Fluid responsiveness-guided individualized strategy for preventing hypotension after spinal anesthesia in cesarean delivery: a randomized trial of prehydration versus norepinephrine preinfusion
Chu-Chu Du, Wei Chen, Hao Wang, Ling Guo, Bin Wang, Yu-Long Wang, Yong-Quan Chen

TL;DR
This study shows that using a personalized approach based on fluid responsiveness can better prevent low blood pressure after spinal anesthesia during cesarean delivery.
Contribution
The study introduces a fluid responsiveness-guided strategy to individualize hypotension prevention in cesarean deliveries.
Findings
Fluid loading and norepinephrine infusion were equally effective in preventing hypotension in fluid-responsive parturients.
Norepinephrine infusion was more effective than fluid loading in preventing hypotension in non-fluid-responsive parturients.
Norepinephrine infusion was linked to higher neonatal lactate levels and slower postoperative recovery in fluid-responsive parturients.
Abstract
This study aimed to evaluate the efficacy of fluid responsiveness-guided strategies for preventing spinal anesthesia-induced hypotension (SAIH) in parturients undergoing cesarean delivery, comparing prophylactic fluid loading with norepinephrine infusion. In this fluid responsiveness-based stratified randomized controlled trial, eligible parturients were stratified into fluid responsive (FR(+)) and non-fluid responsive (FR(-)) cohorts according to carotid corrected flow time (FTc). Each stratum had a preset sample size of 236, and within each stratum, participants were randomly assigned to receive either prophylactic colloid infusion (Co) or norepinephrine infusion (NE), ultimately forming four subgroups: FR(+)/Co, FR(+)/NE, FR(-)/Co, and FR(-)/NE.Primary outcomes included the incidence of SAIH and maximum reduction in mean arterial pressure (MAP). Secondary outcomes encompassed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
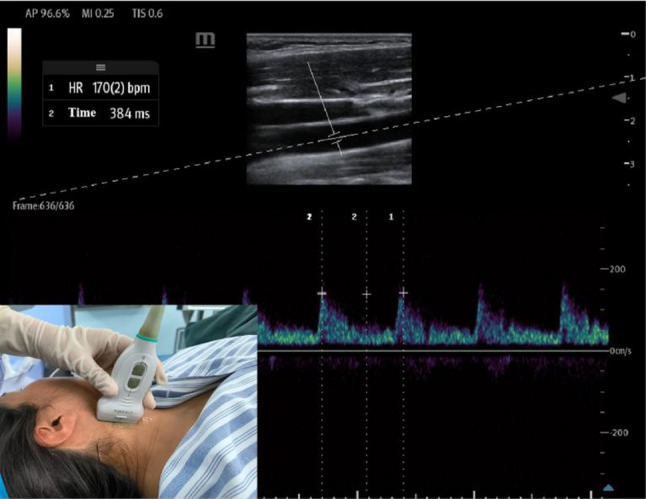 Figure 1
Figure 1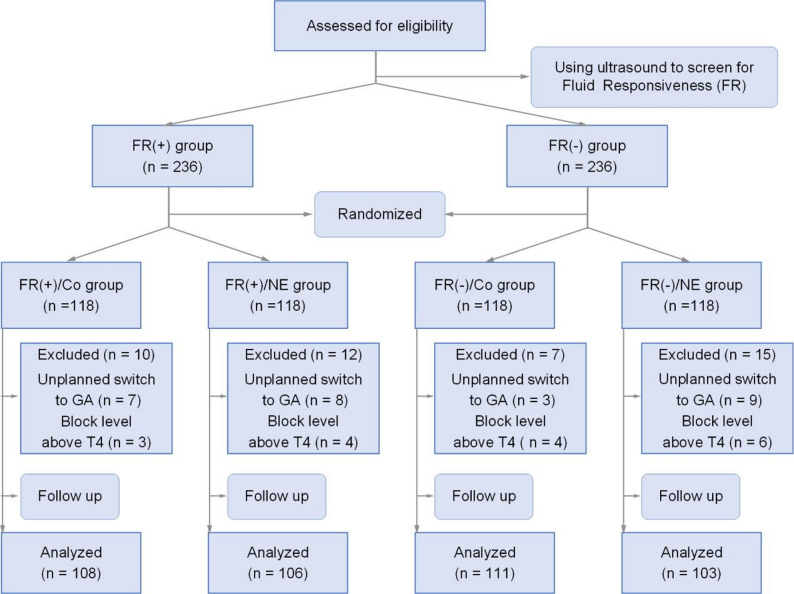 Figure 2
Figure 2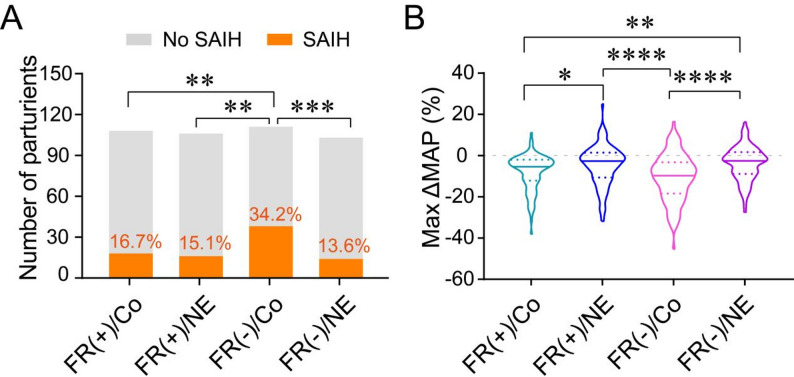 Figure 3
Figure 3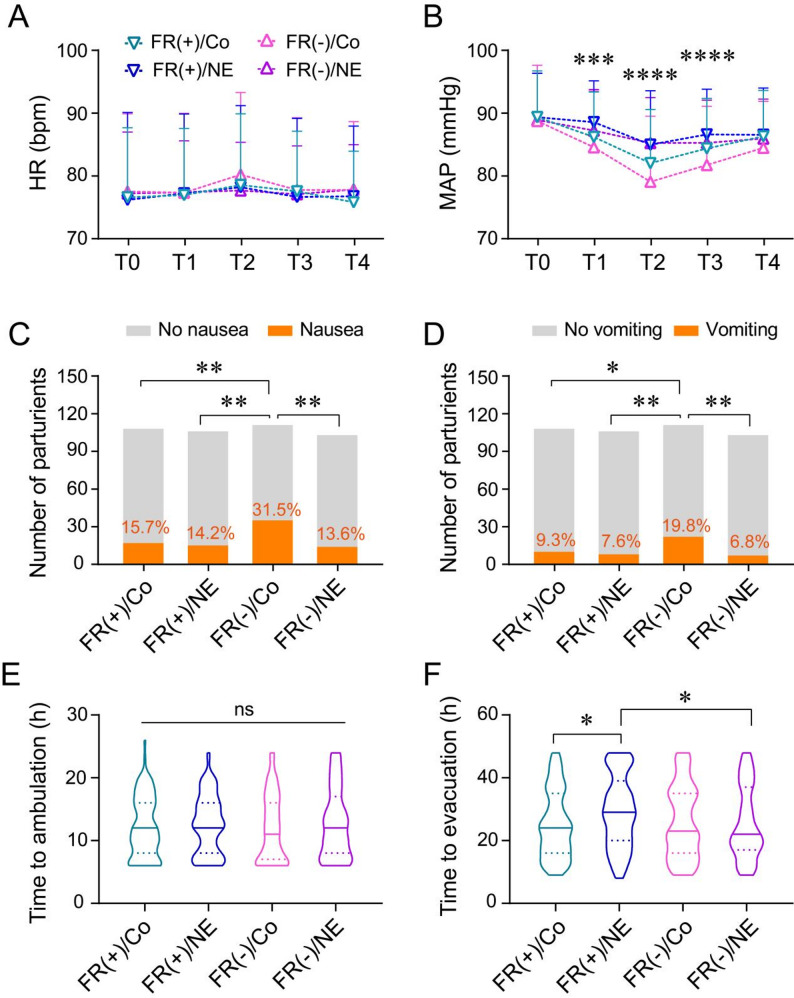 Figure 4
Figure 4- —Anhui University Research Project
- —Anhui Province Clinical Key Specialty Construction Project
- —Natural Science Foundation of Anhui Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemodynamic Monitoring and Therapy · Trauma, Hemostasis, Coagulopathy, Resuscitation · Thermal Regulation in Medicine
Introduction
Spinal anesthesia, favored for its rapid onset, reliable analgesia, and excellent muscle relaxation, has become the preferred anesthetic technique for cesarean sections. However, this method frequently leads to spinal anesthesia-induced hypotension (SAIH) in parturients, with an incidence ranging from 29% to 80% [1–4]. SAIH manifests clinically as nausea and vomiting, and carries serious implications for both mother and fetus. It can lead to maternal complications such as cerebral hypoperfusion, cardiovascular events, and renal impairment, as well as fetal risks including intrauterine hypoxia and acidosis, thereby jeopardizing maternal and neonatal safety [5–7].
Currently, prophylactic vasopressor administration and fluid loading are the primary clinical strategies for preventing SAIH [7–10]. Among vasopressors, α_1_-adrenergic receptor agonists such as phenylephrine and norepinephrine are recommended as first-line agents. However, their prophylactic use is limited in parturients with preeclampsia, hypertension, or cardiac comorbidities. Although some studies suggest that pre-anesthetic colloid infusion can reduce the incidence of SAIH [11], recent evidence indicates that fluid therapy alone is less effective than vasopressors and insufficient for SAIH prevention [7, 10, 12]. The underlying reasons for this discrepancy remain unclear, and we hypothesize that it may be related to individual variations in fluid responsiveness among parturients.
Fluid responsiveness refers to the capacity of the heart to increase its cardiac output in response to fluid administration, primarily reflecting cardiac preload. It is a well-established concept in the field of fluid resuscitation for critically ill patients [13, 14]. This concept is based on the Frank-Starling mechanism: when a patient operates on the ascending limb of the Frank-Starling curve, increasing preload significantly enhances cardiac output, indicating positive fluid responsiveness [15]. Building on this principle, we propose an innovative hypothesis: fluid loading is effective in preventing SAIH only in parturients with positive fluid responsiveness, and its efficacy is non-inferior to prophylactic norepinephrine administration. This hypothesis may provide a novel approach to individualized SAIH prevention. Corrected flow time (FTc) is a dynamic monitoring technique based on Doppler ultrasound that is non-invasive and can be performed at the bedside. It assesses a patient’s preload status and predicts fluid responsiveness by measuring and heart rate-correcting the carotid artery ejection time. Evidence confirms that changes in cardiac preload and output directly translate to carotid blood flow variations [16–18]. Consequently, carotid ultrasound parameters, particularly the FTc which reflects preload, serve as a reliable predictor of volume responsiveness in spontaneously breathing patients. And monitoring and managing fluid responsiveness can significantly reduce the incidence of hypotension following anesthesia [19].
In this study, we employ the emerging parameter of corrected flow time (FTc) measured by carotid ultrasound to assess fluid responsiveness. By comparing the clinical outcomes of parturients with positive and negative fluid responsiveness who receive either prophylactic fluid loading or norepinephrine administration, we systematically evaluate the incidence of SAIH, the maximum decrease in mean arterial pressure, intraoperative and postoperative complications, and postoperative recovery quality. Additionally, we focus on neonatal outcomes, including umbilical cord blood gas analysis and Apgar scores, to comprehensively assess the impact of different prophylactic strategies on maternal and neonatal outcomes.
Methods
Study design and participants
This prospective, randomized, controlled trial was approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College and registered at the Chinese Clinical Trial Registry (Registration No.: ChiCTR2400084392). Written informed consent was obtained from all participants or their legal guardians before the study.
The study enrolled parturients who were scheduled to undergo elective cesarean delivery under spinal anesthesia during the period from May 2024 to March 2025. Patients should refrain from eating solid foods 6–8 h before surgery and avoid drinking clear liquids 2 h before surgery. Inclusion criteria included: singleton pregnancy, age 18–48 years, body mass index (BMI) 20–40 kg/m², American Society of Anesthesiologists (ASA) physical status < III, and gestational age ≥ 37 weeks. Exclusion criteria comprised contraindications to the study drugs, comorbidities such as pregnancy-induced hypertension, diabetes, hyperthyroidism, or epilepsy, carotid artery stenosis > 50%, anatomical variations of the carotid artery, or refusal to participate. Additionally, cases were excluded if the surgical duration exceeded 3 h, the sensory block level was below T8 or above T4, or the anesthesia method was altered intraoperatively.
Carotid artery FTc measurement and fluid responsiveness criteria
Fluid responsiveness was assessed by a trained anesthesiologist using FTc (Fig. 1). Briefly, parturients were placed in the supine position with the head rotated approximately 30° to the right to expose the left common carotid artery. A linear array probe (L2-3) was used to perform transverse scanning at the level of the lower edge of the thyroid cartilage. The probe was then rotated 90° to obtain a longitudinal view, and Doppler ultrasound was used to measure the flow time (FT) and heart rate (HR) at the center of the artery, with an insonation angle ≤ 60°. FTc was calculated using the formula: FTc = FT + [1.29 × (HR − 60)]. Based on previous studies [18, 20], fluid responsiveness was defined as FTc < 326.9 ms (positive) or FTc ≥ 326.9 ms (negative).
Fig. 1. Ultrasound measurement of the blood flow time of the common carotid artery. HR: Heart rate*2; Time: Central blood flow time of the common carotid artery
Randomization and blinding
This study is a stratified randomized controlled trial based on fluid responsiveness. All enrolled subjects were first stratified according to baseline FTc measurements into fluid-responsive (FR(+)) and non-fluid-responsive (FR(-)) cohorts. The preset sample size for both strata was the same. Subsequently, within each cohort, 1:1 block randomization was performed using a computer-generated random number table: subjects in the FR(+) cohort were randomly assigned 1:1 to either the fluid-responsive colloid group (FR(+)/Co) or the fluid-responsive norepinephrine group (FR(+)/NE); subjects in the FR(-) cohort were similarly randomly assigned 1:1 to either the non-fluid-responsive colloid group (FR(-)/Co) or the non-fluid-responsive norepinephrine group (FR(-)/NE).
In this prospective study, except for the ultrasound measurers who were involved in subsequent statistical analysis and data processing, the pregnant women, nursing staff, and data collectors were all blinded to the group allocation. The randomization and recruitment process are summarized in the CONSORT flowchart (Fig. 2).
Interventions and anesthesia protocol
All parturients were transferred to the anesthesia preparation room at least 30 min before surgery, and none had received any sedative medications orally or by injection preoperatively. Standard monitoring was established using an anesthesia monitor, including electrocardiography, non-invasive blood pressure, and pulse oximetry. Baseline blood pressure (BP) and HR were recorded as the average of three consecutive measurements (T0).
Colloid group
Before spinal anesthesia, Hydroxyethyl starch 130/0.4 (15 mL/kg) was administered over 30 min [21, 22].
Norepinephrine group
Norepinephrine was diluted to 40 µg/mL (2 mg in 50 mL normal saline) and administered as a 0.1 µg/kg bolus followed by a continuous infusion at 0.05 µg/kg/min until delivery, after which the dose was gradually tapered [23].
Spinal anesthesia was performed in the left lateral position at the L3-L4 interspace under ultrasound localization, using 0.75% bupivacaine (7.5–11.25 mg, adjusted for height) combined with 2.5 µg sufentanil, with an injection speed of 1 mL/10 s [24]. After anesthesia, parturients were positioned with a 15° left tilt. Sensory block level was assessed using pinprick testing, and motor block depth was evaluated using the modified Bromage scale [25]. Surgery was initiated when the sensory block level reached T6 or above. The occurrence of hypotension was monitored, and BP and HR were recorded at the following time points: T1 (1 min post-spinal anesthesia), T2 (3 min post-spinal anesthesia), T3 (5 min post-spinal anesthesia), and T4 (at skin incision).
Outcome measures
Primary outcomes
Incidence of SAIH and maximum reduction in MAP. SAIH was defined as a decrease in systolic blood pressure (SBP) of more than 20% from baseline or the presence of hypotension-related symptoms such as nausea and vomiting (which were immediately treated with a 4 µg intravenous bolus of norepinephrine) [26].
Secondary outcomes
Neonatal umbilical artery blood gas analysis, 1-minute and 5-minute Apgar scores, intraoperative hemodynamic changes, incidence of intraoperative nausea and vomiting, time to postoperative flatus, and time to ambulation.
Safety outcomes
Incidence of intraoperative adverse events and postoperative dizziness or headache.
Sample size calculation
The sample size was calculated using PASS 15 (NCSS, LLC. Kaysville, Utah, USA) software. Based on previous studies [21, 22], the incidence of SAIH in the prophylactic colloid group was 36.6%. We hypothesized a reduction to 16.6% in the FR(+)/Co group. With a two-sided α = 0.05 and power (1-β) = 0.9, 98 participants per group were required, totaling 392 cases. Accounting for a 20% dropout rate, 472 parturients were enrolled.
Statistical analysis
Data were analyzed using SPSS 26 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism 9.0 (GraphPad Software, La Jolla, CA, USA) software. Normality was assessed using the Kolmogorov-Smirnov test. Normally distributed data were expressed as mean ± standard deviation (SD) and analyzed using Tukey’s multiple comparisons test; non-normally distributed data were expressed as median (interquartile range [IQR]) and analyzed using Dunn’s multiple comparisons test. These tests were two-tailed, and P < 0.05 was considered statistically significant. Categorical data were expressed as frequencies (percentages) and analyzed using chi-square or Fisher’s exact tests. the Bonferroni correction was applied for these multiple comparisons, with an adjusted significance level of P < 0.0083.
Results
Participant flow and baseline characteristics
A total of 472 parturients meeting the inclusion criteria were screened using carotid artery corrected flow time (FTc) and stratified into fluid-responsive (FR(+) group, n = 236) and non-fluid-responsive (FR(-) group, n = 236) cohorts. These groups were further randomized into four subgroups: FR(+)/Co group (n = 118), FR(+)/NE group (n = 118), FR(-)/Co group (n = 118), and FR(-)/NE group (n = 118). During the study, 27 parturients were excluded due to unplanned changes in anesthesia, and 17 were excluded because the sensory block level exceeded T4. Ultimately, 428 parturients (90.7%) completed the trial, and their data were included in the statistical analysis (Fig. 2).
Fig. 2CONSORT flow diagram of participant enrollment, allocation, and analysis. FR(+)/Co: Fluid preload in fluid-responsive parturients; FR(+)/NE: Norepinephrine infusion in fluid-responsive parturients; FR(-)/Co: Fluid preload in non-fluid-responsive parturients; FR(-)/NE: Norepinephrine infusion in non-fluid-responsive parturients
There were no significant differences among the four groups in baseline characteristics, including age, gravidity, parity, gestational age, BMI, uterine height, abdominal circumference, fetal biparietal diameter, femur length, preoperative fasting time, bupivacaine dosage, time from spinal anesthesia to skin incision, time from skin incision to fetal delivery, or sensory block level (P > 0.05, Table 1).
Table 1. Demographic and obstetric characteristicsFR(+)/CoFR(+)/NEFR(-)/CoFR(-)/NEP-value(n = 108)(n = 106)(n = 111)(n = 103)Age (y)33 ± 5.134 ± 4.932 ± 4.732 ± 4.90.158Gravidity2 (1, 2)2 (1.75, 2)2 (1, 2)2 (2, 2)0.612Parity1 (0, 1)1 (0, 1)1 (0, 1)1 (0, 1)0.643Gestational weeks38 (37, 39)38 (37, 39)38 (38, 39)38 (38, 39)0.065BMI (kg/m^2^)26.3 ± 3.5826.6 ± 3.6426.8 ± 2.9926.8 ± 3.110.619Fundal height (cm)34.8 ± 3.3334.2 ± 2.1635.0 ± 2.9434.4 ± 2.380.117Abdominal circumference (cm)102.0 ± 6.48102.1 ± 6.72102.1 ± 6.65101.1 ± 5.870.649BPD (mm)89.7 ± 4.7490.3 ± 4.4390.9 ± 4.1790.7 ± 5.290.227FL (mm)71.0 ± 4.8671.9 ± 5.8371.7 ± 4.9971.8 ± 6.130.553Time from spinal anesthesia to skin incision(min)13 (10,17)13 (10,19)15 (11,18)13.5 (10,18)0.739Time from skin incision to fetal delivery(min)12 (8,15)11 (7,14)11 (9,15)12 (9,15)0.143Fasting time (h)10.4 ± 2.6511.1 ± 2.6710.7 ± 2.7011.0 ± 2.490.227Data are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]), as appropriate. Abbreviations BMI Body Mass Index, BPD Biparietal Diameter, FL Fetal Femur Length
Primary outcomes
The incidence of SAIH in the FR(+)/Co, FR(+)/NE, FR(-)/Co, and FR(-)/NE groups was 16.7%, 15.1%, 34.2%, and 13.6%, respectively. The FR(-)/Co group had a significantly higher incidence of SAIH compared to the other three groups (P < 0.0083, Kruskal-Wallis test), while no significant differences were observed among the FR(+)/Co, FR(+)/NE, and FR(-)/NE groups (P > 0.05, Fig. 3A).
Fig. 3. Primary outcomes of the study. A Incidence of spinal anesthesia-induced hypotension (SAIH) in the FR(+)/Co, FR(+)/NE, FR(-)/Co, and FR(-)/NE groups. B Maximum reduction in mean arterial pressure (Max ΔMAP) expressed as percentage change from baseline: [(MAPatminimum-MAPatT0)/MAPatT0]×100. *P < 0.05, **P < 0.01. ***P < 0.001. ****P < 0.0001
The maximum reduction in MAP after spinal anesthesia was − 5.4% (-1.9%, -12.1%) in the FR(+)/Co group, -2.5% (1.5%, -10.1%) in the FR(+)/NE group, -9.7% (-3.2%, -18.4%) in the FR(-)/Co group, and − 2.6% (1.7%, -8.9%) in the FR(-)/NE group. The FR(-)/Co group exhibited a significantly greater reduction in MAP compared to the FR(+)/Co and FR(-)/NE groups (P < 0.001, Kruskal-Wallis test). Additionally, the FR(+)/Co group showed a greater reduction in MAP compared to the FR(+)/NE and FR(-)/NE groups (P < 0.05, Kruskal-Wallis test, Fig. 3B).
Secondary outcomes
The neonatal umbilical cord blood lactate (Lac) levels were 1.55 ± 0.28 mmol/L in the FR(+)/Co group, 1.66 ± 0.25 mmol/L in the FR(+)/NE group, 1.57 ± 0.30 mmol/L in the FR(-)/Co group, and 1.63 ± 0.31 mmol/L in the FR(-)/NE group. The Lac levels in the FR(+)/Co and FR(-)/Co groups were significantly lower than those in the FR(+)/NE group (P < 0.05). However, no significant differences were observed among the four groups in other umbilical cord blood gas parameters, including pH, base excess (BE), bicarbonate (HCO₃⁻), glucose (GLU), or 1-minute and 5-minute Apgar scores (P > 0.05, Table 2).
Table 2. Neonatal umbilical artery blood gas analysisFR(+)/CoFR(+)/NEFR(-)/CoFR(-)/NEP-value(n = 108)(n = 106)(n = 111)(n = 103)PH7.31 ± 0.047.32 ± 0.047.31 ± 0.037.32 ± 0.030.74Lac (mmol/L)1.55 ± 0.28^a^1.66 ± 0.251.57 ± 0.30^b^1.63 ± 0.310.019BE (mmol/L)-2.4 (-3.14, -1.85)-2.3 (-3.3, -1.41)-2.3 (-3, -1.49)-2.6 (-3.13, -1.78)0.321HCO_3_^−^ (mmol/L)23.54 ± 2.7823.04 ± 2.9323.14 ± 2.7522.837 ± 2.730.286Glu (mmol/L)3.98 ± 0.493.94 ± 0.514.10 ± 0.544.01 ± 0.520.124Apgar score 1 min9 (9, 9)9 (9, 9)9 (9, 9)9 (9, 9)0.257 5 min10 (10, 10)10 (10, 10)10 (10, 10)10 (10, 10)0.519Data are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]), as appropriate. ^a^P < 0.01, FR(+)/Co group vs. FR(+)/NE, ^b^P < 0.05, FR(-)/Co vs. FR(+)/NE
Although no significant differences were observed in heart rate (HR) at T0, T1, T2, T3, or T4 among the four groups (P > 0.05, Tukey’s multiple comparisons test, Fig. 4A), significant differences in MAP were noted at T1, T2, and T3 (P < 0.001, Tukey’s multiple comparisons test, Fig. 4B). The FR(-)/Co group had the lowest MAP, followed by the FR(+)/Co group.
Fig. 4. Secondary outcomes of the study. A & B Heart rate (HR) and mean arterial pressure (MAP) at different time points in the FR(+)/Co, FR(+)/NE, FR(-)/Co, and FR(-)/NE groups. Time points: T0, baseline; T1, 1 min post-spinal anesthesia; T2, 3 min post-spinal anesthesia; T3, 5 min post-spinal anesthesia; T4, skin incision. Data are presented as mean ± standard deviation (SD). ***P < 0.001, ****P < 0.0001 (ANOVA test). C & D Incidence of nausea (C) and vomiting (D) in the four groups. Data are presented as number of cases and percentage. *P < 0.05, **P < 0.01 (Chi-square test). Abbreviations: FR(+)/Co, fluid preload in fluid-responsive parturients; FR(+)/NE, norepinephrine infusion in fluid-responsive parturients; FR(-)/Co, fluid preload in non-fluid-responsive parturients; FR(-)/NE, norepinephrine infusion in non-fluid-responsive parturients. E & F Time to ambulation (E) and time to first postoperative evacuation (F) in the FR(+)/Co, FR(+)/NE, FR(-)/Co, and FR(-)/NE groups. Data are presented as median (interquartile range [IQR]). ns: P > 0.05 (ANOVA test); *P < 0.05 (Dunn’s multiple comparisons test)
The incidence of intraoperative nausea was 15.7% in the FR(+)/Co group, 14.2% in the FR(+)/NE group, 31.5% in the FR(-)/Co group, and 13.6% in the FR(-)/NE group. The incidence of vomiting was 9.3% in the FR(+)/Co group, 7.6% in the FR(+)/NE group, 19.8% in the FR(-)/Co group, and 6.8% in the FR(-)/NE group. The FR(-)/Co group had a significantly higher incidence of nausea and vomiting compared to the other three groups (P < 0.05, Chi-square test, Fig. 4C&D), while no significant differences were observed among the FR(+)/Co, FR(+)/NE, and FR(-)/NE groups (P > 0.05, Fig. 4C**&D**).
No significant differences were observed in the time to postoperative ambulation among the four groups (P > 0.05, Fig. 4E). However, the time to postoperative evacuation was significantly longer in the FR(+)/NE group compared to the FR(+)/Co group (29 [20, 39] h vs. 24 [16, 35] h, P < 0.05, Dunn’s multiple comparisons test, Fig. 4F) and the FR(-)/NE group (29 [20, 39] h vs. 22 [17, 37] h, P < 0.05, Dunn’s multiple comparisons test, Fig. 4F).
Safety outcomes
The incidence of intraoperative adverse events, including hypertension, bradycardia, tachycardia, chest tightness, as well as postoperative dizziness or headache, showed no statistically significant difference (P > 0.05, Table 3).
Table 3. Other secondary outcomesFR(+)/CoFR(+)/NEFR(-)/CoFR(-)/NEP-value(n = 108)(n = 106)(n = 111)(n = 103)Bupivacaine dose (mg)9 (8.25, 9.75)9 (8.25, 9.75)8.25 (8.25, 9)9 (8.25, 9)0.114Block level (T)6 (6, 7)6 (6, 7)6 (6, 6)6 (6, 7)0.184Intraoperative adverse events Hypertension1 (0.9)0 (0)0 (0)2 (1.9)> 0.05 Bradycardia6 (5.6)5 (4.7)3 (2.7)5 (4.9)> 0.05 Tachycardia6 (5.6)5 (4.7)9 (8.1)6 (5.8)> 0.05 Chest distress4 (3.7)3 (2.8)7 (6.3)2 (1.9)> 0.05Postoperative adverse events Dizziness6 (5.6)5 (4.7)7 (6.3)6 (5.8)> 0.05 Headache0 (0)0 (0)1 (0.9)0 (0)> 0.05Data are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]) / n (%), as appropriate
Discussion
The prevention of SAIH in parturients undergoing cesarean delivery is crucial for maternal and fetal safety. This study demonstrates that in fluid-responsive parturients, prophylactic fluid loading and norepinephrine infusion are equally effective in preventing SAIH. However, in non-fluid-responsive parturients, fluid loading is significantly less effective than prophylactic norepinephrine infusion and is associated with a higher incidence of intraoperative nausea and vomiting. Interestingly, our findings also suggest that prophylactic norepinephrine infusion in fluid-responsive parturients may lead to elevated umbilical Lac levels and prolonged postoperative gastrointestinal recovery time. These results highlight the critical role of fluid responsiveness in determining the efficacy of prophylactic fluid loading for SAIH prevention and its influence on the adverse effects of norepinephrine infusion. Our findings support the implementation of individualized SAIH prevention strategies based on parturients’ fluid responsiveness.
In this study, we utilized the novel ultrasound parameter, FTc. This non-invasive technique offers advantages in terms of simplicity, reproducibility, and clinical feasibility for assessing maternal fluid status. FTc primarily reflects cardiac preload, which is particularly relevant for parturients due to the significant impact of preload on hypotension. Our study confirms that a preoperative FTc < 326.9 ms predicts SAIH with high sensitivity and specificity (> 90%) [20]. Clinically, an FTc increase > 4% indicates positive fluid responsiveness, suggesting a favorable response to fluid therapy [17, 27]. Conversely, minimal changes in FTc suggest negative fluid responsiveness, warranting cautious fluid administration.
This study provides the first evidence of the pivotal role of fluid responsiveness in determining the efficacy of prophylactic fluid loading for SAIH prevention. We observed a significant difference in SAIH incidence between fluid-responsive and non-fluid-responsive parturients receiving prophylactic fluid loading (16.7% vs. 34.2%). The pathophysiology of SAIH involves sympathetic blockade-induced vasodilation, reduced venous return, and exacerbated hypotension due to uterine compression of the inferior vena cava and relative hypovolemia [28]. While vasopressors are commonly used, optimizing effective circulating volume is essential. However, not all parturients benefit from fluid loading [12], as adequate colloid volume is required to prevent hypotension, potentially mediated by fluid responsiveness. In fluid-responsive parturients, increased cardiac output following fluid loading helps maintain stable blood pressure, whereas non-fluid-responsive parturients cannot achieve this benefit, resulting in higher SAIH incidence. Notably, prophylactic fluid loading in fluid-responsive parturients achieved comparable efficacy to norepinephrine infusion. Interestingly, norepinephrine’s preventive effect on SAIH appears independent of fluid responsiveness, likely due to its primary mechanism of increasing peripheral vascular resistance [29, 30].
Consistent with previous studies [23, 26], norepinephrine infusion demonstrated superior SAIH prevention compared to fluid loading when fluid responsiveness was not considered (14.4% vs. 25.6%). Our study revealed higher umbilical cord blood Lac levels in the norepinephrine groups, suggesting potential fetal hypoxia. This effect was more pronounced in fluid-responsive parturients receiving norepinephrine, possibly due to vasoconstriction-induced alterations in fetal hemodynamics and reduced umbilical blood flow, particularly in volume-depleted parturients [31–33]. Nevertheless, the statistical significance of these findings must be interpreted with caution, as their clinical relevance may be limited. Despite these findings, there is insufficient evidence to contraindicate norepinephrine use in fluid-responsive parturients, as no differences were observed in pH, base excess, or Apgar scores. Further investigation is warranted in high-risk populations, such as those with pregnancy-induced hypertension.
Additionally, while no differences were observed in time to ambulation, the FR(+)/NE group exhibited significantly prolonged time to flatus, suggesting that norepinephrine infusion in fluid-responsive parturients may impair postoperative intestinal motility, potentially due to reduced intestinal perfusion in volume-depleted states [34].
It should be noted that the restrictions on the use of hydroxyethyl starch 130/0.4 by agencies such as the European Medicines Agency are mainly based on research evidence suggesting a potential increase in the risk of kidney injury and mortality in critically ill patients, particularly those with sepsis. The subjects of this study were all healthy postpartum women, whose risk-benefit context is significantly different from the aforementioned population. Therefore, the results of this study should be interpreted within this specific context. The findings are consistent with previous clinical studies on pregnant women [35, 36], and did not reveal any significant adverse effects on maternal or neonatal outcomes. Furthermore, a fundamental experiment conducted on rats [37], demonstrated that the drug exhibits a high level of safety at reasonable doses, with a relatively controllable metabolic process. The pharmacokinetic profile of the drug in rats shares similarities with that in humans, providing an important reference for the safety assessment of its clinical application.
This study has several limitations. First, the study did not include a combined prophylactic fluid loading and norepinephrine infusion group. Future studies should explore optimal dosing regimens for combination therapy. Second, we did not assess post-intervention fluid responsiveness, which warrants investigation in subsequent research. Finally, the strict inclusion criteria for elective cesarean delivery may limit the generalizability of our findings to emergency cesarean sections or parturients with pathological conditions such as pregnancy-induced hypertension.
Conclusions
In conclusion, our study demonstrates that FTc-guided assessment of fluid responsiveness is valuable for optimizing the choice between prophylactic fluid loading and norepinephrine infusion to prevent SAIH, reduce neonatal hypoxia, and promote postoperative recovery. For fluid-responsive parturients, prophylactic fluid loading may be preferable to norepinephrine infusion, while norepinephrine should be prioritized for non-fluid-responsive parturients. These findings provide insights into the variable efficacy of fluid loading in SAIH prevention and contribute to precise perioperative blood pressure management and enhanced recovery after cesarean delivery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baytaş V, Karadağ Erkoç S, Özçelik M, Gökmen D, Bermede AO, Selvi Can Ö, Uysalel A. A Randomized, Double-Blind, graded Dose-Response study of norepinephrine administration for prevention of Post-Spinal hypotension during elective Cesarean delivery. J Clin Med 2023, 12(20).10.3390/jcm 12206437 PMC 1060754737892573 · doi ↗ · pubmed ↗
- 2Messina A, Romano SM, Bonicolini E, Colombo D, Cammarota G, Chiostri M, Della Corte F, Navalesi P, Payen D, Romagnoli S. Cardiac cycle efficiency and dicrotic pressure variations: new parameters for fluid therapy: an observational study. Eur J Anaesthesiol 2017, 34(11):755–63.10.1097/EJA.000000000000066128722695 · doi ↗ · pubmed ↗