Endoscopic Prelacrimal Approach for the Surgical Management of a Late Silicone Foreign Body and an Odontogenic Maxillary Cyst: A Case Report
Badr Soudi, Amine Benfaida, Florian Rivieccio, Pierre Louis Chiche, Hassan El Edghiri

TL;DR
A new endoscopic surgical approach successfully removed hard-to-reach foreign bodies and cysts in the maxillary sinus, offering a safe and effective treatment option.
Contribution
The paper introduces the endoscopic prelacrimal recess approach for managing difficult maxillary sinus pathologies.
Findings
EPLA enabled complete removal of a retained silicone fragment and an odontogenic cyst in two patients.
The approach preserved critical anatomical structures without complications.
Postoperative outcomes showed complete symptom resolution in both cases.
Abstract
Foreign bodies and odontogenic lesions of the maxillary sinus can lead to chronic rhinosinusitis, particularly when located in compartments that are difficult to access surgically. We report two cases managed using the endoscopic prelacrimal recess approach (EPLA). The first case involved a 76-year-old woman presenting with chronic facial pain and purulent discharge caused by a retained silicone fragment following bilateral inferior turbinectomy performed 20 years earlier. The second case concerned a 28-year-old woman with recurrent left maxillary sinusitis secondary to a 2.1-cm pericoronal cyst associated with an ectopic tooth. In both patients, EPLA allowed direct access to the anterior and inferior maxillary sinus, enabling complete lesion removal while preserving the nasolacrimal duct, natural ostium, and inferior turbinate. Postoperative outcomes were favorable, with complete…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
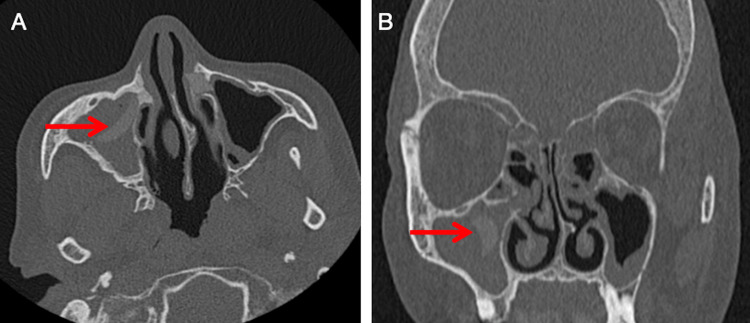 Figure 1
Figure 1 Figure 2
Figure 2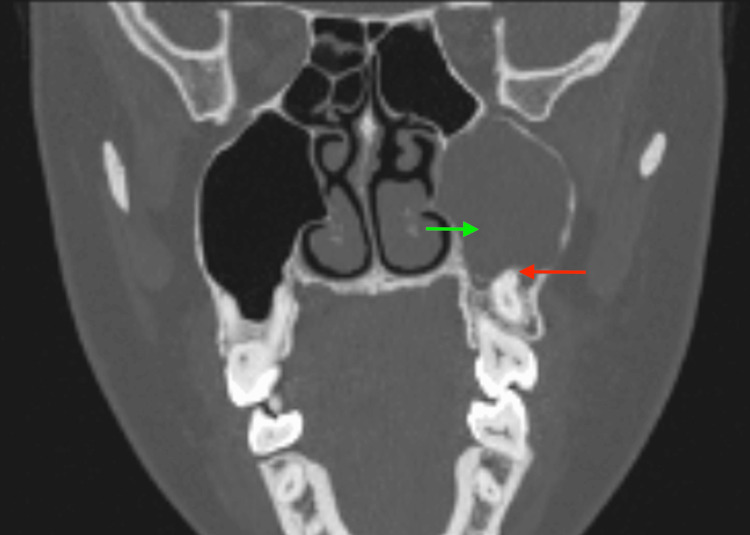 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSinusitis and nasal conditions · Nasolacrimal Duct Obstruction Treatments · Head and Neck Surgical Oncology
Introduction
Foreign material or odontogenic lesions within the maxillary sinus can lead to persistent rhinosinusitis and secondary infection, particularly when located in anatomically difficult-to-access compartments. Several surgical approaches have historically been used to address such lesions. The Caldwell-Luc procedure, although once the standard, is associated with significant postoperative morbidity, including facial numbness, oroantral fistula, and chronic pain [1,2]. The middle meatal antrostomy (MMA), as part of functional endoscopic sinus surgery, reduces morbidity but provides limited access to the anterior and inferior regions of the maxillary sinus [3]. The modified Denker approach offers broader exposure of the anterior maxillary sinus but may be associated with increased tissue disruption and altered nasal physiology.
In 2010, Nakamaru et al. introduced the endoscopic prelacrimal recess approach (EPLA) to overcome these limitations [4]. EPLA provides direct access to the anteroinferior maxillary sinus while preserving key structures, including the inferior turbinate and nasolacrimal duct. This approach has since been applied successfully for benign tumors, cysts, and foreign bodies [5,6]. Compared with other techniques, EPLA allows for targeted exposure with minimal disruption of nasal anatomy, though larger studies are required to fully establish its comparative efficacy.
In this report, we assessed the feasibility and outcomes of EPLA in two distinct cases: a chronic silicone foreign body and an odontogenic cyst with an ectopic tooth, lesions that might otherwise require more invasive external approaches.
Case presentation
Case 1: Silicone foreign body
A 76-year-old woman presented with chronic right maxillary sinusitis and facial pain. Her surgical history included a bilateral partial inferior turbinectomy performed 20 years earlier. She also had diabetes, hypercholesterolemia, and coronary artery disease treated with a stent.
Endoscopic examination revealed purulent discharge and bilateral synechiae, more pronounced on the right side. Computed tomography demonstrated complete right maxillary sinus opacification with a well-defined hyperdense foreign body along the lateral wall, consistent with a non-metallic material measuring approximately 15 mm (Figure 1, axial and coronal views).
Referenced in Case 1, Diagnostic Assessment section - axial (A) and coronal computed tomography (B) scans showing a hyperdense foreign body (red arrow) in the right maxillary sinus.
Under general anesthesia, we performed the EPLA. A vertical incision was made anterior to the uncinate process, and the inferior turbinate-nasolacrimal duct (IT-NLD) flap was elevated to expose the anteromedial maxillary sinus. The silicone fragment was dissected and removed en bloc (Figure 2). The flap was repositioned and sutured with absorbable material. No intraoperative images are available for this case.
Referenced in Case 1, Therapeutic Intervention section - silicone fragment removed en bloc during surgery (red arrow).
Histopathologic examination revealed chronically inflamed mucosa without granulomatous reaction. The patient was discharged on postoperative Day 1. At six weeks and three months, she reported complete pain relief and no recurrent discharge.
Case 2: Odontogenic cyst with ectopic tooth
A 28-year-old woman presented with recurrent left maxillary sinusitis and dental pain refractory to antibiotics. Nasoendoscopy revealed mucopurulent drainage from the left middle meatus. CT imaging identified a 2.1-cm cyst containing an ectopic tooth in the left maxillary sinus near the natural ostium (Figure 3, coronal view).
Coronal computed tomography scan showing the pericoronal cyst (green arrow) with an ectopic tooth (red arrow).
Under general anesthesia, we performed EPLA. After an incision anterior to the uncinate process, the IT-NLD flap was raised to access the prelacrimal recess. The cyst and ectopic tooth were removed en bloc under endoscopic control, and the flap was replaced and sutured. Consultation with an oral surgeon was obtained before the procedure to ensure comprehensive management. No intraoperative images are available for this case.
Histological examination confirmed a cyst lined by non-keratinized squamous epithelium with mild chronic inflammation. The patient was discharged the same day. At six months, she remained symptom-free with complete mucosal healing.
Discussion
Chronic sinusitis secondary to retained foreign material or odontogenic pathology remains a surgical challenge. In the first case, the retained silicone fragment likely originated from previous partial inferior turbinectomy material and induced chronic inflammation years later. Synthetic material within the sinus can perpetuate bacterial colonization and lead to mucosal fibrosis [7-9]. Awareness of such iatrogenic causes is crucial to prevent long-term complications.
Odontogenic disease accounts for up to 12% of maxillary sinus pathology, whereas ectopic teeth within the sinus remain exceptional [10]. These cystic or dental-related lesions can obstruct normal sinus drainage and sustain recurrent infections. Collaboration between otolaryngologists and oral surgeons is essential to ensure complete removal and reduce the risk of recurrence, as demonstrated in the second case.
Several surgical approaches are available for the management of maxillary sinus pathology. The Caldwell-Luc procedure, historically the standard, provides wide access but is associated with postoperative complications such as facial numbness, oroantral fistula, and prolonged recovery [1,2]. MMA reduces morbidity but offers limited visualization of the anterior and inferior sinus compartments [3]. The modified Denker approach allows extensive exposure of the anterolateral maxillary sinus and floor, yet it is more invasive and may carry a higher risk of facial swelling and dental complications [11].
The EPLA broadens access beyond the limitations of MMA while avoiding the morbidity of more invasive techniques. By entering through the prelacrimal recess and elevating the inferior turbinate-nasolacrimal duct flap, the surgeon achieves direct visualization of the anterior and inferior maxillary sinus. This approach preserves physiologic drainage pathways, reduces postoperative discomfort, and minimizes complications such as facial numbness, oroantral fistula, and chronic pain [2,5]. In both patients, EPLA allowed complete visualization and en bloc excision under controlled endoscopic vision.
It is important to note that this report includes only two cases, which represent a limitation. While the outcomes were favorable, larger case series or comparative studies are necessary to further assess the safety, efficacy, and relative advantages of EPLA compared with other approaches.
Overall, EPLA can be considered a minimally invasive option for selected maxillary sinus lesions located in anatomically challenging compartments, particularly when preservation of key structures is desired.
Conclusions
We report two uncommon cases of maxillary sinus pathology successfully managed using the EPLA: a silicone foreign body of uncertain origin and a pericoronal cyst associated with an ectopic tooth. Both patients experienced complete symptom resolution. EPLA allows excellent exposure of the anterior and inferior maxillary compartments while preserving the nasolacrimal duct, natural ostium, and inferior turbinate. Reported complications are rare and usually transient.
Close collaboration between ENT and dental specialists is essential to optimize the management of complex odontogenic sinus disease. It is important to note that this report describes only two cases, which represents a limitation. While EPLA was effective in these cases, larger case series or comparative studies are necessary to fully evaluate its safety, efficacy, and potential advantages relative to alternative surgical approaches such as the modified Denker or Caldwell-Luc procedures.
Overall, EPLA can be considered a reliable and minimally invasive option for selected maxillary sinus pathologies, particularly in anatomically challenging compartments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Endoscopic surgical treatment of chronic maxillary sinusitis of dental origin J Oral Maxillofac Surg Costa F Emanuelli E Robiony M Zerman N Polini F Politi M 2232286520071723692510.1016/j.joms.2005.11.109 · doi ↗ · pubmed ↗
- 2Complications of the Caldwell-Luc operation and how to avoid them Aust N Z J Surg Low WK 582584651995766180010.1111/j.1445-2197.1995.tb 01700.x · doi ↗ · pubmed ↗
- 3Functional endoscopic sinus surgery. Technique Arch Otolaryngol Kennedy DW 6436491111985403813610.1001/archotol.1985.00800120037003 · doi ↗ · pubmed ↗
- 4Preservation of the nasolacrimal duct during endoscopic medial maxillectomy for sinonasal inverted papilloma Rhinology Nakamaru Y Furuta Y Takagi D Oridate N Fukuda S 4524564820102144208410.4193/Rhino 10.015 · doi ↗ · pubmed ↗
- 5Comparison between endoscopic prelacrimal medial maxillectomy and Caldwell-Luc approach for benign maxillary sinus tumors Clin Exp Otorhinolaryngol Lee JJ Ahmad ZAM Kim D 2872931220193045860310.21053/ceo.2018.01165 PMC 6635712 · doi ↗ · pubmed ↗
- 6Clinical outcome of endonasal endoscopic prelacrimal approach in managing different maxillary pathologies Peer J Lin YH Chen WC 08202010.7717/peerj.8331 PMC 694411731915590 · doi ↗ · pubmed ↗
- 7Chronic maxillary sinusitis of dental origin: is external surgical approach mandatory?Laryngoscope Lopatin AS Sysolyatin SP Sysolyatin PG Melnikov MN 1056105911220021216027310.1097/00005537-200206000-00022 · doi ↗ · pubmed ↗
- 8Meta-analysis of the etiology of odontogenic maxillary sinusitis Med Oral Patol Oral Cir Bucal Arias-Irimia O Barona-Dorado C Santos-Marino JA Martínez-Rodriguez N Martínez-González JM 0315201010.4317/medoral.15.e 7019767698 · doi ↗ · pubmed ↗