BRCA2 Reversion Mutation after Neoadjuvant Dose-Dense EC and Dose-Dense Paclitaxel in Triple-Negative Breast Cancer: A Case Report and Literature Review
Hajime Hikino, Asa Otani, Yoshinari Makino

TL;DR
A patient with BRCA2-mutated breast cancer developed a reversion mutation after chemotherapy, leading to early recurrence, suggesting the need for monitoring BRCA status.
Contribution
Reports a rare case of BRCA2 reversion mutation emerging without PARPi or platinum therapy, highlighting its clinical implications.
Findings
BRCA2 reversion mutation was detected in residual tumor after chemotherapy, restoring the open reading frame.
The patient experienced early systemic recurrence, including leptomeningeal metastasis, 7 months post-surgery.
The case suggests reversion mutations can occur early, independent of PARPi or platinum exposure.
Abstract
BRCA reversion mutations are known mechanisms of acquired resistance to poly (ADP-ribose) polymerase inhibitors (PARPis) and platinum agents. However, their clinical emergence without such therapies is rarely reported. We describe a 44-year-old woman with early-stage triple-negative breast cancer carrying a germline BRCA2 mutation who developed a BRCA2 reversion mutation after neoadjuvant dose-dense epirubicin and cyclophosphamide (EC) followed by dose-dense paclitaxel, without prior PARPi or platinum exposure. She underwent modified radical mastectomy and achieved a good pathological response; however, she developed early systemic recurrence, including leptomeningeal metastasis, 7 months postoperatively. Comprehensive genomic profiling of the residual breast tumor revealed a BRCA2 reversion mutation (allele frequency: 6.7%) that restored the open reading frame. We speculate that the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
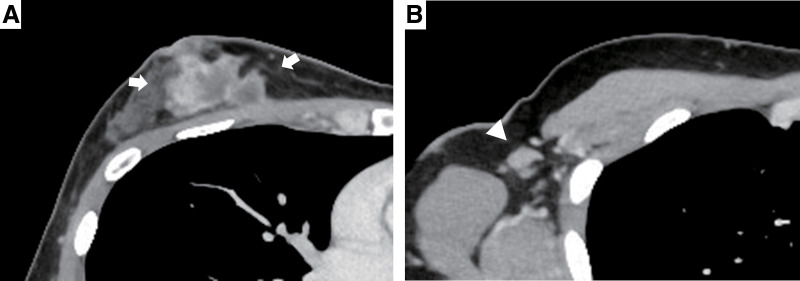 Fig. 1
Fig. 1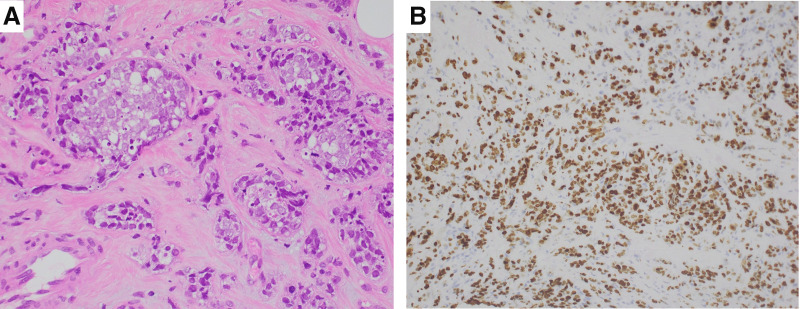 Fig. 2
Fig. 2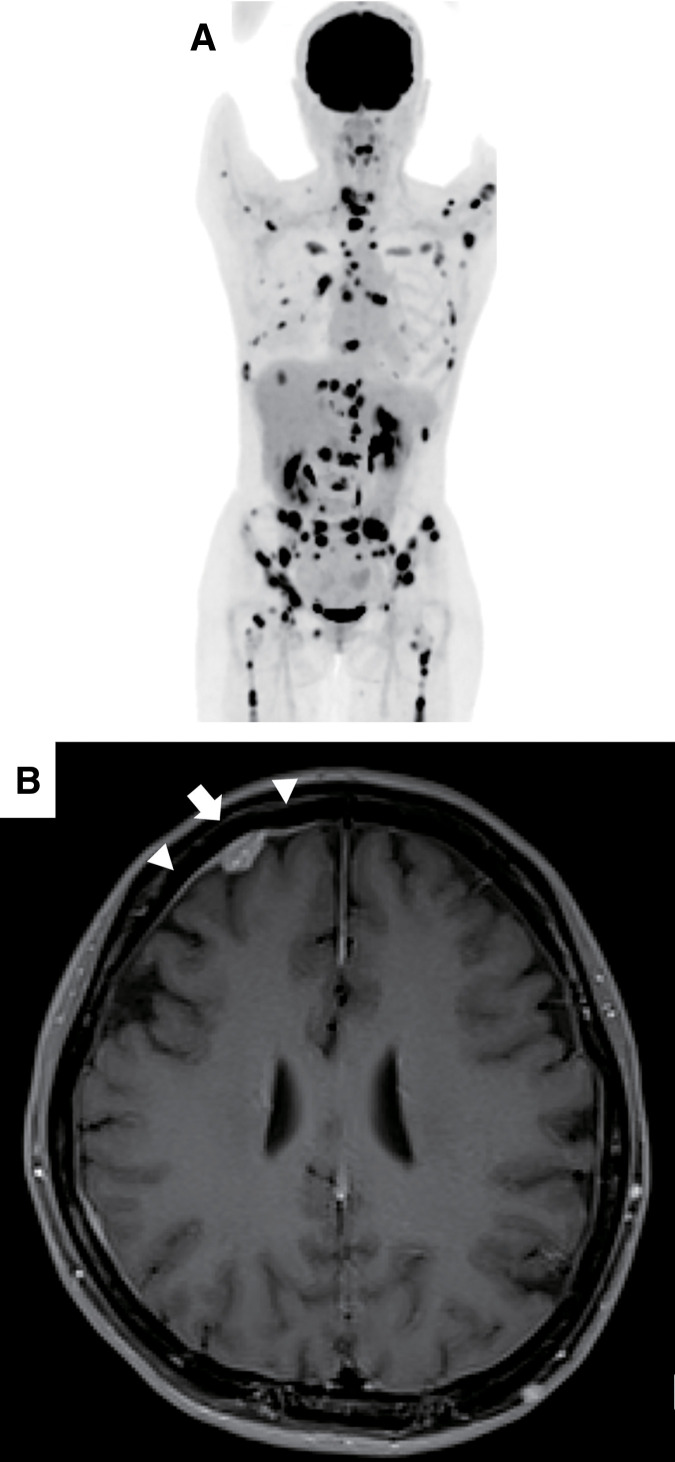 Fig. 3
Fig. 3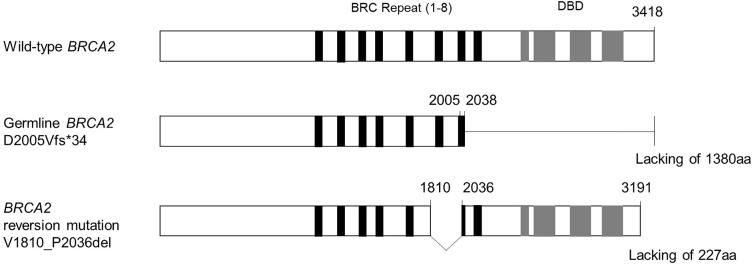 Fig. 4
Fig. 4| Author | Year | Cancer type | Status | Deleterious mutation | CGP specimen | Prior systemic therapies |
|---|---|---|---|---|---|---|
| Nakamura et al. | 2024 | Pancreas | Metastasis |
| Liquid | Non-platinum-based chemotherapy |
| Carneiro et al. | 2018 | Prostate | Metastasis |
| Liquid | Taxane, mitoxantrone, radium-223 |
| Vidula et al. | 2020 | Breast | Metastasis |
| Liquid | ET, capecitabine, everolimus, paclitaxel, eribulin, gemcitabine, mitoxantrone, vinorelbine |
| Prostate | Metastasis |
| Liquid | ADT, docetaxel, enzalutamide, abiraterone acetate, cabazitaxel, mitoxantrone | ||
| Murciano-Goroff et al. | 2022 | Breast | Primary |
| Tumor | Doxorubicin, cyclophosphamide, docetaxel, paclitaxel |
| Present case | 2025 | Breast | Primary |
| Tumor | Epirubicin, cyclophosphamide, paclitaxel |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · PARP inhibition in cancer therapy · Breast Cancer Treatment Studies
Abbreviations
cfDNA cell-free DNA CGP comprehensive genomic profiling EC epirubicin and cyclophosphamide gBRCA germline BRCA PARPi poly (ADP-ribose) polymerase inhibitor TNBC triple-negative breast cancer
INTRODUCTION
In Japan, approximately 4.2% of unselected breast cancers are reported to possess germline BRCA1 or BRCA2 mutations.^1)^ These mutations impair homologous recombination repair, rendering tumors sensitive to PARPis and platinum agents through synthetic lethality.^2)^ However, resistance can develop due to secondary reversion mutations that restore BRCA function.^3,4)^
Reversion mutations typically arise after exposure to PARPi or platinum agents. Here, we present a rare case of a gBRCA2-mutated TNBC patient who developed a BRCA2 reversion mutation after neoadjuvant chemotherapy with dose-dense EC and dose-dense paclitaxel, without exposure to PARPi or platinum agents. This case highlights the possibility of spontaneous reversion mutations early in the clinical course and their potential clinical significance.
CASE PRESENTATION
A 44-year-old woman presented with a 4.3 × 4.3-cm mass in the upper-inner quadrant of the right breast. She had no significant medical history but reported a family history of ovarian cancer (paternal grandmother) and pancreatic cancer (paternal uncle). A CT revealed a contrast-enhancing breast mass with 3 axillary lymphadenopathies (Fig. 1). Core needle biopsy showed high-grade invasive ductal carcinoma, negative for estrogen receptor, progesterone receptor, and HER2, with Ki-67 expression of 90% (Fig. 2). Genetic testing (BRACAnalysis; Myriad Genetics, Salt Lake City, UT, USA) identified a pathogenic gBRCA2 c.6014_6017del (p.D2005Vfs*34) mutation. The clinical stage was cT2N1M0 (Stage IIB).
Contrast-enhanced CT images at presentation revealed a 4.3 × 4.3-cm tumor in the upper-inner quadrant of the right breast (A, arrows), with enlarged axillary lymph nodes (B, arrowhead).
Photomicrographs of the core needle biopsy specimen. (A) Tumor cells showed marked nuclear atypia and mitoses infiltrating surrounding tissue in alveolar and tubular patterns (H&E stain, ×400). (B) MIB-1 labeling index was 90% (×200).H&E, hematoxylin and eosin; MIB-1, molecular immunology Borstel-1
She received neoadjuvant chemotherapy using 4 cycles of dose-dense EC (epirubicin 90 mg/m^2^ and cyclophosphamide 600 mg/m^2^ every 2 weeks), followed by 4 cycles of dose-dense paclitaxel (175 mg/m^2^ every 2 weeks), with pegfilgrastim 3.6 mg per cycle. She then underwent a right modified radical mastectomy and contralateral risk-reducing mastectomy. Pathology revealed a 7-mm residual invasive carcinoma (triple-negative, Ki-67 73%). PD-L1 was negative on immunohistochemistry (PD-L1 antibody clone SP142; Ventana Medical Systems, Tucson, AZ, USA; PD-L1 antibody clone 22C3 pharmDx; Dako, Glostrup, Denmark). No nodal involvement was noted, and pathological staging was ypT1bN0M0 (ypStage IA). The left breast was free of malignancy.
Adjuvant therapy included post-mastectomy radiotherapy (50 Gy in 25 fractions) to the right chest wall and supraclavicular area, and capecitabine (1250 mg/m^2^ twice daily on days 1–14 every 3 weeks). At 7 months post-surgery, during the fifth cycle of capecitabine, she developed widespread metastases to bone, liver, lung, lymph nodes, and leptomeninges, confirmed by PET (Fig. 3A) and brain/spine MRI (Fig. 3B). Cerebrospinal fluid cytology confirmed leptomeningeal involvement. Rapid clinical deterioration precluded PARPi therapy; weekly paclitaxel (90 mg/m^2^) plus biweekly bevacizumab (10 mg/kg) and zoledronic acid were initiated.
(A) 18F-FDG PET/CT showed abnormal uptakes in bone, liver, lung, and distant lymph nodes, indicating multiple systemic recurrences. (B) Gadolinium-enhanced T1-weighted MRI of the brain revealed a nodular enhancing lesion (arrow) and leptomeningeal involvement (arrowheads) in the right frontal lobe, consistent with carcinomatous meningitis.
CGP (FoundationONE; Foundation Medicine, Boston, MA, USA) of the residual primary tumor, with an estimated tumor content of approximately 20%, identified the original BRCA2 frameshift mutation (allele frequency: 44.8%) and a BRCA2 reversion mutation c.5429_6109del681 (p.V1810_P2036del; allele frequency: 6.7%) that restored the reading frame (Fig. 4). Additional mutations included PIK3CA c.1637A>G (p.Q546R), CTNNA1 c.1256_1265del (p.Y419fs*9), and low tumor mutational burden.
Illustration of the wild-type BRCA2, the germline frameshift mutation, and the BRCA2 reversion mutation. The reversion mutation encompassed the frameshift site and restored an open reading frame, resulting in a protein of 3191 amino acids lacking 227 residues.aa, amino acid; DBD, DNA-binding domain
The patient’s general condition was significantly compromised, leading to her death a month later (11 months after surgery).
DISCUSSION
We present a rare case of a BRCA2 reversion mutation occurring after neoadjuvant chemotherapy with dose-dense EC and dose-dense paclitaxel, without prior PARPi or platinum agents. In this case, the original germline BRCA2 mutation was a frameshift deletion at positions c.6014–6017, resulting in the loss of BRCA2 function. After neoadjuvant chemotherapy, a secondary large in-frame deletion (c.5429–6109del) was identified, which encompassed and removed the region containing the original frameshift mutation. As a result, the open reading frame of BRCA2 was restored, potentially allowing partial recovery of homologous recombination function. This mechanism is well documented in PARPi and platinum resistance.^5,6)^ The variant allele frequency of the BRCA2 reversion mutation was 6.7%. Given the estimated tumor content of approximately 20% in the analyzed tissue, this finding suggests that the reversion mutation was present in a minor to intermediate subclonal tumor population.
Although reversion mutations are known to occur under intensive therapeutic selection pressure from PARPi or platinum agents, the precise mechanism and prevalence of reversion mutations remain unclear.^5,7,8)^ We performed a literature search in the PubMed database using the words “BRCA,” “reversion,” “mutation,” and “secondary mutation”. We excluded data that did not describe the clinical course of the disease. A total of 171 cases were reported, with a predominance of BRCA2 (121 cases) compared with BRCA1 (50 cases). In BRCA2-mutated tumors, reversion events often involve large deletions within exon 11 encoding the BRC repeat domain, where partial BRCA2 function may be retained. This characteristic may contribute to the higher frequency of reversion mutations observed in BRCA2.^5,9)^ However, the precise molecular mechanisms underlying this tendency remain to be fully elucidated. By cancer type, 60 were ovarian, 59 prostate, 35 breast, 14 pancreatic, 1 gallbladder, 1 esophageal, and 1 non-small cell lung cancer. Only 5 of 171 cases (2.9%) occurred without prior PARPi or platinum exposure, with 4 detected by cfDNA (Table 1).^7,10–12)^ In these cases, patients had typically received intensive chemotherapy including DNA cross-linking agents such as cyclophosphamide, which may exert similar selection pressure.^13)^
Reversion mutations are generally rare stochastic events that usually arise in advanced cancers with high genomic instability.^14)^ However, our case is unique in that the mutation was detected in residual tumor after neoadjuvant therapy for early-stage disease, suggesting that a small clone harboring the reversion mutation may have pre-existed or been induced early during chemotherapy. Given the elevated genomic instability associated with homologous recombination deficiency in gBRCA-mutated TNBC,^15)^ spontaneous reversion may occur more readily in this context. Notably, the patient experienced rapid recurrence and died of the disease, but whether BRCA reversion mutations directly increase intrinsic tumor aggressiveness remains uncertain. Recognition of this phenomenon is critical for treatment decisions and for developing strategies to overcome therapeutic resistance.
This study has limitations. We did not use PARPi in either the adjuvant or metastatic setting. Adjuvant olaparib has shown significant overall survival benefit in TNBC patients with gBRCA mutations and residual disease after intensive neoadjuvant therapy.^16)^ At the time of treatment, adjuvant PARPi was not yet approved in Japan for gBRCA-mutated breast cancer. In the metastatic setting, the presence of a reversion mutation raised concern for intrinsic PARPi resistance. Furthermore, the patient’s rapid decline precluded oral targeted therapy.
CONCLUSIONS
BRCA2 reversion mutations can arise early in the course of gBRCA-mutated breast cancer, even without PARPi or platinum exposure. Serial monitoring using liquid biopsies may help detect these events, guide treatment selection, and predict resistance. Further studies are needed to clarify the incidence, timing, and mechanisms of reversion mutations in breast cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Momozawa Y, Iwasaki Y, Parsons MT, et al. Germline pathogenic variants of 11 breast cancer genes in 7,051 Japanese patients and 11,241 controls. Nat Commun 2018; 9: 4083.30287823 10.1038/s 41467-018-06581-8PMC 6172276 · doi ↗ · pubmed ↗
- 2Robson M, Im SA, Senkus E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med 2017; 377: 523–33.28578601 10.1056/NEJ Moa 1706450 · doi ↗ · pubmed ↗
- 3Sakai W, Swisher EM, Karlan BY, et al. Secondary mutations as a mechanism of cisplatin resistance in BRCA 2-mutated cancers. Nature 2008; 451: 1116–20.18264087 10.1038/nature 06633 PMC 2577037 · doi ↗ · pubmed ↗
- 4Puhalla SL, Diéras V, Arun BK, et al. Relevance of platinum-free interval and BRCA reversion mutations for veliparib monotherapy after progression on carboplatin/paclitaxel for g BRCA advanced breast cancer (BROCADE 3 Crossover). Clin Cancer Res 2021; 27: 4983–93.34131001 10.1158/1078-0432.CCR-21-0748 PMC 9401555 · doi ↗ · pubmed ↗
- 5Tobalina L, Armenia J, Irving E, et al. A meta-analysis of reversion mutations in BRCA genes identifies signatures of DNA end-joining repair mechanisms driving therapy resistance. Ann Oncol 2021; 32: 103–12.33091561 10.1016/j.annonc.2020.10.470 · doi ↗ · pubmed ↗
- 6Ashworth A. Drug resistance caused by reversion mutation. Cancer Res 2008; 68: 10021–3.19074863 10.1158/0008-5472.CAN-08-2287 · doi ↗ · pubmed ↗
- 7Nakamura K, Hayashi H, Kawano R, et al. BRCA 1/2 reversion mutations in a pan-cancer cohort. Cancer Sci 2024; 115: 635–47.38041241 10.1111/cas.16033 PMC 10859608 · doi ↗ · pubmed ↗
- 8Afghahi A, Timms KM, Vinayak S, et al. Tumor BRCA 1 reversion mutation arising during neoadjuvant platinum-based chemotherapy in triple-negative breast cancer is associated with therapy resistance. Clin Cancer Res 2017; 23: 3365–70.28087643 10.1158/1078-0432.CCR-16-2174 PMC 5496787 · doi ↗ · pubmed ↗