Vulnerability and non-adherence to treatment in cisgender women living with HIV/AIDS: a scoping review (2000–2024)
Denise Eliziana de Souza, Cleber Nascimento do Carmo, Simone Monteiro

TL;DR
This review explores how gender inequalities and social factors affect HIV treatment adherence in cisgender women and highlights the need for integrated solutions.
Contribution
A conceptual model is proposed to explain how vulnerability contexts impact treatment adherence in cisgender women with HIV/AIDS.
Findings
Stigma affects all levels of vulnerability and contributes to treatment non-adherence.
Barriers include mental health, gender-based violence, and structural health system issues.
A socio-ecological model is introduced to guide interventions addressing these challenges.
Abstract
Cisgender women are disproportionately affected by HIV/AIDS due to structural gender inequalities and intersecting social determinants, which generate vulnerability contexts that act as barriers to treatment adherence. A scoping review to map studies examining vulnerability contexts influencing antiretroviral treatment non-adherence and discontinuation among cisgender women living with HIV/AIDS. Searches were performed in PubMed, SciELO, Scopus, Web of Science, and gray literature. A total of 78 studies published between 2000 and 2024 were included. Findings were organized across three vulnerability dimensions individual, social, and programmatic. Stigma emerged as a transversal element permeating all levels. Barriers included mental health conditions, substance use, pregnancy and postpartum dynamics, socioeconomic inequalities, gender-based violence, and structural barriers in health…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
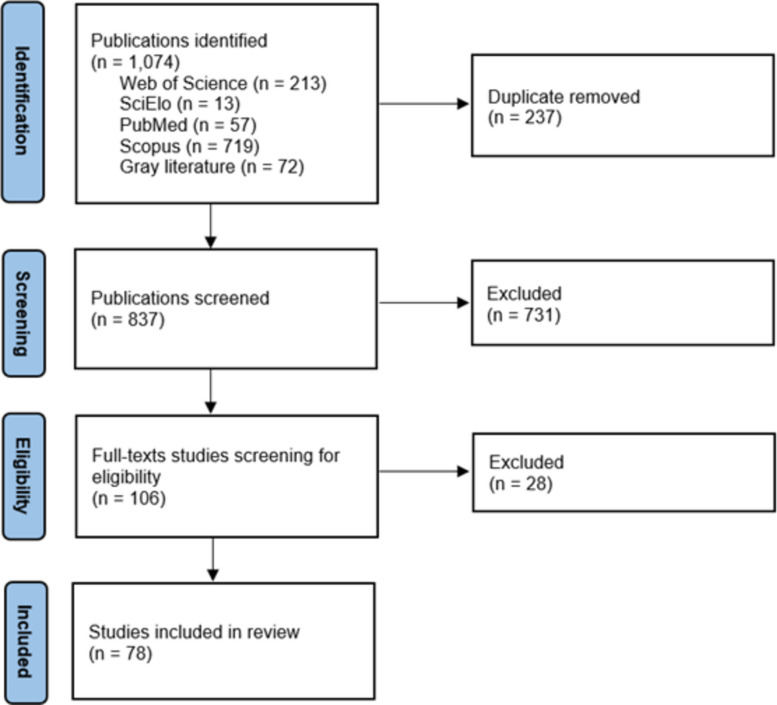 Figure 1
Figure 1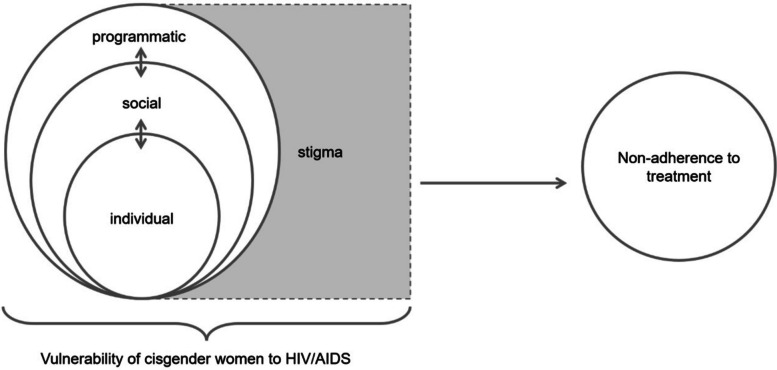 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Adolescent Sexual and Reproductive Health · HIV-related health complications and treatments
Text box 1. Contributions to the literature- Maps evidence (2000–2024) on vulnerability contexts associated with antiretroviral treatment non-adherence and discontinuation among cisgender women living with HIV/AIDS.- Shows that stigma intersects mental health symptoms, violence, and socioeconomic deprivation across individual, social, and health-system levels to undermine adherence.- Highlights pregnancy and the postpartum period as a high-risk window for disengagement due to service transitions, caregiving demands, and disclosure-related pressures.- Identifies policy and practice entry points for gender-responsive care, including stigma and violence-informed services, strengthened continuity across maternal and HIV/AIDS services, and social protection to reduce structural barriers.
Introduction
Human Immunodeficiency Virus and Acquired Immunodeficiency Syndrome (HIV/AIDS) affects population groups in unequal ways. In 2024, an estimated 40.8 million people were living with HIV/AIDS worldwide. In the same year, approximately 1.3 million new infections were reported, and around 630,000 deaths occurred due to AIDS-related causes. Women and girls accounted for nearly 45% of all new infections globally, highlighting persistent gender-based inequalities in HIV vulnerability. In sub-Saharan Africa—a region marked by pronounced structural and social vulnerabilities—cisgender women and girls represented approximately 63% of new HIV infections, with a substantial concentration among women of reproductive age [1]. As an illustrative national context, data from Brazil indicate that 81.4% of reported HIV cases in 2024 occurred among individuals aged 15 to 49 years, alongside a growing proportion of diagnoses among women aged 50 years or older, increasing from 10.9% in 2014 to 17.0% in 2024 [2]. These trends underscore the need to consider age, gender, and context-specific vulnerability dynamics when examining antiretroviral treatment engagement among women living with HIV.
Gender inequalities intersect with social, racial-ethnic, generational, and regional disparities, heightening women’s vulnerability to HIV infection and creating barriers to sustained treatment adherence. These vulnerabilities are not restricted to individual behavior, but are shaped by structural and relational dynamics, such as unequal power relations, stigma, and limited access to resources. At the same time, women demonstrate autonomy in negotiating health care, disclosing their diagnosis, and mobilizing support networks, which highlights the complexity of adherence behaviors [3].
The concept of social determinants of health (SDH) provides a useful starting point for understanding these inequalities, encompassing individual, social, and structural conditions that affect health outcomes [4, 5]. Dahlgren and Whitehead [6] proposed that these determinants be arranged in layers, from individual characteristics to macro-structural conditions. Complementing this perspective, the socio-ecological model emphasizes the interactions between levels of influence—individual, relational, community, and institutional—highlighting their interdependence [7].
Applied to the HIV/AIDS context, theoretical approaches aim to identify how inequalities affect infection risks, access to care, as well as health services [8]. The concept of vulnerability in the health area emphasizes the interaction among these factors, taking into consideration the cultural, institutional, geographical, as well as informational components [9].
Building on these perspectives, the concept of vulnerability has been widely applied in the field of HIV/AIDS. Mann, Tarantola and colleagues [10, 11] advanced the notion that vulnerability goes beyond individual risk, incorporating social, economic, cultural, and institutional factors that shape exposure, prevention, and care. Later, Ayres and collaborators [12, 13] proposed a three-dimensional framework—individual, social, and programmatic vulnerabilities—to analyze how these dimensions interact and condition health outcomes. This perspective emphasizes that health care outcomes are not merely the consequence of individual choices but rather emerge from a complex web of interactions among individuals, societal structures, and institutional frameworks. Such an approach offers a conceptual basis for comprehending the multifactorial realities that shape the lived experiences of people living with HIV/AIDS (PLWHA). This framework is particularly useful for examining adherence to antiretroviral therapy (ART), as it situates women’s experiences within broader social and programmatic contexts.
In this review, we operationalize the vulnerability framework by charting and synthesizing evidence into three interrelated dimensions: individual vulnerability (e.g., mental health symptoms, substance use, treatment beliefs, caregiving burden), social vulnerability (e.g., stigma, violence, poverty, gender norms, partner dynamics, social support), and programmatic vulnerability (e.g., service accessibility, continuity of care, communication with providers, health system fragmentation) [12, 13]. This structure supports a socio-ecological interpretation of adherence, emphasizing that treatment engagement is shaped by interactions between personal circumstances, social relations, and health system arrangements rather than individual choices alone [7].
Aligned with this theoretical basis, the present review investigates how vulnerability contexts affect antiretroviral treatment adherence among women living with HIV/AIDS (WLWHA). In order to deepen the understanding of factors associated with non-adherence, this article sought to map the existing academic literature on the subject, identifying determinants of non-adherence; here understood as the failure or inconsistency in following prescribed therapeutic regimens, which may compromise the effectiveness of continuous antiretroviral therapy and related clinical monitoring indicators [14].
Methods
This study consists of a scoping review of the academic literature addressing vulnerability contexts that hinder HIV/AIDS treatment adherence among cisgender women. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses—Extension for Scoping Reviews (PRISMA-ScR) guidelines [15] and was guided by the methodological framework proposed by the Joanna Briggs Institute (JBI) [16]. The process involved six main key steps: (1) identification of the research question; (2) identification of relevant studies aligned with the objectives of the review; (3) selection of studies based on predefined inclusion and exclusion criteria; (4) data charting; (5) synthesis of findings through thematic analysis; and (6) presentation of results, highlighting implications for policy, clinical practice, and future research. The review protocol was registered on the Open Science Framework platform (OSF) [17].
Searches
The research question, constructed using the population-concept-context (PCC) strategy, is: How do various vulnerability contexts impact the failure to adhere to and abandonment of antiretroviral treatment by cisgender women living with HIV/AIDS? The review focused on three analytical dimensions of vulnerability—individual, social, and programmatic—based on the framework proposed by Ayres and collaborators [12, 13]. Accordingly, studies addressing factors related to non-adherence among WLWHA were included, encompassing conference abstracts, guidelines, books, editorials, primary studies employing qualitative, quantitative, or mixed methods, reviews, theses, and dissertations. No restrictions were imposed regarding language, publication dates, or locations.
The search was conducted between October and December 2024 across health-related databases, including the National Library of Medicine (PubMed), Scientific Electronic Library Online (SciELO), Scopus, and Web of Science. To include gray literature, searches were performed in the Digital Library of Theses and Dissertations (DLTD). Descriptors, including Medical Subject Headings (MeSH) terms, were: "cisgender women," "women," "female," "non-adherence," "treatment failure," "abandonment," "HIV," "Acquired Immunodeficiency Syndrome," "antiretroviral therapy," "ART," "antiretroviral treatment," and their Portuguese equivalents, combined using Boolean operators "OR" and "AND." Gray literature was searched in the DLTD using the same PCC logic and translated keywords aligned with the database strategy. Records retrieved from DLTD were exported and imported into Rayyan alongside bibliographic database results for deduplication and screening. Titles/abstracts were screened independently by two reviewers, followed by full-text screening using the same eligibility criteria applied to peer-reviewed studies. When necessary, additional document information (e.g., thesis institutional repository page) was consulted to confirm eligibility.
Study inclusion and exclusion criteria
The study included peer-reviewed articles and gray literature that addressed WLWHA; reported on treatment adherence, discontinuation, or interruption; analyzed factors associated with individual, social, or programmatic vulnerabilities. Exclusion criteria were studies focusing exclusively on male or transgender populations; articles not addressing adherence or treatment interruption.
Potential effect modifiers and reasons for heterogeneity
Not applicable to this scoping review, which aimed to map evidence rather than assess comparative effects or sources of statistical heterogeneity.
Study quality assessment
Not performed, as this is a scoping review conducted in accordance with PRISMA-ScR guidance.
Data extraction strategy
Studies were managed using the Rayyan Qatar Computing Research Institute platform [18] for duplicate removal and screening processes. Two reviewers independently screened titles and abstracts, followed by full-text reading of potentially eligible studies. Disagreements were resolved by consulting a third reviewer. The review team had full-text proficiency in Portuguese, English, and Spanish. For studies in other languages (e.g., French, Italian, Romanian), titles/abstracts were screened using available translations, and full texts were assessed with translation support when required, with key excerpts cross-checked by the reviewers to minimize misinterpretation. Subsequently, full-text readings were conducted for analysis and content summarization using a data extraction spreadsheet containing information on title, author, publication year, journal, country of study, objectives, population, methodology, main results, and final considerations.
Data synthesis and presentation
Extracted data were analyzed using qualitative content analysis. Studies were organized according to the vulnerability framework proposed by Ayres and collaborators [12, 13]. Recurring themes were identified, and findings were synthesized narratively. Theoretical concepts of vulnerability and the socio-ecological perspective guide the interpretation of results. Finally, results were compiled through thematic construction based on elements influencing the research question's response.
Results
Review statistics
From 1,074 initial studies, 213 were identified in Web of Science, 13 in SciELO, 57 in PubMed, 719 in Scopus, and 72 in gray literature. After removing 237 duplicates, 837 studies remained. Of these, 731 were excluded after title and abstract screening for not meeting the review's objectives, leaving 106 studies for full-text reading and analysis, and 78 were included in this study (Fig. 1).Fig. 1PRISMA-ScR flowchart results for a scoping review on vulnerability and non-adherence to treatment in cisgender women living with HIV/AIDS (2000–2024). Source: elaboration constructed by the authors. Note: Searches conducted October-December 2024 using Rayyan. PRISMA-ScR: Preferred Reporting Items for Systematic Reviews and Meta-Analyses – Scoping Review Extension
Among the 106 full-text reports assessed, 28 were excluded for reasons including: lack of women-specific results (e.g., mixed-gender samples without stratified analyses), absence of ART adherence/non-adherence outcomes, focus on prevention rather than treatment engagement, ineligible population (not cisgender women living with HIV), or insufficient information to determine adherence-related findings.
Study quality assessment
Not applicable. No formal quality appraisal was conducted, consistent with the objectives of this scoping review.
Quantitative synthesis/meta-analysis
Not applicable. No quantitative synthesis or meta-analysis was planned or conducted.
Evidence of effectiveness
Not assessed, as this review aimed to map vulnerability contexts rather than evaluate intervention effectiveness.
Study characteristics
The selected studies were published between 2000 and 2024 in Portuguese, English, Spanish, French, Italian, and Romanian. Included materials comprised peer-reviewed journal articles (85.9%), gray literature such as theses and dissertations (12.8%), and conference presentations (1.3%). The majority originated from the Americas (53.8%), followed by Africa (37.2%), Europe (7.7%), Asia (2.5%), and one multi-country study (1.3%) involving Argentina, Botswana, Brazil, China, the United States, Haiti, Peru, and Thailand. Quantitative studies predominated (64.0%), with qualitative approaches (18.0%), reviews and evidence syntheses (11.5%), and mixed-methods studies (6.4%).
Table 1 presents general characteristics of the studies, including author, year, population scope, and country coverage.Table 1. Study characteristics (author, year, population, and country) extracted for a scoping review on vulnerability and non-adherence to treatment in cisgender women living with HIV/AIDS (2000–2024)AuthorsYearPopulationCountryJohnston et al2000WLWHAUnited StatesSankar et al2002WLWHAUnited StatesMellins et al2002WLWHA—mothers from ethnic minoritiesUnited StatesMurphy et al2002WLWHA—symptomatic or AIDS-diagnosedUnited StatesWood et al2004WLWHA—mothersUnited StatesSchiopescu et al2005PLWHAUnited StatesLocher et al2007WLWHA—black womenUnited StatesMellins et al2008WLWHA—pregnant and postpartumUnited StatesUbbiali et al2008PLWHAItalyCosta et al2009WLWHABrazilPlankey et al2009WLWHAUnited StatesPsaros et al2009WLWHA—with depressionUnited StatesApplebaum et al2009PLWHAUnited StatesPuskas et al2011PLWHAUnited StatesFelix et al2012WLWHABrazilChristie et al2012WLWHA—pregnant women, exposed children, adolescentsJamaicaBonolo et al2013PLWHABrazilVitalis2013WLWHAEnglandPhillips et al2014WLWHA—pregnant womenSouth AfricaRemien et al2014PLWHAUnited StatesNjuki et al2014WLWHAKenyaPadoin et al2015WLWHABrazilFagbami et al2015WLWHAUnited StatesWillie et al2016WLWHA—history of childhood sexual abuseUnited StatesGameiro2016WLWHA—pregnant womenBrazilSanta Helena2016WLWHABrazilPhillips et al2016WLWHA—pregnant womenSouth AfricaHatcher et al2016WLWHA—pregnant and postpartumSouth AfricaCurrier et al2017WLWHA—postpartumArgentina, Botswana, Brazil, China, Haiti, Peru, Thailand, United StatesLi et al2017PLWHAUnited StatesLobato2017WLWHA—pregnant womenBrazilAcheampong et al2017WLWHA—breastfeeding mothersGhanaAdeniyi et al2018WLWHA—postpartumSouth AfricaLangwenya et al2018WLWHASouth AfricaSikkema et al2018WLWHASouth AfricaKadima et al2018WLWHA—pregnant womenLesothoWilliams et al2018WLWHA—pregnant womenUnited StatesMusoke et al2018Male partners of pregnant HIV-positive and negative womenKenyaOmonaiye et al2018WLWHA—pregnant womenSub-Saharan AfricaRamlagan et al2019WLWHASouth AfricaGeter et al2019WLWHAUnited StatesDlamini et al2019WLWHA—postpartumEswatiniNamale et al2019WLWHAUgandaBraga2019PLWHAMozambiqueCoan2019WLWHA—pregnant womenBrazilConroy et al2019Serodiscordant and seroconcordant couplesMalawiTebeu et al2019WLWHA—pregnant womenCameroonKisigo et al2020WLWHA—postpartumTanzaniaGouvea2020WLWHABrazilAllam et al2020WLWHA—sex workersIndiaCutimanco-Pacheco et al2020WLWHA—pregnant womenPeruAduloju et al2020WLWHA—pregnant womenNigeriaMarcu et al2020WLWHA—pregnant womenRomaniaGarriga et al2020PLWHASpainMedeiros et al2021WLWHA—pregnant and postpartumBrazilCandido et al2021WLWHABrazilPeña et al2021WLWHASpainMukose et al2021WLWHA—pregnant womenUgandaCabral et al2021WLWHABrazilLorenzetti et al2021WLWHA—pregnant and postpartumMalawiDada et al2021WLWHA—pregnant and postpartumNigeriaSão Pedro2022WLWHA—pregnant womenBrazilMyer et al2022WLWHA—postpartumSouth AfricaHatcher et al2022WLWHASouth AfricaMarinaro et al2022WLWHAItalyArgolo Júnior2022WLWHA—elderly womenBrazilMinja et al2022WLWHA—pregnant women with depressionTanzaniaBarros2023WLWHABrazilPellowski et al2023WLWHA—pregnant and postpartumSouth AfricaPalar et al2023WLWHAUnited StatesWang et al2023WLWHA—sex workersDominican RepublicMartins et al2023PLWHABrazilBatitucci2023WLWHA—pregnant womenBrazilStedile2024WLWHA—pregnant womenBrazilTusabe et al2024WLWHA—refugee pregnant womenUgandaTizianel et al2024PLWHABrazilHeydari et al2024WLWHAIranZeleke et al2024WLWHAEthiopiaData sources: Scopus, PubMed, SciELO, Web of Science, and Digital Library of Theses and DissertationsWLWHA Women living with HIV/AIDS, PLWHA People living with HIV/AIDS
A significant proportion focused exclusively on WLWHA (84.6%); among these, 48.5% centered on pregnancy and/or postpartum contexts. Additionally, studies analyzing PLWHA by gender highlighted differences associated with increased vulnerability among women to HIV/AIDS.
Vulnerability contexts of cisgender Women to HIV/AIDS
Analyzing factors related to non-adherence among WLWHA through vulnerability dimensions reveals interconnections among factors, emphasizing the importance of this analytical perspective in understanding and promoting treatment adherence.
Based on the vulnerability framework proposed by Ayres and collaborators [12, 13], Table 2 organizes the identified factors into individual, social, and programmatic dimensions.Table 2. Thematic synthesis of individual, social, and programmatic vulnerabilities associated with non-adherence, extracted for a scoping review on vulnerability and non-adherence to treatment in cisgender women living with HIV/AIDS (2000–2024)DimensionAspectsIndividualAge [28; 35; 42–62]; education level[47–48; 57–60]; pregnancy/postpartum [19; 42; 57; 58; 61; 63–69]; mental health [19–27]; alcohol and drug use [28–34]; attitudes and beliefs [26; 35–46]; time since diagnosis [28; 35; 42]; race/skin color [44; 56; 68; 78]; mode of transmission [70; 71]; body image perception [39; 59]; clinical status [63; 72; 76]SocialSocioeconomic status [43; 79; 82]; food insecurity [46; 81]; stigma perception [47; 79–81]; social and family support [79; 80]; marital/relationship status [21; 54]; migrant/refugee status [83]; sex work [44; 73]; incarceration [83]; partner involvement [73; 80]; disclosure of HIV status [28; 66]; context of violence [21; 22; 35; 84]ProgrammaticDistance to healthcare services [24; 40; 85]; availability of ART [69; 78]; availability of healthcare staff [41; 50]; therapeutic regimen [79; 86; 87]; vertical transmission prevention protocol [55; 75]; provider-patient relationship [24; 80]; timing of ART initiation [72; 88]; institutional/governmental policies [32; 58; 66]Data sources: Scopus, PubMed, SciELO, Web of Science, and Digital Library of Theses and DissertationsART Antiretroviral
Individual vulnerability
Individual vulnerability encompasses a complex interplay of psychosocial, behavioral, and clinical determinants that significantly affect adherence to therapeutic regimens. Mental health disorders—particularly anxiety, depression, bipolar affective disorder (BAD), and post-traumatic stress disorder (PTSD) [19–27], constitute critical barriers to consistent treatment engagement. These conditions often impair cognitive functioning, emotional regulation and motivation, thereby undermining the patient’s ability to comply with prescribed interventions. Additionally, the consumption of both legal and illicit psychoactive substances has been consistently identified as a major impediment to adherence, further exacerbating treatment discontinuity and compromising health outcomes [28–34].
Negative or unfavorable attitudes and beliefs regarding antiretroviral therapy have also been identified as vulnerability factors [26, 35–42]. These factors influence behaviors that increase exposure to risks, such as non-adherence to preventive and self-care practices [43–46].
Younger women and those with a shorter time since diagnosis appear more prone to non-adherent behaviors [28, 35, 42–60]. Among older women, adherence behavior was generally satisfactory, although ignorance and fear were reported as dominant initial reactions to the diagnosis [61]. Another relevant aspect involves the experience of menopause; women experiencing symptoms are more likely to exhibit non-adherence compared to asymptomatic women [62].
Initiation of ART during later stages of pregnancy—possibly reflecting a late diagnosis—was associated with poorer adherence indicators [19, 61, 63–68]. The postpartum period is also significant: the literature indicates that better adherence during pregnancy is often driven by fear of vertical transmission of HIV to the baby. However, adherence behaviors typically decline after delivery [42, 57, 58]. These dynamics reflect social and structural expectations placed on women as caregivers, often prioritizing the well-being of others, particularly children, over their own health, especially in the context of motherhood [69].
Women infected through vertical transmission tend to demonstrate greater adherence compared to those infected via sexual transmission, possibly due to greater risk awareness and the lifelong internalization of self-care practices [70]. Furthermore, women diagnosed for longer periods are generally more adapted to their treatment routines, which facilitates adherence [65, 71]. Nevertheless, one study found that women diagnosed before 2005 were at higher risk of treatment interruption, possibly due to challenges related to the longitudinal nature of care [72].
Perceptions of antiretroviral therapy side effects can hinder treatment continuity and increase the risk of discontinuation [32, 53–55, 58, 59, 73–77]. Additional clinical factors, such as low CD4 + lymphocyte counts, late ART initiation, drug interactions from concurrent treatments, and the presence of comorbidities, complicate adherence due to the increased complexity of the therapeutic regimen and uncertainty about its effectiveness [63, 72, 76]. Body image concerns, particularly regarding fat redistribution or accumulation, also serve as predictors of non-adherence, adversely affecting women's attitudes toward their treatment [39, 59].
Lower educational attainment is associated with a reduced capacity to comprehend the importance of continuous treatment and the consequences of HIV infection, which may hinder adherence [47–49, 52, 53]. Women with lower education levels consistently demonstrate lower adherence rates than men, indicating greater vulnerability [54, 60].
Skin color and race also play a critical role: black women (including those identified as black or brown) and other ethnic minorities frequently experience worse adherence outcomes due to structural racism, discrimination, and barriers in accessing healthcare [44, 56, 68, 78]. Findings on race/ethnicity and adherence were reported predominantly in studies from the United States, where race/ethnicity variables were more consistently collected and analyzed; evidence from other regions was more limited and less comparable, which constrains cross-context generalizability.
Fear, related both to disease progression and to potential rejection, negatively affects adherence by creating psychological and social barriers [26, 35, 79, 80]. In this context, stigma is a particularly significant obstacle to treatment adherence. It is commonly linked to fears of discrimination and social exclusion, especially in communities where HIV is still surrounded by taboos [64, 66, 68].
These factors are often interwoven with other aspects of vulnerability, particularly those that fall within the social and programmatic dimensions, discussed in the following sections.
Social vulnerability
Social vulnerability refers to economic and social factors that hinder adherence to treatment. Within this context, stigma is prominently cited in literature as a critical factor, significantly affecting the emotional well-being of WLWHA, with direct consequences for their treatment adherence. Experiences of stigmatization often lead to feelings of shame, social isolation, and lack of support, all of which jeopardize treatment continuity and intensify emotional and social vulnerability [47, 81].
Women who face stigma, whether in family settings, social environments, or within healthcare systems, tend to experience greater difficulty maintaining therapeutic adherence due to fear of judgment or rejection [79, 80]. As a result, many choose to conceal their HIV status, which limits social support and engagement with treatment networks [28, 66]. Marital or relational status also plays a significant role: women who maintain relationships with partners to whom they have not disclosed their HIV status or who do not participate in their treatment process are more likely to encounter difficulties with adherence [21, 54]. These factors together may influence women’s perceptions of the illness as well as the treatment, modulating adherence behaviors [44, 72].
Partner involvement may indeed offer both emotional and practical support, constituting a protective factor. Socio-familial support networks can help women cope with the challenges of living with HIV and undergoing antiretroviral therapy [73, 80].
Studies have also identified that socioeconomic aspects are decisive in shaping adherence behaviors and other health outcomes among WLWHA. Women with low income and educational levels often face significant access barriers to treatment [43, 79, 82]. In this regard, unemployment and food insecurity are particularly detrimental, contributing to worsened physical and mental health conditions and posing substantial obstacles to adherence [46, 81].
Contextual factors such as migrant or refugee status can further complicate access to treatment due to lack of healthcare access, language barriers, and uncertainties related to relocation [83]. Similarly, WLWHA who engage in sex work face multiple layers of vulnerability—including stigma, discrimination, and limited healthcare access—which negatively affect adherence [44, 73]. Notably, women in conflict with the law or experiencing incarceration exhibit the poorest levels of adherence [83], highlighting the impact of structural barriers on healthcare access.
Furthermore, the context of violence must be underscored as a compounding factor of vulnerability, intrinsically tied to gender-based inequality. According to the literature, women who experience violence may lack the resources, both emotional and practical, to seek and maintain treatment, particularly due to trauma [22]. Research on intimate partner violence (IPV) and studies involving WLWHA who experienced childhood abuse reveal that such contexts of violence significantly compromise adherence, including among pregnant women. These situations are often linked to poor clinical outcomes and mental health issues [21, 22, 35, 84, 85].
As demonstrated, individual and social factors, when interrelated with programmatic factors described in the next section, highlight the complex challenges that women living with HIV must navigate to maintain consistent treatment adherence.
Programmatic vulnerability
Programmatic vulnerability refers to issues related to public policies and access to healthcare services. Public policies are expected to promote equity between individuals and health services, ensuring democratic access to healthcare resources. Programmatic factors include barriers to treatment access such as the complexity of therapeutic regimens, as well as unfavorable institutional attitudes and protocols that may discourage treatment continuity.
Structural barriers represent a fundamental challenge to HIV treatment adherence, especially within contexts of social and economic inequality. WLWHA in situations of vulnerability frequently encounter difficulties in initiating and maintaining adequate treatment due to distance from healthcare services or transportation challenges [24, 40, 41, 50, 69, 78, 86]. Moreover, the stigma associated with HIV may in fact discourage women from seeking medical services for fear of discrimination [43, 63].
Beyond concerns about side effects, the complexity of antiretroviral regimens may pose adherence barriers for WLWHA who struggle with comprehension, organization, and lack of psychological or social support [79, 87, 88]. In this regard, in addition to social support, a strong bond between the patient and healthcare providers may foster treatment engagement. Trust in healthcare professionals facilitates adherence, especially when women feel welcomed and understood. Studies highlight that positive interpersonal relationships with healthcare providers are among the most decisive factors for treatment success, whereas lack of rapport may lead to treatment abandonment [24, 80].
The HIV vertical transmission prevention protocol may also act as a barrier to adherence. Beyond subjective aspects, the demands and routines required by this protocol may complicate adherence. While pregnancy is often associated with improved adherence among WLWHA, the complexity and rigor of the protocol, along with the availability and workflow of healthcare services, may become obstacles. Structural barriers hinder both access and follow-up for pregnant women, compounding vulnerabilities related to pregnancy and the postpartum period [72, 85].
The timing of ART initiation is also a critical factor from a programmatic perspective. Starting treatment as soon as possible after diagnosis is essential to reduce viral load, prevent disease progression, and reduce transmission. Several studies indicate that delayed ART initiation, especially among young or pregnant women, increases the risk of complications and vertical transmission [58, 75]. Delays may stem from fear of diagnosis, late awareness, or difficulties accessing and connecting with healthcare services. Moreover, such delays are linked to institutional shortcomings, limited availability of reference services, and pervasive stigma.
The lack of effective public policies and inconsistent implementation of prevention and treatment programs also obstruct access to medication and care for many women [32]. Policies such as free medication distribution, accessible healthcare facilities, and awareness campaigns are essential to ensure that all women have equal opportunities for treatment. Furthermore, effective policies may help reduce access barriers and ensure that treatment is initiated and maintained appropriately [58, 66].
Pregnancy and postpartum-specific vulnerabilities
Nearly half of the included studies focused on pregnancy and/or postpartum contexts. In this subset, programmatic vulnerabilities were often centered on transitions across services (e.g., antenatal care, delivery, postpartum follow-up) and disruptions in continuity of ART and monitoring. Social vulnerabilities were frequently mediated by disclosure concerns, partner dynamics, and stigma related to motherhood and vertical transmission. Individual-level factors included emotional distress, treatment fatigue, and competing caregiving demands. These patterns suggest that pregnancy/postpartum periods may concentrate intersecting vulnerabilities and represent a critical window for differentiated support to sustain ART engagement.
Vulnerability and non-adherence in cisgender women
Based on the reviewed studies, a hypothetico-deductive model [89] is proposed to represent the relationships between individual, social, and programmatic dimensions of vulnerability among cisgender women living with HIV/AIDS. These dimensions are conceived as existing across proximal, intermediate, and distal levels, in accordance with the Social Determinants of Health framework [6] and the socio-ecological model [7]. This model maps the components of each vulnerability dimension as outlined in Table 2. Non-adherence is defined here as the failure or inconsistency in following prescribed treatment guidelines, negatively impacting adherence indicators [14].
Figure 2 illustrates the proposed model, highlighting how individual, social, and programmatic vulnerabilities interact and reinforce each other, ultimately affecting adherence. Stigma, although classified under the social dimension, is represented as a transversal element permeating all levels of vulnerability.Fig. 2. Conceptual model of vulnerability and non-adherence to treatment derived from a scoping review on vulnerability and non-adherence to treatment in cisgender women living with HIV/AIDS (2000–2024). Source: elaboration constructed by the authors
The model illustrates how individual (e.g., depression/anxiety, substance use, side effects, caregiving burden), social (e.g., anticipated/enacted stigma, gender-based violence, poverty/food insecurity, disclosure dynamics, social support), and programmatic vulnerabilities (e.g., clinic accessibility/transport, waiting times, continuity of care, postpartum follow-up, patient–provider communication) interact across proximal, intermediate, and distal levels to influence adherence and discontinuation. Stigma is represented as a transversal mechanism permeating all dimensions.
The intertwining of these dimensions reveals that many factors are common to two or more categories, adding layers of complexity to their interactions. The combined effects of these vulnerabilities may negatively impact both adherence behaviors and monitoring indicators. Not only do these barriers differ from those faced by men, as it also varies among women, considering their individual and collective diversities. The proposed model thus suggests that analyses of barriers to treatment adherence among WLWHA must account for the distinct dimensions of vulnerability, their interactions, and their effects on treatment outcomes and monitoring.
Discussion
The findings of this review indicate that adherence to antiretroviral therapy among WLWHA is shaped by a complex interplay of vulnerabilities extending beyond individual behavior. Although numerous studies examined adherence-related factors, many did not explicitly employ the term “vulnerability.” We interpret this as primarily a terminological and theoretical framing gap, rather than absence of vulnerability-related mechanisms: the reported barriers and facilitators map conceptually onto individual, social, and programmatic dimensions.
A systematic review analyzing gender-based differences in adherence identified female sex as a predictor of non-adherence, referencing vulnerability primarily in terms of gender-related factors affecting treatment [90]. Other studies aligned conceptually with vulnerability frameworks but did not explicitly adopt the terminology.
Similarly, a prior scoping review in Brazil emphasized the interplay of individual, social, economic, and structural conditions influencing adherence, noting that the term “vulnerability” has been inconsistently applied despite its conceptual relevance early in the HIV epidemic [91]. Over time, literature focus has shifted toward risk-oriented and epidemiological interpretations, moving away from broader vulnerability perspectives.
The literature’s emphasis on pregnancy and the postpartum period reflects a predominantly clinical and biomedical focus, particularly regarding vertical transmission and antenatal care. This prioritization often marginalizes broader social and structural factors affecting WLWHA’s lives and treatment adherence [44–80]. Consequently, treatment technologies and biomedical outcomes may overshadow women’s lived experiences, neglecting the influence of power structures and social determinants. In the perspective, Foucault’s theory of biopower provides a lens to understand how medicalized governance reinforces control over women’s bodies, particularly concerning sexuality and reproductive roles [92]. The focus on preventing vertical transmission links women’s health responsibilities to reproductive control. Coitinho Filho and Rinaldi [93] highlight how the moralized discourse of undetectability in pregnant women reinforces medicalized oversight of female bodies.
The present review reinforces the interconnection between individual, social, and programmatic dimensions of vulnerability, illustrating how these dimensions compound one another. Individual vulnerabilities are shaped by social inequalities, which are, in turn, structured through institutional and policy frameworks [94–100].
Among all factors, stigma consistently emerged as the most pervasive determinant, operating at multiple levels—internalized fear (individual), discrimination and violence (social), and barriers to healthcare services (programmatic). It exacerbates the vulnerability of WLWHA by undermining both social and institutional relationships. Though typically classified as part of the social dimension [12], it is evident that stigma transcends all levels, making it one of the most powerful forces disrupting adherence. Addressing stigma, alongside gender-based inequalities and structural barriers, is thus central to improving adherence. Overall, the interrelation of vulnerabilities underscores the need for comprehensive approaches that integrate biomedical, social, and structural perspectives, supporting evidence from other HIV-affected populations [101].
While vulnerability provides the primary analytic framework of this review, syndemic theory offers complementary insight into the synergistic nature of co-occurring challenges, helping to interpret how mental health conditions, violence, substance use, and socioeconomic deprivation interact to intensify barriers to sustained antiretroviral treatment adherence [102].
Strengthening adherence requires moving beyond purely biomedical paradigms toward strategies that prioritize social justice, human rights, and structural change. Addressing stigma, along with broader gender-based inequalities and structural barriers, is therefore central to improving adherence. Despite decades of HIV programs focused on women, persistent disparities underscore the need for more integrated responses that value women’s autonomy, recognize their autonomy, and promote equitable access to care. Strengthening adherence in this population requires moving beyond biomedical paradigms toward comprehensive strategies that incorporate social justice, human rights, and structural change.
Limitations
This scoping review has limitations. First, definitions and measurements of ART adherence/non-adherence varied substantially across studies (e.g., self-report, pharmacy refill, clinical indicators), limiting direct comparability across contexts. Second, consistent with scoping review guidance, we did not conduct critical appraisal of individual sources; therefore, the mapped evidence reflects the breadth of available literature rather than strength of causal inference. Third, despite efforts to include gray literature, our approach may not have captured all non-indexed sources and may be influenced by publication bias. Fourth, language capacity and translation support may have introduced residual language bias, particularly for full texts beyond the team’s primary languages. Finally, the relatively high proportion of pregnancy/postpartum-focused studies may shape the prominence of these contexts in the synthesis, and findings may not fully represent vulnerabilities outside reproductive care pathways.
Conclusions
This scoping review demonstrates that barriers to adherence to antiretroviral therapy among cisgender WLWHA is shaped by interconnected vulnerability contexts spanning individual, social, and programmatic dimensions. Adherence challenges are not limited to personal responsibility but emerge from the intersection of mental health conditions, socioeconomic inequalities, gender-based violence, stigma, and structural barriers within health systems.
Recognizing these overlapping vulnerabilities highlights the need for comprehensive strategies that integrate biomedical, social, and structural perspectives. Interventions must address clinical factors while simultaneously confronting gender inequalities, racial and socioeconomic disparities, and institutional practices that reinforce exclusion.
Importantly, women’s autonomy must be acknowledged many navigate treatment while managing family responsibilities, negotiating disclosure, and mobilizing social support. Policies and programs should build on this autonomy while actively reducing systemic inequities. Effectively addressing HIV among women requires moving beyond risk-focused and biomedical approaches toward rights-based, equity-driven responses. Reducing stigma, ensuring equitable access to care, and promoting social justice are essential to enhance adherence and ultimately improve the health and well-being of WLWHA. While several recommendations—such as strengthening continuity of care, reducing structural barriers to access, and implementing stigma and violence-informed services—emerged across multiple regions, some policy levers are context-dependent and should be adapted to local health system organization, resource availability, and sociocultural conditions.
Supplementary Information
Supplementary Material 1. Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joint United Nations Programme on HIV/AIDS (UNAIDS). Global report: UNAIDS report on the global AIDS epidemic 2025. Geneva: UNAIDS; 2025. Available from: https://unaids.org.br/. Cited 2025 Dec 31.
- 2Brasil. Ministério da Saúde. Boletim Epidemiológico HIV/Aids 2025. Brasília: Ministério da Saúde; 2025. Available from: https://www.gov.br/aids/pt-br/central-de-conteudo/boletins-epidemiologicos/2025/boletim_hiv_aids_2025.pdf/view. Cited 2025 Dec 31.
- 3Dahlgren G, Whitehead M. Policies and strategies to promote social equity in health. Stockholm: Institutet för Framtidsstudier; 2007. Available from: https://core.ac.uk/download/pdf/6472456.pdf. Cited 2024 Oct 20.
- 4Pires RP. Modelo teórico de análise sociológica. Sociol Probl Prat. 2014;74:9-37. Available from: http://journals.openedition.org/spp/1426. Cited 2024 Nov 20.
- 5Joanna Briggs Institute. Joanna Briggs Institute reviewers’ manual: 2014 edition. Adelaide: Joanna Briggs Institute; 2014. Available from: https://jbi.global/scoping-review-network/. Cited 2024 Sep 6.
- 6Barros SF. Ser mulher com HIV: preditores da adesão ao tratamento antirretroviral em relação ao distress, estigma e percepção de doença [dissertação]. Brasília: Universidade de Brasília; 2023. Available from: http://repositorio 2.unb.br/jspui/handle/10482/49433. Cited 2024 Oct 20.
- 7Gouvea PB. Fatores relacionados à adesão a terapia antirretroviral entre mulheres com HIV atendidas na Rede de Atenção à Saúde de um município prioritário do Sul do Brasil [tese]. Florianópolis: Universidade Federal de Santa Catarina; 2020. Available from: https://repositorio.ufsc.br/handle/123456789/216297. Cited 2024 Dec 2.
- 8Batitucci CP. Maternidade de mulheres vivendo com HIV e sua relação com o tratamento antirretroviral: estudo de revisão sistemática [dissertação]. São Paulo: Universidade de São Paulo; 2023. Available from: https://www.teses.usp.br/teses/disponiveis/5/5137/tde-03052023-155100/. Cited 2024 Dec 20.