Interobserver Reproducibility of the Visual Echocardiographic Scoring System for Left Ventricular Filling Pressure
Yuka Uruma, Michito Murayama, Wahei Uemura, Namiko Sakai, Midori Shimomura, Kaori Nozaki, Yasuyuki Kunieda

TL;DR
This study shows that a simple echocardiographic method for assessing heart pressure is highly reliable across different users and devices.
Contribution
Demonstrates excellent interobserver agreement for a handheld echocardiographic scoring system across varying expertise and equipment.
Findings
11 out of 27 patients had VMT scores ≥2, indicating elevated left ventricular filling pressure.
Interobserver agreement for VMT scoring had a weighted kappa of 0.97, indicating almost-perfect concordance.
Agreement was consistent regardless of operator experience or device type (handheld vs. stationary).
Abstract
Background The visually assessed time difference between mitral and tricuspid valve opening (VMT) scoring is a simple B-mode echocardiographic method for estimating left ventricular filling pressure (LVFP). This study aimed to evaluate the interobserver reproducibility of VMT scoring between a resident doctor using a handheld ultrasound device and experienced sonographers using a stationary system. Methodology In this prospective observational study, 27 inpatients underwent two echocardiographic examinations on the same day: a handheld ultrasound performed by a resident doctor and standard echocardiography performed by cardiac sonographers. Both observers independently assessed VMT scores (0-3) based on the time sequence of atrioventricular valve opening and inferior vena cava findings. Interobserver agreement was evaluated using weighted kappa statistics. Results Among the 27…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
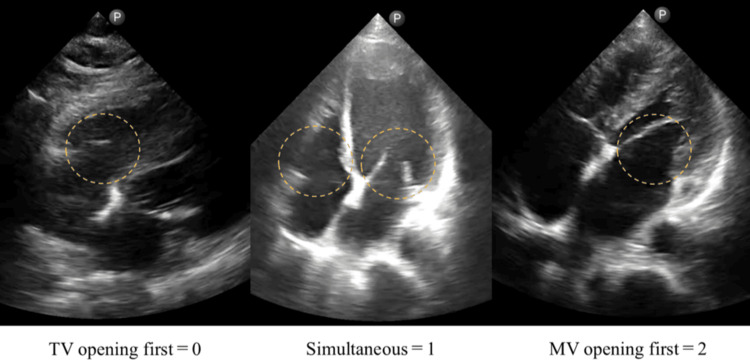 Figure 1
Figure 1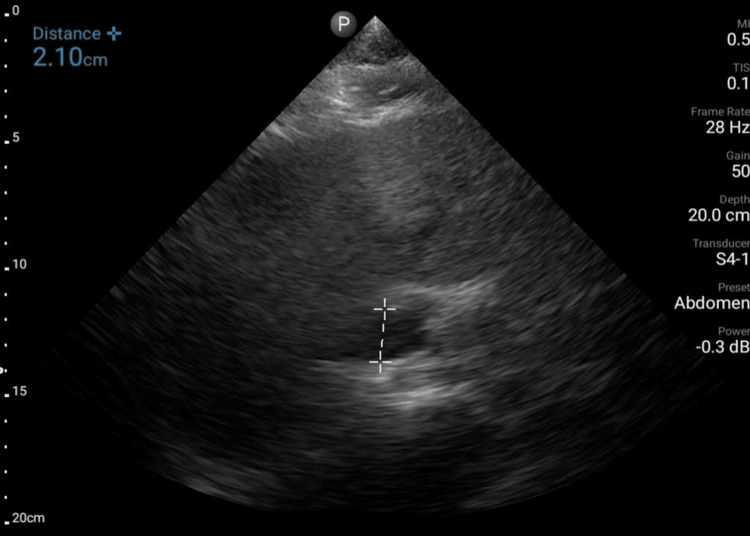 Figure 2
Figure 2| Demographics | All patients | VMT 0 or 1 | VMT 2 or 3 | P-value |
| Number, n (%) | 27 | 16 (59) | 11 (41) | NA |
| Age (years), mean ± SD | 76 ± 12 | 72 ± 12 | 81 ± 12 | 0.095 |
| Female, n (%) | 15 (56) | 8 (50) | 7 (64) | 0.696 |
| Male, n (%) | 12 (44) | 8 (50) | 4 (36) | 0.696 |
| Electrocardiography, n (%) | ||||
| Atrial fibrillation | 9 (33) | 3 (19) | 6 (55) | 0.097 |
| Others | 3 (11) | 1 (6) | 2 (18) | 0.549 |
| Cardiac disease, n (%) | ||||
| History of heart failure | 5 (19) | 1 (6) | 4 (36) | 0.125 |
| Ischemic heart disease | 6 (22) | 2 (13) | 4 (36) | 0.187 |
| Valvular heart disease | 4 (15) | 2 (13) | 2 (18) | >0.999 |
| Comorbidity, n (%) | ||||
| Hypertension | 13 (48) | 8 (50) | 5 (45) | >0.999 |
| Diabetes mellitus | 7 (26) | 4 (25) | 3 (27) | >0.999 |
| Dyslipidemia | 8 (30) | 5 (31) | 3 (27) | >0.999 |
| Chronic kidney disease | 5 (19) | 2 (13) | 3 (27) | 0.371 |
| Purpose, n (%) | ||||
| Heart failure evaluation | 6 (22) | 2 (13) | 4 (36) | 0.187 |
| Post-acute coronary syndrome | 4 (15) | 1 (6) | 3 (27) | 0.273 |
| Preoperative exam | 9 (33) | 8 (50) | 1 (9) | 0.042 |
| Others | 8 (30) | 5 (31) | 3 (27) | >0.999 |
| Sonographer with stationary US | ||||||
| 0 | 1 | 2 | 3 | Total | ||
| Resident with portable US | 0 | 2 | 1 | 0 | 0 | 3 |
| 1 | 2 | 9 | 1 | 0 | 12 | |
| 2 | 0 | 2 | 6 | 1 | 9 | |
| 3 | 0 | 0 | 1 | 2 | 3 | |
| Total | 4 | 12 | 8 | 3 | 27 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiac Valve Diseases and Treatments · Ultrasound in Clinical Applications
Introduction
Heart failure (HF) is a leading cause of hospitalization and requires effective management [1]. Echocardiography plays a vital role in the assessment of patients with HF. Left ventricular (LV) filling pressure (LVFP) is an important parameter in echocardiographic evaluation, with an elevated LVFP being associated with poor clinical outcomes in patients with HF [2]. While the early diastolic opening of the tricuspid valve (TV) precedes that of the mitral valve (MV) in normal conditions [3,4], once LVFP is elevated, MV opening occurs early and precedes TV opening, resulting from the early crossover of the left atrium (LA) and LV pressures [3,5,6]. Reduced right ventricular (RV) relaxation due to post-capillary pulmonary hypertension also accentuates this time sequence [3,7]. Accordingly, early MV opening is considered to reflect the degree of LVFP elevation. Several recent studies have validated that the time delay of TV opening relative to MV opening reflects LVFP in patients with HF [8-11].
The visually assessed time difference between MV and TV opening, the VMT score, has emerged as a promising tool for LVFP estimation using only the B-mode in echocardiography [8-10]. Previous studies have reported that a VMT score of ≥2 was associated with adverse clinical outcomes in patients with HF, showing a wide range of LV ejection fraction [2,12]. Furthermore, the VMT score exhibited high diagnostic accuracy for patients with acute HF presenting with dyspnea, outperforming lung ultrasonography [13]. These findings indicate the potential of the VMT score to improve HF diagnosis and risk stratification.
The recent development of handheld ultrasound (US) devices has the potential to revolutionize the availability and integration of echocardiography into medical practice, particularly for noncardiology medical professionals [14]. However, whether the VMT score can be correctly assessed by beginners in echocardiography and handheld US remains unknown. Therefore, this study aimed to evaluate the interobserver reproducibility of the VMT score between a novice physician using a handheld US device and experienced cardiac sonographers using a standard echocardiography system.
This article was previously posted to the Authoria preprint server on October 6, 2025 [15].
Materials and methods
Study population
We conducted a prospective observational study including adult patients admitted to Wakkanai City Hospital from June to July 2024. We initially enrolled 30 consecutive patients scheduled to undergo echocardiography performed by cardiac sonographers. Patients with poor echocardiographic images were excluded. Ultimately, 27 patients were included in the final analysis. This study was reviewed and approved by the Institutional Ethics Committee of Wakkanai City Hospital (approval number: R6-04; approval date: May 31, 2024).
Echocardiographic examination
Each patient underwent two echocardiographic examinations on the same day within five hours. The resident doctor had performed approximately 30 transthoracic echocardiographic examinations during the six months before this study. First, transthoracic echocardiography was performed by a resident doctor at the bedside using a handheld US (Lumify with S4-1 sector probe, Philips, Amsterdam, the Netherlands) on the hospital ward. Subsequently, a standard transthoracic echocardiography was performed by cardiac sonographers on the same patient in the echocardiography laboratory using a high-end stationary US (EPIQ Elite; Philips Healthcare, Andover, MA, USA) equipped with a 1.0-5.0 MHz phased-array transducer (S5-1). The frame rate was 20-28 Hz for the handheld US system and 52 ± 7 frames per second (fps) (range = 42-67 fps) for the stationary system. The resident and the sonographers were blinded to each other’s findings. Both observers independently evaluated the VMT score for each patient. The VMT score has been evaluated as a marker of elevated LVFP [8-10]. Based on the earlier opening of the MV than the TV when LVFP exceeds right atrial (RA) pressure, the scoring system consists of (i) visual assessment of the time sequence of atrioventricular valve openings and (ii) estimation of RA pressure based on inferior vena cava (IVC). To observe the time sequence of atrioventricular valve opening, apical or subcostal four-chamber images with a depth of 15-20 cm were acquired. Adequate image quality was defined as visualization of both the MV and TV in either the apical or subcostal four-chamber view. To ensure clear delineation of valve motion, the B-mode gain was adjusted to ≥50 whenever possible. The time sequence of the MV and TV opening was visually assessed using slow playback. For each examination, cine loops including at least three cardiac cycles were reviewed frame-by-frame to determine the order of valve opening, and graded as follows: 0 = TV opening first; 1 = simultaneous; 2 = MV opening first (Figure 1). When a marker of abnormal RA pressure (IVC diameter >21 mm with <50% collapse on sniffing) was detected [16], 1 point was added, and the VMT score was calculated as four grades from 0 to 3. Then, VMT ≥2 was considered to indicate an elevated LVFP.
The VMT score was graded as 0 for TV opening first, 1 for simultaneous opening, and 2 for MV opening first.VMT = visually assessed time difference between mitral and tricuspid valve opening; TV = tricuspid valve; MV = mitral valve
Outcome assessment
Other physicians or surgeons confirmed the clinical diagnosis based on physical examination, laboratory data, chest X-ray, electrocardiogram findings, echocardiographic findings other than the VMT score, and the clinical course at follow-up.
Statistical analyses
Continuous variables were expressed as mean ± standard deviation. Student’s t-test was used to compare continuous variables between groups. When appropriate, categorical variables were expressed as numbers (%) and compared using the chi-square test or Fisher’s exact test. Weighted kappa statistics were used to assess interobserver agreement for VMT score grading [17]. As a 2- or 3-point difference in the VMT score between observers represents greater disagreement than a 1-point difference, the weighted kappa was calculated (assigning partial agreement for a 1-point difference) instead of a standard (unweighted) kappa. SPSS version 25 for Windows (IBM Corp., Armonk, NY, USA), R software version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria), and Excel version 2024 (BellCurve for Excel; Social Survey Research Information, Tokyo, Japan) were used for all statistical analyses. For all tests, a p-value <0.05 was considered statistically significant.
Results
Patient characteristics
Table 1 presents the clinical characteristics of the 27 patients stratified by the VMT score. Among them, 16 (59%) had a VMT score of 0 or 1, and 11 (41%) had a score of 2 or 3. Preoperative examinations were more predominant in patients with a VMT score of ≤1. Ischemic heart disease was the most common underlying cardiac disease, and almost half of the patients had hypertension.
Reproducibility of the VMT score
Interobserver agreement analysis was conducted based on the VMT scores determined by the resident (Y.U.) and the cardiac sonographers (N.S., M.S., and K.N.) for each patient who were blinded to the clinical, hemodynamic, and other echocardiographic data. The weighted kappa value was 0.97, indicating an almost-perfect agreement in the VMT grading between the novice and the expert observers (Table 2).
Discussion
This study found that the VMT score can be evaluated with excellent interobserver reproducibility, even when the assessments are conducted by individuals with different levels of US experience and using different echocardiography equipment. The almost-perfect agreement between the resident using a handheld device and the experienced sonographers using a standard machine highlights the robustness of VMT scoring.
Although the interobserver agreement for the VMT score exhibited high reproducibility, discrepancies were observed in 3 out of 27 cases (Table 2), resulting in disagreement in terms of the presence or absence of elevated LVFP. These discrepancies were found to primarily arise from errors in the IVC measurement, where the resident doctor either measured the aorta instead of the IVC or relied on unclear echocardiographic images (Figure 2), leading to incorrect assessment of the RA pressure component. To reduce such misidentification, the use of color Doppler imaging may help differentiate venous flow in the IVC from pulsatile arterial flow in the aorta. In addition, obtaining images from a right intercostal approach or alternative subcostal windows may improve visualization of the IVC and prevent measurement errors, particularly in patients with suboptimal acoustic windows. The findings of this study indicate the potential of VMT scoring as a reliable and reproducible method for LVFP estimation, even for less-experienced practitioners. Moreover, as both handheld and stationary US can accurately measure the VMT score, the VMT score can be evaluated regardless of the type of US device. However, challenges remain, particularly in patients with suboptimal imaging conditions, such as those who are overweight or unable to assume optimal positions. In these cases, the acquisition of clear MV and TV images is difficult, which can compromise accuracy. Although apical and subcostal four-chamber views were effective for VMT score assessment, the incorporation of parasternal views or subcostal window may enhance visualization and accuracy in difficult cases. The simplicity of the VMT score, which does not require Doppler functionality, highlights its utility in resource-constrained settings and its accessibility for clinicians with varying levels of US expertise.
Misinterpreting the aorta instead of IVC.IVC = inferior vena cava
Recently, the American Society of Echocardiography proposed updated 2025 guidelines for LVFP assessment, introducing new algorithms that incorporate multiple indices, including Doppler parameters [18]. Although this new algorithm has been validated against invasive hemodynamic measurements [19] and its prognostic impact in daily practice has been shown [20], it requires complex parameters, such as Doppler indices and left atrial strain. The technical demands and learning curve associated with these measurements make it difficult for noncardiology medical professionals to implement the algorithm in busy primary care or emergency settings. Furthermore, atrial fibrillation (AF) is a common comorbidity whose prevalence increases with advancing age and is frequently associated with HF; for example, more than 30% of patients with HF have AF [21]. Although the 2025 guidelines provide specific algorithms for AF [18,22], these algorithms remain inherently complex and include parameters such as a body mass index (BMI) >30 kg/m². The clinical value of this BMI threshold, which is based on Western populations, remains unclear when applied to Asian populations, where obesity-related phenotypes differ. Contrarily, multicenter studies have shown that the VMT score is an effective and reliable tool even in patients with AF [10,23]. Its reliance on simple B-mode findings rather than complex hemodynamics indicates its significance as a practical imaging biomarker for HF, providing high accessibility for nonspecialists in diverse clinical settings.
Limitations
The present study has several limitations that need to be acknowledged. First, echocardiographic examinations were not performed simultaneously, and the interval between the handheld and stationary scans was up to five hours. In patients with HF, LVFP may change rapidly depending on volume status, treatment, or hemodynamic instability. Therefore, some interobserver disagreement may have been influenced by true physiological variation over time rather than observer-related error. Second, a single resident performed all the handheld scans, whereas the standard examinations were performed by multiple sonographers. While this reflects real-world practice, it could introduce variability in the method. Third, this study focused only on interobserver agreement, and intraobserver reproducibility was not examined. Future studies should assess whether VMT scoring remains consistent when repeated by the same examiner. Fourth, as the study only included patients who were admitted and scheduled for echocardiography, potential selection bias could not be excluded. Finally, the small sample size may have limited the statistical power to detect true differences, increasing the risk of a type II error, particularly when comparing individual groups shown in Table 2. Therefore, larger, multicenter studies and broader patient populations, including outpatients, are warranted to confirm our findings.
Conclusions
VMT scoring demonstrated excellent interobserver reproducibility and may serve as a practical screening or adjunctive tool for LVFP assessment using only B-mode echocardiography, pending further validation studies. It is considered to be valuable for physicians owing to its ease of use and adaptability, regardless of the level of clinical experience or the type of US system available. The use of VMT scoring has the potential to improve HF diagnosis and management in various clinical settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ultrasonography in heart failure: a story that matters Curr Probl Cardiol Mozzini C Cominacini L Casadei A Schiavone C Soresi M 1161364420193017255110.1016/j.cpcardiol.2018.05.003 · doi ↗ · pubmed ↗
- 2Visual echocardiographic scoring system of the left ventricular filling pressure and outcomes of heart failure with preserved ejection fraction Eur Heart J Cardiovasc Imaging Murayama M Iwano H Obokata M 6166262320223469436810.1093/ehjci/jeab 208PMC 9016355 · doi ↗ · pubmed ↗
- 3Prognostic value of time interval between mitral and tricuspid valve opening in patients with heart failure Circ J Sugahara M Mano T Goda A 4014098320193055512610.1253/circj.CJ-18-0999 · doi ↗ · pubmed ↗
- 4Right ventricular function in cardiovascular disease, part I: anatomy, physiology, aging, and functional assessment of the right ventricle Circulation Haddad F Hunt SA Rosenthal DN Murphy DJ 1436144811720081834722010.1161/CIRCULATIONAHA.107.653576 · doi ↗ · pubmed ↗
- 5Relation of transmitral flow velocity patterns to left ventricular diastolic function: new insights from a combined hemodynamic and Doppler echocardiographic study J Am Coll Cardiol Appleton CP Hatle LK Popp RL 426440121988339233610.1016/0735-1097(88)90416-0 · doi ↗ · pubmed ↗
- 6Tricuspid regurgitation occurring in the early-diastolic phase in a case of heart failure: insights from echocardiographic and invasive hemodynamic findings Echocardiography Murayama M Iwano H Tsujinaga S 177117753620193142410910.1111/echo.14458 · doi ↗ · pubmed ↗
- 7Non-invasive estimation of pulmonary artery systolic pressure with Doppler ultrasound Br Heart J Hatle L Angelsen BA Tromsdal A 157165451981745917510.1136/hrt.45.2.157PMC 482504 · doi ↗ · pubmed ↗
- 8Simple two-dimensional echocardiographic scoring system for the estimation of left ventricular filling pressure J Am Soc Echocardiogr Murayama M Iwano H Nishino H 7237343420213367594210.1016/j.echo.2021.02.013 · doi ↗ · pubmed ↗