A Prospective, Randomized Comparative Study of Intravenous and Perineural Dexamethasone as an Adjuvant to Levobupivacaine in Ultrasound-Guided Supraclavicular Brachial Plexus Block for Adult Patients Undergoing Elective Upper Limb Surgery
Rashmi Soni, Sweta Singh, Sudhir K Dhama, Pramod Chand

TL;DR
This study compares two ways of giving dexamethasone during anesthesia for arm surgery and finds that giving it near the nerve works better than through the vein.
Contribution
The study provides new evidence that perineural dexamethasone improves block effectiveness more than intravenous administration.
Findings
Perineural dexamethasone led to faster onset and longer duration of sensory and motor block.
Postoperative analgesia was significantly longer with perineural dexamethasone.
No serious complications were observed in either group.
Abstract
Background Ultrasound-guided supraclavicular brachial plexus block is a widely used regional anesthesia technique for upper limb surgeries, offering effective intraoperative and postoperative analgesia. Dexamethasone, a corticosteroid with analgesic and anti-inflammatory properties, is often used as an adjuvant via either the perineural or the intravenous route to prolong block duration. This study aimed to compare the efficacy of intravenous versus perineural dexamethasone as adjuvants to levobupivacaine in ultrasound-guided supraclavicular blocks. Methods A prospective, randomized, double-blind study was conducted at Sardar Vallabh Bhai Patel Hospital, Meerut, over 18 months. Sixty American Society of Anesthesiologists (ASA) I/II adult patients aged 18-60 years undergoing elective upper limb surgeries were randomly allocated into two equal groups. Group A received 19 mL of 0.5%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
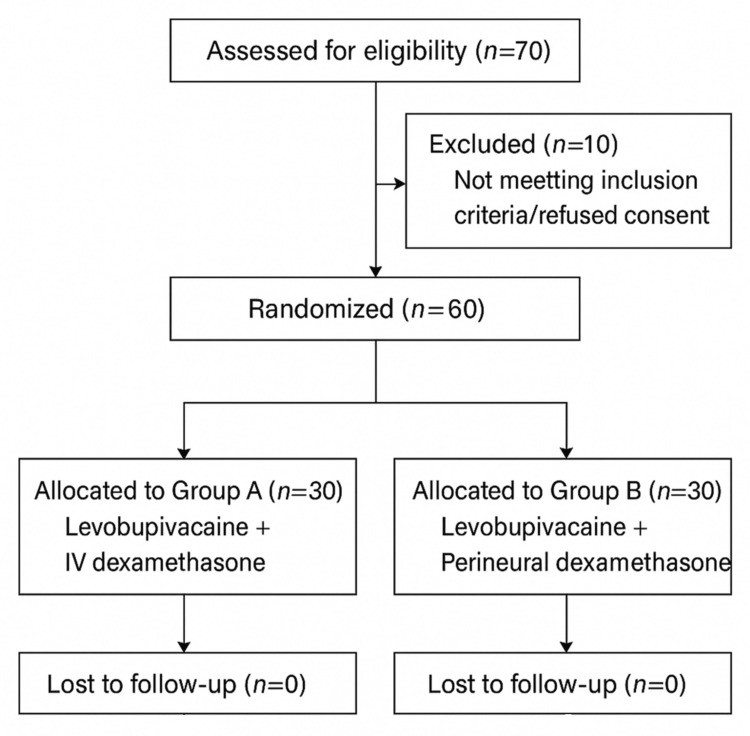 Figure 1
Figure 1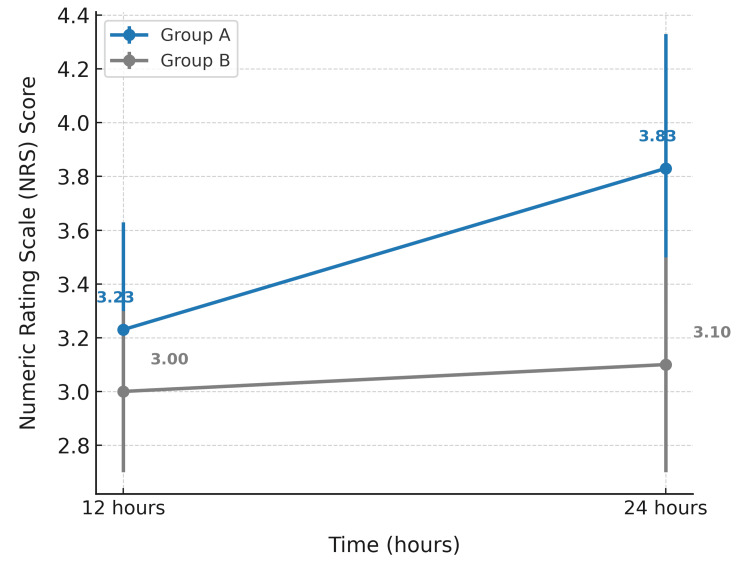 Figure 2
Figure 2| Baseline Characteristics | Groups | t value | p-value | ||
| A | B | ||||
| Age (years) | 38.17±12.50 | 39.67±12.82 | -.459 | .648 | |
| Sex | Male | 17 (56.7%) | 17 (56.7%) | - | 1.000 |
| Female | 13 (43.3%) | 13 (43.3%) | |||
| BMI (kg/m2) | 21.15±2.12 | 21.27±1.78 | -.231 | .818 | |
| ASA | Grade 1 | 17 (56.7%) | 17 (56.7%) | - | 1.000 |
| Grade 2 | 13 (43.3%) | 13 (43.3%) | |||
| Parameters | Groups | t value | p-value | |
| A | B | |||
| Duration of surgery | 98.17±32.73 | 98.50±30.18 | -.041 | .967 |
| Sensory block onset | 10.37±1.97 | 20.13±3.09 | -14.58 | .001 |
| Sensory block duration | 405.33±39.28 | 866.33±82.73 | -27.57 | .001 |
| Motor block onset | 12.60±2.50 | 22.27±2.96 | -13.67 | .001 |
| Motor block duration | 381.67±38.24 | 1060.00±96.13 | -35.91 | .001 |
| Duration of analgesia | 470.0±46.24 | 1171.67±96.74 | -35.84 | .001 |
| Heart Rate (Beats per minute) | Groups | t value | p-value | |
| A | B | |||
| Baseline | 82.07±12.98 | 83.20±11.63 | -.356 | .723 |
| 0 min | 86.07±12.13 | 86.73±11.61 | -.217 | .829 |
| 5 min | 88.93±12.15 | 89.13±11.40 | -.066 | .948 |
| 10 min | 89.60±11.67 | 92.07±10.14 | -.874 | .386 |
| 15 min | 87.77±11.54 | 90.60±9.86 | -1.02 | .311 |
| 30 min | 85.67±10.90 | 89.33±9.43 | -1.39 | .169 |
| 60 min | 83.93±11.68 | 87.60±9.44 | -1.34 | .186 |
| 90 min | 83.20±10.73 | 85.93±9.46 | -1.05 | .300 |
| 120 min | 80.43±10.88 | 83.20±8.94 | -1.08 | .286 |
| 150 min | 80.67±10.70 | 80.93±8.53 | -.107 | .915 |
| 180 min | 79.53±10.58 | 78.53±8.85 | .397 | .693 |
| 6 hours | 76.73±10.74 | 76.07±8.94 | .261 | .795 |
| 12 hours | 75.20±11.05 | 75.20±8.84 | .000 | 1.00 |
| 24 hours | 74.27±11.27 | 74.40±7.76 | -.053 | .958 |
| Systolic Blood Pressure (mmHg) | Groups | t value | p-value | |
| A | B | |||
| Baseline | 124.67±9.18 | 124.87±7.89 | -.091 | .928 |
| 0 min | 125.27±8.92 | 124.87±7.87 | .184 | .855 |
| 5 min | 125.33±9.10 | 124.33±7.52 | .464 | .644 |
| 10 min | 125.06±8.97 | 124.13±7.06 | .448 | .656 |
| 15 min | 125.13±8.33 | 123.13±6.84 | 1.02 | .314 |
| 30 min | 124.67±8.16 | 121.07±6.10 | 1.94 | .058 |
| 60 min | 124.07±6.99 | 121.20±6.14 | 1.69 | .097 |
| 90 min | 123.13±6.82 | 120.07±6.02 | 1.85 | .070 |
| 120 min | 121.93±7.67 | 119.93±6.02 | 1.12 | .266 |
| 150 min | 120.27±6.76 | 119.00±6.19 | .757 | .452 |
| 180 min | 118.80±6.21 | 118.13±6.45 | .408 | .685 |
| 6 hours | 118.07±6.31 | 117.0±5.38 | .705 | .484 |
| 12 hours | 117.13±5.50 | 115.47±5.14 | 1.21 | .230 |
| 24 hours | 115.80±5.05 | 113.73±4.78 | 1.63 | .109 |
| Diastolic Blood pressure(mmHg) | Groups | t value | p-value | |
| A | B | |||
| Baseline | 81.27±8.04 | 78.07±8.52 | 1.50 | .140 |
| 0 min | 81.13±7.92 | 78.07±8.52 | 1.44 | .154 |
| 5 min | 81.27±7.89 | 77.87±8.39 | 1.62 | .111 |
| 10 min | 80.93±7.59 | 77.53±8.03 | 1.69 | .097 |
| 15 min | 80.87±7.38 | 77.13±7.67 | 1.92 | .060 |
| 30 min | 80.53±7.12 | 76.47±7.51 | 2.15 | .036 |
| 60 min | 79.93±7.13 | 76.33±7.54 | 1.90 | .062 |
| 90 min | 78.67±6.69 | 75.47±7.82 | 1.70 | .094 |
| 120 min | 78.13±6.45 | 74.73±7.78 | 1.84 | .071 |
| 150 min | 78.00±6.35 | 74.47±7.71 | 1.94 | .058 |
| 180 min | 77.20±6.49 | 73.20±7.64 | 2.19 | .033 |
| 6 hours | 76.60±6.22 | 72.93±7.93 | 1.99 | .051 |
| 12 hours | 76.47±6.66 | 72.33±7.45 | 2.27 | .027 |
| 24 hours | 75.47±7.29 | 71.60±7.36 | 2.04 | .046 |
| Spo2 (%) | Groups | t value | p-value | |
| A | B | |||
| Baseline | 98.43±1.16 | 98.53±1.07 | -.346 | .731 |
| 0 min | 98.47±1.17 | 98.43±1.01 | .119 | .906 |
| 5 min | 98.23±1.07 | 98.23±.858 | .000 | 1.00 |
| 10 min | 98.03±.858 | 98.07±.944 | -.136 | .892 |
| 15 min | 97.80±.925 | 97.87±1.01 | -.267 | .790 |
| 30 min | 97.73±.944 | 97.60±1.10 | .503 | .617 |
| 60 min | 97.57±1.16 | 97.37±1.07 | .694 | .491 |
| 90 min | 97.33±1.18 | 97.27±.944 | .241 | .810 |
| 120 min | 97.23±1.14 | 97.13±1.01 | .361 | .720 |
| 150 min | 97.27±1.17 | 97.10±1.03 | .585 | .561 |
| 180 min | 97.10±1.16 | 97.00±.947 | .367 | .715 |
| 6 hours | 97.10±1.13 | 96.90±.960 | .741 | .462 |
| 12 hours | 97.07±1.14 | 96.90±.922 | .621 | .537 |
| 24 hours | 97.33±1.35 | 97.10±1.27 | .690 | .493 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Nausea and vomiting management · Enhanced Recovery After Surgery
Introduction
Since Halstead introduced the first brachial plexus block using cocaine in 1884, the technique has significantly evolved from blind approaches to nerve stimulator-assisted and ultrasound-guided methods [1-4]. Brachial plexus blocks now serve as a reliable alternative to general anesthesia for upper limb surgeries, providing excellent perioperative analgesia, reducing hospital stays, lowering costs, and minimizing the side effects of general anesthesia [4-6].
Of the various approaches--interscalene, supraclavicular, infraclavicular, and axillary--the supraclavicular technique is widely preferred for surgeries at or below the elbow [7,8]. Often referred to as the “spinal of the arm,” it offers dense anesthesia with rapid onset and requires a smaller volume of anesthetic. It may be used alone or as an adjunct to general anesthesia to enhance perioperative pain control [9-12].
Ultrasound guidance has further improved the efficacy and safety of supraclavicular blocks, offering real-time visualization, precise drug deposition, faster onset, reduced anesthetic volume, and fewer complications such as pneumothorax. The use of echogenic needles enhances safety and accuracy [13-15].
To prolong the duration and quality of block, adjuvants like alpha-2 agonists (clonidine, dexmedetomidine), opioids (fentanyl, tramadol), and corticosteroids (dexamethasone) are often used. Levobupivacaine, a pure S(-)-enantiomer of bupivacaine, is preferred due to its favorable safety profile, particularly lower cardiotoxicity [8,16,17].
Dexamethasone, a synthetic corticosteroid with anti-inflammatory, analgesic, and antiemetic properties, is used via perineural or intravenous routes to enhance block duration. It may act via vasoconstriction, direct nerve membrane effects, and activation of inhibitory potassium channels [9,17-19]. Perineural dexamethasone has been shown to shorten the onset and prolong the duration of both sensory and motor blocks, as well as analgesia, with minimal adverse effects. Intravenous dexamethasone is also known to reduce postoperative pain, nausea, and vomiting [20]. The present study aims to compare the effects of intravenous versus perineural dexamethasone as an adjuvant to levobupivacaine in ultrasound-guided supraclavicular blocks for adult patients undergoing elective upper limb surgeries.
Materials and methods
Study design and setting
This was a prospective, randomized, double-blind, parallel-group, controlled study conducted at Sardar Vallabhbhai Patel Hospital affiliated with Lala Lajpat Rai Memorial Medical College, Meerut. The study duration was 18 months, from May 2023 to November 2024. Ethical clearance was obtained from the institutional ethics committee (SC-1-2024/4486), and all participants provided written informed consent prior to enrolment. The study is also registered with the Clinical Trials registry of India (CTRI/2025/02/080286).
Participants
Eligible participants were adults aged 18 to 60 years, of either sex, classified as American Society of Anaesthesiologists (ASA) physical status I or II [21], and scheduled for elective upper limb surgery under ultrasound-guided supraclavicular brachial plexus block (Figure 1). Inclusion also required a body mass index (BMI) between 18 and 24 kg/m². Exclusion criteria included refusal to participate, local infection at the injection site, coagulopathy, pregnancy, first-to-third degree heart block, peripheral neuropathy, or known allergy to local anesthetic agents.
CONSORT (Consolidated Standards of Reporting Trials) 2010 flow diagram depicting patient enrollment, randomization, allocation, follow-up, and analysis
Interventions
Patients were randomly assigned to one of two groups (n=30 each).
Group A (IV Dexamethasone Group)
Patients received 19 mL of 0.5% levobupivacaine with 1 mL of normal saline (total 20 mL) for a supraclavicular block, and 4 mg (1 mL) dexamethasone was administered intravenously.
Group B (Perineural Dexamethasone Group)
Patients received 19 mL of 0.5% levobupivacaine with 4 mg (1 mL) dexamethasone (total 20 mL) for the block, and 1 mL of intravenous normal saline.
Drug preparation was done by an independent anesthesiologist not involved in patient care or data collection. All blocks were performed under ultrasound guidance using standard sterile technique.
Outcomes
The primary outcomes were onset time and duration of sensory and motor block. The secondary outcomes included duration of postoperative analgesia (time to first rescue analgesic), hemodynamic changes (heart rate, mean arterial pressure, systolic and diastolic blood pressure), pain scores using the numeric rating scale (NRS) [22] and incidence of complications (e.g., drowsiness, nausea, vomiting, Horner’s syndrome, phrenic nerve palsy, pneumothorax, and signs of local anesthetic toxicity).
Block onset and duration were assessed using the pin-prick method [23] for sensory block (3-point scale) and the Modified Bromage scale [24] for motor block. Pain was assessed using NRS at 12 and 24-hour intervals postoperatively.
Sample size
A total of 60 participants were included, with 30 in each group. The sample size was based on previously published studies and calculated to achieve adequate precision of 95% confidence limits for the primary outcome variables.
Randomization and blinding
Randomization was performed using a computer-generated random number table. Allocation was concealed in sealed opaque envelopes. The anesthesiologist performing the block and the patient were both blinded to group allocation. A separate anesthesiologist not involved in data collection prepared the study drugs.
Data collection and monitoring
Baseline clinical data, vitals, and preoperative assessment (PAC) findings were recorded. Standard intraoperative and postoperative monitoring was conducted at specific time intervals: 0, 5, 10, 15, 30, 60, 90, 120, 150, and 180 minutes, and at 6, 12, and 24 hours. Complications, if any, were recorded and managed accordingly.
Statistical analysis
Data were entered in Microsoft Excel. Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, New York, USA). Descriptive statistics, such as mean, standard deviation, median (IQR), frequencies, and percentages, were used. Independent t-tests or chi-square tests were applied for between-group comparisons depending on the data type. A p-value of < 0.05 was considered statistically significant.
Results
There were no significant differences between Groups A and B in age (p=0.648), sex (p=1.000), BMI (p=0.818), or ASA grade (p=1.000), indicating well-matched baseline characteristics (Table 1).
Table 1: Comparison of baseline characteristics between groupsValues are presented as mean ± standard deviation or number (%).BMI: body mass index; ASA: American Society of Anaesthesiologistsp-values were calculated using the Independent t-test for continuous variables and the chi-square test for categorical variables.“–” indicates not applicable. A p-value of <0.05 is considered significant.
The study found a comparable surgery duration (p=0.967), but Group B had significantly slower onset and prolonged duration of sensory and motor blocks, and longer analgesia (all p=0.001) (Table 2). The heart rate remained comparable between Groups A and B at all measured time intervals from baseline to 24 hours postoperatively, with no statistically significant differences (all p > 0.05) (Table 3).
Table 2: Comparison of duration of surgery, sensory and motor block characteristics, and duration of analgesia between Groups A and BValues are presented as mean ± standard deviation.min: minutesp-values were calculated using the independent t-test. A p-value of <0.05 is considered significant.
Table 3: Comparison of heart rate (beats per minute) at different time intervals between Groups A and BValues are presented as mean ± standard deviation.HR: heart rate; bpm: beats per minutep-values were calculated using the independent t-test. A p-value of <0.05 is considered significant.
The comparison of systolic blood pressure (SBP) between Groups A and B across multiple time intervals showed no statistically significant differences at any time point (p > 0.05). Both groups had nearly identical baseline SBP (124.67±9.18 vs. 124.87±7.89 mmHg; p = 0.928). Slightly higher SBP values were observed in Group A at 30, 60, and 90 minutes, with p-values approaching significance (0.058, 0.097, and 0.070, respectively), suggesting a trend but not reaching statistical significance. Overall, SBP remained comparable between the two groups throughout the 24-hour period (Table 4).
Table 4: Comparison of systolic blood pressure (mmHg) at different time intervals between Groups A and BValues are presented as mean ± standard deviation.SBP: systolic blood pressurep-values were calculated using the Independent t-test. A p-value <0.05 is considered significant.
The diastolic blood pressure (DBP) was consistently higher in Group A than in Group B at all time points. Statistically significant differences were observed at 30 min (p=0.036), 180 min (p=0.033), 12 hours (p=0.027), and 24 hours (p=0.046). Several other intervals showed near-significant trends. Overall, Group A maintained a higher DBP profile compared to Group B over 24 hours (Table 5). Table 6 shows that the oxygen saturation (SpO₂) levels remained comparable between Groups A and B at all time intervals, with no statistically significant differences (p > 0.05). Both groups maintained stable SpO₂ values close to 97-98% throughout the 24-hour period (Table 6).
Table 5: Comparison of diastolic blood pressure (mmHg) at different time intervals between Groups A and BValues are presented as mean ± standard deviation.DBP: diastolic blood pressurep-values were calculated using the Independent t-test. A p-value of <0.05 is considered as significant.
Table 6: Comparison of oxygen saturation (SpO2, %) at different time intervals between Groups A and BValues are presented as mean ± standard deviation.SpO₂: peripheral capillary oxygen saturationp-values were calculated using the independent t-test. A p-value of <0.05 is considered significant.
A comparison of NRS scores at 12 and 24 hours between Groups A and B. Group A exhibited a noticeable increase in NRS scores from 3.23 at 12 hours to 3.83 at 24 hours, indicating a rise in perceived pain over time. In contrast, Group B maintained relatively stable scores, increasing only slightly from 3.00 to 3.10. This suggests that Group B experienced better pain control over the 24-hour period compared to Group A (Figure 2).
Comparison of NRS at different time intervals between groupsNRS: numeric rating scale
No cases of nausea, vomiting, tachycardia, bradycardia, hypotension, hypertension, or respiratory depression were observed in either group. This indicates that both interventions were well-tolerated, with no reported adverse events or hemodynamic instability in either group.
In our study, Group B demonstrated significantly prolonged sensory (866.33±82.73 vs. 405.33±39.28 min) and motor block durations (1060.00±96.13 vs. 381.67±38.24 min), extended analgesia duration (1171.67±96.74 vs. 470.0±46.24 min), and lower postoperative pain scores at 12 and 24 hours compared to Group A, with p = 0.001 in all parameters. These findings suggest the enhanced efficacy of the intervention used in Group B in terms of nerve blockade and postoperative analgesia, without compromising safety.
Discussion
Ultrasound-guided supraclavicular brachial plexus block is a preferred regional anesthesia technique for upper limb surgeries because it provides dense anesthesia with rapid onset and prolonged postoperative analgesia. To further enhance block duration and quality, various adjuvants, such as α-2 agonists, opioids, and corticosteroids, have been explored, with dexamethasone emerging as one of the most effective options. In the present prospective, randomized, double-blind study comparing intravenous and perineural dexamethasone as adjuvants to levobupivacaine, we observed that perineural administration significantly shortened the onset and markedly prolonged the duration of both sensory and motor block. It also extended postoperative analgesia and maintained lower pain scores at 12 and 24 hours without compromising hemodynamic stability or increasing adverse effects. These results clearly establish the superiority of perineural dexamethasone over intravenous administration in optimizing block characteristics and postoperative pain control.
The sensory and motor block durations were shorter than those reported by Veena G et al. (2021) [25], possibly due to variations in drug dosage, adjuvant use, or patient characteristics. In contrast, our findings showed a stronger effect than Bisui B et al. (2017) [4], who reported shorter block durations, likely due to different anesthetic agents or the absence of adjuvants. Rao MV Kameswar et al. (2019) [26] also reported similar prolongation with adjuvant use, aligning with our findings.
The prolonged analgesia in Group B is supported by Veena G et al. [25], Rao MV Kameswar et al. [26], and further corroborated by Baeriswyl M et al. (2017) [27] and Chong A M et al. (2017) [5], who demonstrated the efficacy of perineural dexamethasone in prolonging pain relief. Our lower pain scores at 12 and 24 hours are consistent with Veena G et al. [25] and Vasconcelos M M et al. (2020) [28], highlighting sustained analgesia and reduced need for rescue medication in Group B.
Hemodynamic parameters remained stable across groups, differing from Prathibhan S et al. (2024) [29] and Parthasarathy P et al. (2018) [6], possibly due to differences in monitoring protocols or anesthetic regimens. Importantly, no significant complications were observed, confirming the safety of the Group B intervention, consistent with findings from Baeriswyl M et al. [27] and Chong A M et al. [5].
Our study's strengths include well-balanced baseline characteristics, comprehensive assessment of anesthesia parameters, objective pain scoring, and consistent findings with previous studies [4,5,25-27]. Overall, the results provide strong evidence supporting the efficacy and safety of the Group B intervention for enhanced postoperative pain management.
Limitations
The study was limited by a relatively small sample size and the single-center design, which may restrict generalizability. Only short-term postoperative outcomes were assessed, without evaluation of long-term analgesic efficacy. Subjective variation in pain perception and operator-dependent factors in performing ultrasound-guided blocks could also have influenced the results.
Conclusions
Both intravenous and perineural dexamethasone effectively enhanced the quality and duration of ultrasound-guided supraclavicular brachial plexus blocks when combined with levobupivacaine. However, perineural dexamethasone resulted in a significantly slower onset and longer duration of sensory and motor block, as well as prolonged postoperative analgesia. Hemodynamic stability was maintained in both groups, and no major complications were observed. Perineural administration of dexamethasone is recommended as the preferred adjuvant in supraclavicular blocks to maximize block effectiveness and analgesia duration. Further studies with larger sample sizes and longer follow-up are suggested to confirm safety and explore the potential of combining dexamethasone with other adjuvants for enhanced perioperative pain control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hemostasis Wylie & Churchill-Davidson’s A Practice of Anaesthesia, 7th ed Healy T Knight P 185202 Boca Raton (FL)CRC Press 2003
- 2Supraclavicular brachial plexus blocks: review and current practice Acta Anaesthesiol Belg Vermeylen K Engelen S Sermeus L Soetens F Van de Velde M 1521632012 https://pubmed.ncbi.nlm.nih.gov/22783706/22783706 · pubmed ↗
- 3Adjuvants to local anesthetics: current understanding and future trends World J Clin Cases Swain A Nag DS Sahu S Samaddar DP 307323520172886830310.12998/wjcc.v 5.i 8.307PMC 5561500 · doi ↗ · pubmed ↗
- 4Effect of locally administered dexmedetomidine as adjuvant to levobupivacaine in supraclavicular brachial plexus block: double-blind controlled study Anesth Essays Res Bisui B Samanta S Ghoshmaulik S Banerjee A Ghosh TR Sarkar S 9819861120172928486010.4103/aer.AER_55_17PMC 5735499 · doi ↗ · pubmed ↗
- 5Perineural versus intravenous dexamethasone as an adjuvant for peripheral nerve blocks: a systematic review and meta-analysis Reg Anesth Pain Med Chong MA Berbenetz NM Lin C Singh S 3193264220172825252310.1097/AAP.0000000000000571 · doi ↗ · pubmed ↗
- 6The effect of single-dose intravenous dexamethasone on postoperative pain and postoperative nausea and vomiting in patients undergoing surgery under spinal anesthesia. A double-blind randomized clinical study Anesth Essays Res Parthasarathy P Babu K Raghavendra Rao RS Raghuram S 3133171220182996258910.4103/aer.AER_159_17PMC 6020567 · doi ↗ · pubmed ↗
- 7Corticosteroids in the treatment of acute asthma Ann Thorac Med Alangari AA 187192920142527623610.4103/1817-1737.140120 PMC 4166064 · doi ↗ · pubmed ↗
- 8Assessment of pain Br J Anaesth Breivik H Borchgrevink PC Allen SM 172410120081848724510.1093/bja/aen 103 · doi ↗ · pubmed ↗