Case report: a two-step approach in the management of angle-closure glaucoma associated with Plateau iris configuration
Tiago Santos Prata, Isabella Cristina Tristão Pinto Resende, Daniela Mauricio Ribeiro, Fábio Nishimura Kanadani, Izabela Negrão Frota de Almeida

TL;DR
A two-step treatment approach for a patient with advanced angle-closure glaucoma and Plateau iris improved vision and pressure control with fewer complications.
Contribution
A two-step treatment using cyclophotocoagulation followed by phacoemulsification is proposed as a simpler alternative for managing Plateau iris.
Findings
Both eyes achieved improved visual acuity and intraocular pressure control.
The two-step approach resulted in fewer medications and no significant complications.
The method offers more predictable outcomes compared to combined surgeries.
Abstract
Angle-closure glaucoma is a major cause of visual impairment worldwide, with Plateau iris syndrome presenting management challenges. We present a case report of a 58-year-old woman with advanced, uncontrolled angle--closure glaucoma and Plateau iris. Her history included laser peripheral iridotomy and three glaucoma medications in both eyes. Different treatments were implemented. For the eye with lower intraocular pressure, fewer peripheral anterior synechiae, and milder disease: phacoemulsification with intraocular lens implantation. For the eye with more advanced disease, a two-step approach was used: slow-coagulation transscleral cyclophotocoagulation using the double-arc protocol, followed by phacoemulsification with intraocular lens implantation 2 months later. Both eyes achieved improved visual acuity and intraocular pressure control with fewer medications, without significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
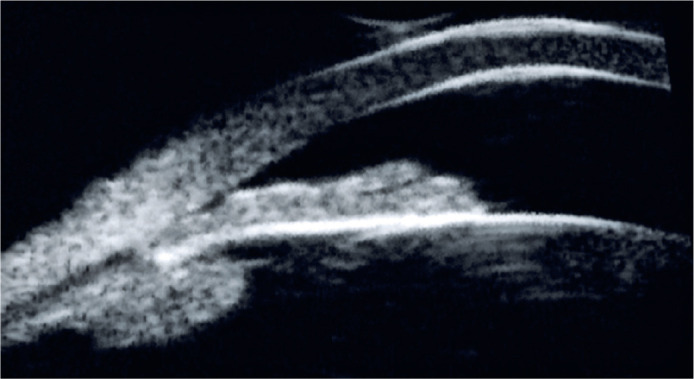 Figure 1
Figure 1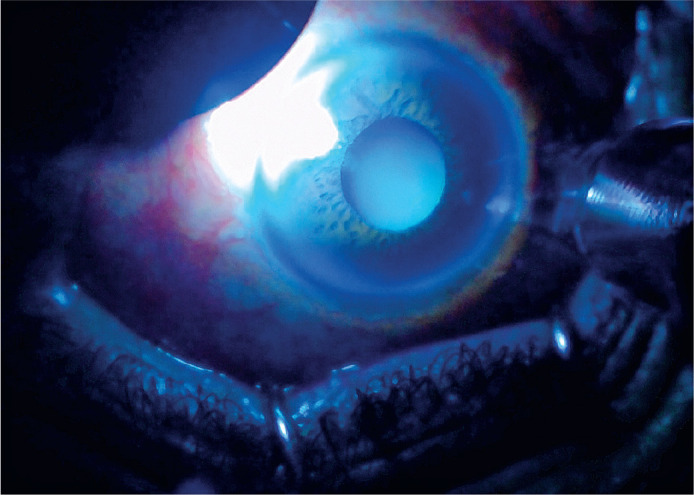 Figure 2
Figure 2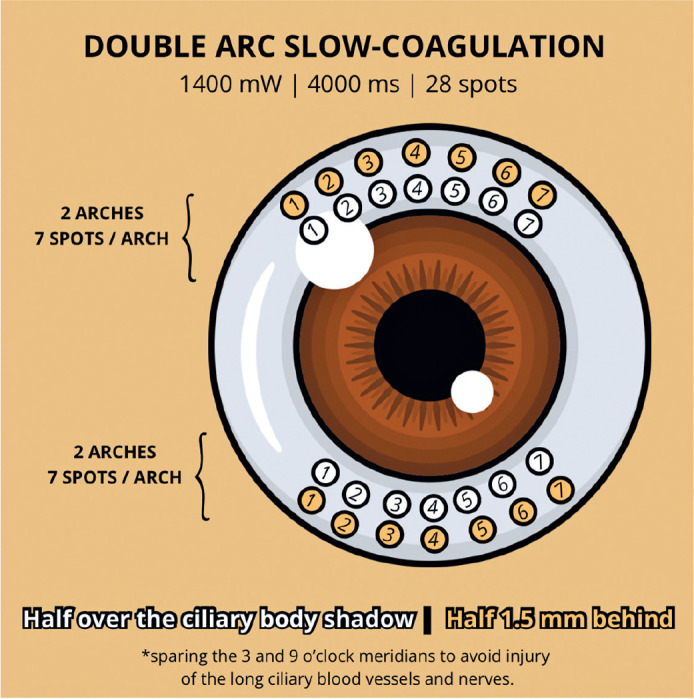 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Intraocular Surgery and Lenses · Retinal and Macular Surgery
INTRODUCTION
Angle-closure glaucoma (ACG) is a major cause of visual impairment worldwide. It is characterized by elevated intraocular pressure (IOP) due to impaired drainage of aqueous humor, often resulting from anatomic abnormalities that block the trabecular meshwork. Plateau iris syndrome presents unique management challenges among the forms of ACG due to its distinct anatomical configuration^(1)^.
Regarding treatment, laser peripheral iridotomy (LPI), the first-line therapy, is insufficient if there is persistent IOP elevation or extensive peripheral anterior synechiae (PAS)^(1)^. Phacoemulsification also deepens the anterior chamber (AC) and widens the angle, relieving IOP^(2)^. However, in more advanced disease or anatomical challenges, it may not adequately control IOP, requiring combined or sequential interventions^(3)^.
Traditionally, combined phacoemulsification and trabeculectomy are used in advanced cases but carry a higher risk of complications, particularly in eyes with Plateau iris^(3)^. An alternative is a two-step strategy using transscleral cyclophotocoagulation (TSCPC) with the double-arc slow-coagulation TSCPC protocol (DA-TSCPC), followed by phacoemulsification. This approach may be safe and effective for complex cases^(4)^.
A PubMed literature review on September 16, 2024, using the keywords “Transscleral Cyclophotocoagulation” and “Plateau iris”, identified one successful case of ACG and Plateau iris treated with combined phacoe-mulsification, goniotomy, and TSCPC^(5)^. No reports of DA-TSCPC followed by phacoemulsification were found. This case presents a strategy for managing uncontrolled ACG and Plateau iris configuration, offering insights into the benefits and considerations of a staged surgical approach.
CASE REPORT
A healthy 58-year-old White female was referred due to uncontrolled ACG, on three glaucoma medications (brinzolamide plus timolol maleate, and latanoprost in both eyes - OU), treated for 9 years. Her ocular history included only laser peripheral iridotomy (LPI) in OU.
Best-corrected visual acuity (BCVA) was 20/25 in OU, with mild hyperopia (+1.50 -0.75 × 135 in the right eye - OD; +1.25 -0.50 × 160 in the left eye - OS). IOP was 25 mmHg in OD and 17 mmHg in OS. Biomicroscopy revealed mild cataracts, a shallow peripheral anterior chamber (AC), and a relatively deep central AC in OU. Gonioscopy showed occludable angles with the double hump sign during indentation, extensive peripheral anterior synechiae (PAS) in OD, and appositional angle closure with localized PAS in OS. Fundus examination showed enlarged disc cupping, more pronounced in OD (cup-to-disc ratio of 0.85 OD and 0.7 OS), with neuroretinal rim thinning confirmed by structural and functional tests (Mean Deviation: -11.82 and -4.11, OD and OS, respectively). Ultrasound biomicroscopy revealed a Plateau iris configuration in OU (Figure 1).
Figure 1. Ultrasound biomicroscopy (UBM) shows anteriorly positioned ciliary processes, a narrow or absent ciliary sulcus, and a flat central iris with steep peripheral angulation, consistent with a Plateau iris configuration.
Given the findings, different approaches were used for each eye. For OS, which had lower IOP and fewer PAS, phacoemulsification with intraocular lens (IOL) implantation was performed. For OD, which had higher IOP, extensive PAS, and more advanced disease, a two--step approach was used: DA-TSCPC^(4)^ followed by phacoemulsification with IOL implantation 2 months later.
DA-TSCPC was performed under peribulbar anesthesia using a transillumination microscope (Figure 2) and a conventional 810 nm diode laser with a laser probe (Lightmed Corporation, San Clemente, CA, USA). The settings were 1400 mW and 4000 ms. A total of 28 applications were applied in four rows: upper and lower arcs (Figure 3). For each arc, 7 spots were placed over the ciliary body shadow (perilimbal dark band) and 7 spots 1.5 mm behind, sparing the 3 and 9 o’clock meridians. No “POP sound” indicative of ciliary body explosion was heard. The patient was prescribed 0.1% nepafenac 4 times/day for 15 days and 1% prednisolone acetate 4 times/day, tapered by removing one dose each week.
Figure 2. The ciliary body position was determined by transillumination.
Figure 3. The double-arc slow-coagulation transscleral cyclophotocoagulation technique has 28 applications divided into four rows: two superior and two inferior (upper and lower arcs).
Six weeks after surgery in OS, IOP was 14 mmHg with two topical medications. Six weeks after DA-TSCPC in OD, IOP was 13 mmHg with three topical medications. Following phacoemulsification in OD, one medication was discontinued. After six months, BCVA was 20/20 in OU (refraction: +0.50 -0.50 × 145 and +0.25 -0.50 × 150, OD and OS, respectively), and medications remained unchanged (brinzolamide plus timolol maleate in OU), with IOP at 14 and 12 mmHg. No significant postoperative pupillary diameter changes were observed in OU.
DISCUSSION
This case highlights the complexity of managing ACG, particularly in eyes with Plateau iris. Although many cases can be managed with phacoemulsification^(2)^, eyes with uncontrolled IOP and advanced damage often require a combined procedure, such as phacoemulsification and trabeculectomy^(3)^.
However, combined procedures can be challenging, especially in the presence of Plateau iris, a risk factor for postoperative malignant glaucoma^(6)^. This underscores the need to explore surgical techniques that improve patient safety in such cases.
In this case, a two-step approach was used for OD instead of the conventional combined procedure. We believe this strategy offers advantages, particularly in eyes with good visual potential^(4)^. Dividing the treatment simplifies each step, reduces aggressiveness, improves postoperative inflammation control, and potentially lowers the risk of complications associated with combined phacoemulsification and cyclophotocoagulation (CPC). It also allows for more straightforward postoperative management^(7)^.
Additionally, performing CPC before cataract surgery enhances predictability in pressure control, which enables more precise surgical planning^(4)^. It also offers flexibility to repeat CPC or adjust the technique if the initial outcome is suboptimal^(8)^. However, this approach requires two visits to the surgical center under anesthesia.
Diode laser TSCPC has been successfully used to treat chronic ACG, with a one-year success rate over 80%^(9)^. In this case, it eliminated the need for a filtering procedure and reduced the risk of ocular decompression in OD. Evidence also suggests that laser application to the ciliary body may deepen the AC, potentially making phacoemulsification easier and refractive outcomes more predictable^(10)^.
While potential complications of TSCPC include prolonged inflammation and hypotony, our one-year safety profile of DA-TSCPC showed that complications were infrequent and transient, especially in eyes with better visual prognosis^(4)^.
In summary, this case demonstrates the potential of TSCPC as a preparatory step before phacoemulsification in eyes with uncontrolled ACG and Plateau iris. This approach may provide a safer and more effective alternative to traditional combined procedures. The case is part of an ongoing prospective study, with one-year results pending publication. However, studies with larger sample sizes and longer follow-up are needed to confirm the safety and efficacy of this two-step approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Junqueira DL Prado VG Lopes FS Biteli LG Dorairaj S Prata TS. Non-pupillary block angle-closure mechanisms: a comprehensive analysis of their prevalence and treatment outcomes Arq Bras Oftalmol 20147763603632562718110.5935/0004-2749.20140090 · doi ↗ · pubmed ↗
- 2Azuara-Blanco A Burr J Ramsay C Cooper D Foster PJ Friedman DS EAGLE study group Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial Lancet 20163881005213891397 Comment in: Arch Soc Esp Oftalmol. 2017;92(8):401-2; Natl Med J India. 2017;30(2):78-9. Comment on: Lancet. 2016;388(10052):1349; Lancet. 2016;388(10052):1352-4.2770749710.1016/S 0140-6736(16)30956-4 · doi ↗ · pubmed ↗
- 3Tham CC Kwong YY Leung DY Lam SW Li FC Chiu TY Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts Ophthalmology 20091164725731 Comment in: Ophthalmology. 2009;116(12):2478;author reply 2478-9. Ophthalmology. 2009; 116(12):2479; author reply 2479-80.1924383110.1016/j.ophtha.2008.12.054 · doi ↗ · pubmed ↗
- 4Almeida IN Resende IC Magalhães LM Oliveira HK Kanadani FN Prata TS. Double-Arc slow-coagulation transscleral cyclophotocoagulation laser protocol: one-year effectiveness and safety outcomes Ophthalmol Glaucoma 2024765805863897152310.1016/j.ogla.2024.06.008 · doi ↗ · pubmed ↗
- 5Laroche D Rickford K Sakkari S. Case report: cataract extraction/lensectomy, excisional goniotomy, and transscleral cyclophotocoa-gulation: affordable combination MIGS for plateau iris glaucoma J Natl Med Assoc 2022114138413499857210.1016/j.jnma.2021.12.005 · doi ↗ · pubmed ↗
- 6Prata TS Dorairaj S De Moraes CG Mehta S Sbeity Z Tello C Is preoperative ciliary body and iris anatomical configuration a predictor of malignant glaucoma development?Clin Exp Ophthalmol 20134165415452327957610.1111/ceo.12057 · doi ↗ · pubmed ↗
- 7Nirappel A Klug E Neeson C Chachanidze M El Helwe H Hall N Transscleral vs endoscopic cyclophotocoagulation: safety and efficacy when combined with phacoemulsification BMC Ophthalmol 20232311293699787910.1186/s 12886-023-02877-6PMC 10061713 · doi ↗ · pubmed ↗
- 8Khodeiry MM Sheheitli H Sayed MS Persad PJ Feuer WJ Lee RK. Treatment outcomes of slow coagulation transscleral cyclophotocoagulation in pseudophakic patients with medically uncontrolled glaucoma Am J Ophthalmol 202122990993385290610.1016/j.ajo.2021.04.003 · doi ↗ · pubmed ↗