11.006PMC 10333954 · doi ↗ · pubmed ↗
- 4Vilar-Gomez E.Martinez-Perez Y.Calzadilla-Bertot L.Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis Gastroenterology 14922015367378.e 52586504910.1053/j.gastro.2015.04.005 · doi ↗ · pubmed ↗
- 5Annesi J.J.Behavioral weight loss and maintenance: a 25-year research program informing innovative programming Perm J 2622022981173593367810.7812/TPP/21.212PMC 9662257 · doi ↗ · pubmed ↗
- 6Javed Z.Valero-Elizondo J.Maqsood M.H.Social determinants of health and obesity: findings from a national study of US adults Obesity (Silver Spring)30220224915023508855110.1002/oby.23336 · doi ↗ · pubmed ↗
- 7Kardashian A.Serper M.Terrault N.Health disparities in chronic liver disease Hepatology 7742023138214033599334110.1002/hep.32743 PMC 10026975 · doi ↗ · pubmed ↗
- 8Shibayama K.Furushima C.Saka M.Barriers to lifestyle modification in patients with non-alcoholic fatty liver disease: a scoping review J Rural Med 1912024193819680810.2185/jrm.2023-026PMC 10774003 · doi ↗ · pubmed ↗