Exploring the Impact of Professional Acting on Empathy Development in Medical Students
Nino Shiukashvili, Gvantsa Vardosanidze, Mariam Rochikashvili, Nino Tevzadze, Archil Undilashvili, Mary Jo Lechowicz, Eka Ekaladze, Candace Chow, Mariam Rochikashvili, Eng-Koon Ong, Mariam Rochikashvili

TL;DR
A performance-based training program with professional actors significantly improves medical students' empathetic communication skills.
Contribution
This study introduces a novel actor-led training method to enhance empathy in medical students through experiential learning.
Findings
Significant improvements in empathetic communication were observed across all domains after the training.
The largest gains were in verbal expressiveness, non-verbal behavior, and integration of self.
The intervention was well-received and feasible for integration into medical curricula.
Abstract
Empathy is essential to patient-centered care and is linked to improved satisfaction, adherence, and clinical outcomes. Yet, empathy often declines during medical training, and traditional teaching methods may fall short in cultivating observable empathic behaviors. This study evaluated a structured, actor-led training program designed to enhance third-year medical students’ empathetic communication. Eighteen third-year students participated in a four-week, performance-based workshop incorporating role-play, character immersion, and feedback from professional actors and faculty. Empathetic communication was assessed pre- and post-intervention using a 28-item observational checklist across five domains. Paired-sample t-tests were used to evaluate changes. Twelve students completed the full training. Statistically significant improvements were observed across all domains (p < 0.001),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
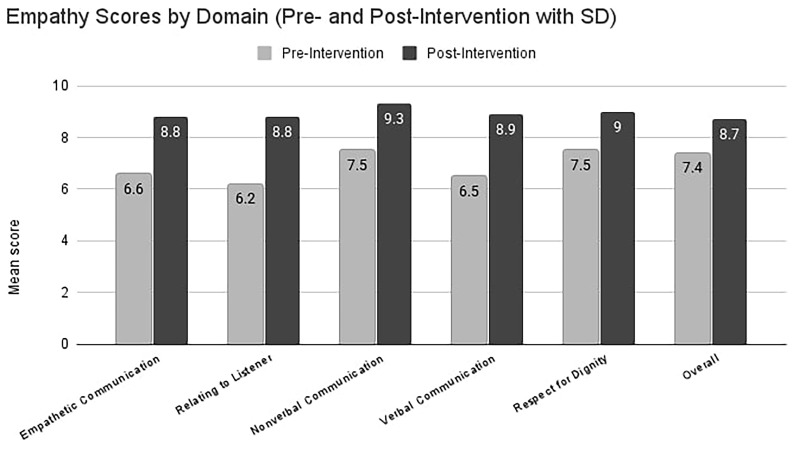 Figure 1
Figure 1| Domain | Pre-test
| Post-test
| Mean
| t-value | df | p-value |
|---|---|---|---|---|---|---|
| Empathetic
| 6.6 (0.85) | 8.8 (0.92) | +2.2 | -8.6 | 11 | <0.001 |
| Relating to Listener | 6.2 (1.03) | 8.8 (1.22) | +2.6 | -7.7 | 11 | <0.001 |
| Non-verbal
| 7.5 (0.98) | 9.3 (0.87) | +1.8 | -5.4 | 11 | <0.001 |
| Verbal Communication | 6.5 (0.96) | 8.9 (0.92) | +2.4 | -9.7 | 11 | <0.001 |
| Respect for Dignity | 7.5 (0.83) | 9.0 (0.70) | +1.5 | -5.3 | 11 | <0.001 |
| Overall | 7.4 (0.88) | 8.7 (0.94) | +1.3 | -5.1 | 11 | <0.001 |
| Questions | Pre-
| Post-
| t-test | p-value |
|---|---|---|---|---|
|
| ||||
| 1. Social sensitivity: displays recognition of differences
| 7.5 (0.98) | 9.7 (0.39) | -8.13 | <0.001 |
| 2. Patience: allows time for full interpersonal
| 6.8 (1.52) | 8.8 (1.25) | -4.14 | 0.002 |
| 3. Tactfulness: displays the ability to recognize and
| 6.1 (1.07) | 8.5 (1.15) | -4.58 | <0.001 |
| 4. Enthusiasm: displays energy and interest in the
| 6.0 (1.81) | 8.3 (1.19) | -5.19 | <0.001 |
| 5. Listening while speaking: displays an ability to
| 6.9 (1.47) | 8.8 (1.29) | -3.97 | 0.002 |
| 6. Integration of self: displays ability to integrate
| 5.1 (1.62) | 8.7 (1.03) | -9.03 | <0.001 |
| 7. Synthesis: integrates an array of emotional,
| 5.9 (1.86) | 8.7 (1.24) | -4.90 | <0.001 |
|
| ||||
| 8. Integrates multiple modes of communication
| 5.7 (1.47) | 8.7 (1.17) | -5.70 | <0.001 |
| 9. Chooses appropriate language/uses medical
| 7.1 (0.71) | 9.1 (1.17) | -6.61 | <0.001 |
| 10. Incorporates patient's questions and responses
| 5.8 (1.73) | 8.8 (1.37) | -6.10 | <0.001 |
| 11. Checks for non-verbal signs of comprehension | 6.1 (1.32) | 8.5 (1.53) | -5.69 | <0.001 |
| 12. Is aware of patient's breath as reflective of
| 6.1 (1.65) | 8.6 (1.66) | -6.82 | <0.001 |
|
| ||||
| 13. Allows for eye contact | 8.0 (1.23) | 9.3 (1.22) | -2.99 | 0.012 |
| 14. Presents an open body posture | 7.8 (0.89) | 9.4 (0.70) | -5.27 | <0.001 |
| 15. Appropriately positions self in relation to patient
| 6.9 (1.21) | 9.3 (0.96) | -6.10 | <0.001 |
|
| ||||
| 16. Articulates words clearly | 7.0 (1.17) | 9.2 (0.93) | -8.18 | <0.001 |
| 17. Chooses effective vocal placement (timbre, tone,
| 6.5 (1.57) | 8.7 (1.14) | -3.83 | 0.003 |
| 18. Projects appropriately/chooses appropriate
| 6.1 (1.62) | 8.9 (0.90) | -7.16 | <0.001 |
| 19. Selects appropriate pace | 6.4 (1.22) | 8.8 (1.08) | -6.33 | <0.001 |
| 20. Provides appropriate wait time for responses after
| 6.6 (1.18) | 8.8 (1.30) | -3.74 | 0.003 |
| 21. Varies delivery approach (e.g pitch, rate, emphasis,
| 6.0 (1.30) | 8.9 (1.10) | -6.29 | <0.001 |
|
| ||||
| 22. Establishes an environment respectful of patient
| 8.2 (0.95) | 9.5 (0.57) | -4.84 | <0.001 |
| 23. Clearly describes illness, condition, and/or
| 7.9 (0.83) | 9.3 (0.96) | -3.47 | 0.005 |
| 24. Solicits active patient participation and
| 6.8 (1.47) | 9.0 (1.14) | -6.44 | <0.001 |
| 25. Asks permission before touching or intruding on
| 6.7 (1.75) | 8.2 (1.56) | -2.60 | 0.025 |
|
| ||||
| 26. Presence | 7.4 (1.15) | 9.2 (0.88) | -4.82 | <0.001 |
| 27. Attentiveness | 7.8 (0.84) | 9.2 (0.84) | -6.27 | <0.001 |
| 28. Physical expressiveness | 6.9 (1.48) | 8.4 (1.38) | -2.77 | 0.018 |
| Student N | Mean Diff (Post-Pre) | t-value | df | p-value |
|---|---|---|---|---|
| 1 | +3.1 | -11.5 | 28 | <0.001 |
| 2 | +2.8 | -9.4 | 28 | <0.001 |
| 3 | +1.1 | -7.0 | 28 | <0.001 |
| 4 | +1.9 | -5.2 | 28 | <0.001 |
| 5 | +2.2 | -7.6 | 28 | <0.001 |
| 6 | +2.9 | -11.8 | 28 | <0.001 |
| 7 | +2.2 | -10.0 | 28 | <0.001 |
| 8 | +2.3 | -12.8 | 28 | <0.001 |
| 9 | +2.6 | -11.6 | 28 | <0.001 |
| 10 | +1.0 | -7.2 | 28 | <0.001 |
| 11 | +0.8 | -2.8 | 28 | 0.008 |
| 12 | +1.7 | -6.0 | 28 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmpathy and Medical Education · Innovations in Medical Education · Education and Critical Thinking Development
Introduction
In an era where artificial intelligence is transforming clinical practice, the human capacity for empathy remains essential to patient-centered care, safeguarding relational and emotional dimensions that technology cannot replicate. Empathy is not merely an internal emotional state of the physician, but a patient-perceived experience of being genuinely acknowledged, heard, and understood ( Archer & Meyer, 2021; Hojat et al., 2011). Patient-perceived empathy has been consistently associated with improved satisfaction, adherence to treatment, and clinical outcomes ( Derksen et al., 2013; Mercer & Reynolds, 2002), including in emotionally complex fields such as oncology, chronic illness, and primary care ( Stepien & Baernstein, 2006).
Empathy is most impactful when conveyed through observable behaviors. Several researches demonstrate that specific verbal and non-verbal cues—such as tone of voice, eye contact, posture, and facial expressions—strongly influence patients’ perceptions ( Riess et al., 2012; Silverman, 2009). This externalization of empathy enables clinicians to translate internal understanding into relational connection through the “integration of self”—the ability to bring authenticity into clinical interactions—which has been shown to deepen trust and strengthen therapeutic relationships ( Kelm et al., 2014). Therefore, fostering empathy in medical students requires moving beyond theoretical understanding toward the intentional development of observable and assessable communication behaviors ( Hemmerdinger et al., 2007).
Despite widespread recognition of its value, empathy tends to decline during medical training—particularly during the transition to clinical years—due to increased workload, emotional fatigue, and decreased emphasis on relational learning ( Chen et al., 2007; Neumann et al., 2011). Conventional teaching methods such as reflective writing and patient narratives, while beneficial, may insufficiently address the behavioral and expressive dimensions of empathy ( Batt-Rawden et al., 2013).
To address these limitations, emerging pedagogical approaches now integrate the arts—especially drama and performance—as tools for empathy cultivation. Arts-based methods promote perspective-taking and emotional regulation through experiential immersion ( Shapiro & Rucker, 2003). Acting techniques that focus on character embodiment and emotional attunement have shown promise in medical training for enhancing interpersonal sensitivity and communication ( Wear & Zarconi, 2008). A recent model by Haider et al. (2024) further emphasizes that patients perceive empathy largely through clinicians’ verbal and non-verbal behaviors, regardless of their internal affective state, supporting the need for behaviorally oriented training.
Accordingly, we implemented a performance-based training intervention, led by professional actors, to enhance the empathetic communication skills of third-year medical students. This study sought to determine (1) whether the intervention led to measurable improvements in empathic communication and (2) which specific behavioral domains exhibited the most significant gains.
Methods
Participants
Sixty third-year medical students from Ken Walker International University were invited to participate in a pilot empathy training program. The university’s six-year MD curriculum includes a pre-medical humanities-focused first year, followed by two years of biomedical sciences, and a clinical phase during the final three years. Third-year students were selected for this study as they had completed foundational training in patient communication, including history-taking and standardized patient encounters.
Eighteen students enrolled on a voluntary basis and were divided into three groups of six. These students participated in a four-week extracurricular workshop. The first session included orientation and baseline empathy assessment, while the following three weeks comprised two sessions per week: an actor-led training workshop and a faculty supervised practice session.
Every student provided written informed consent prior to participation. Ethical approval for the study was obtained from the Ken Walker International University Institutional Review Board, and all procedures were conducted in accordance with the Declaration of Helsinki.
Intervention design
Each week introduced a new emotionally complex clinical scenario, with students alternating roles between physician and patient. The actor-led sessions focused on verbal and non-verbal aspects of communication—tone, posture, facial expression, and gestures. After guided instruction, students engaged in peer role-play and received immediate, personalized feedback from the professional actor.
In the second session of each week, the same scenario was revisited under faculty observation. Students again rotated roles, receiving structured feedback from the faculty physician, peers, and the actor. This multi-source feedback process reinforced skill development across sessions.
Assessment
Students’ communication skills were assessed before and after the program using the Empathetic Communication Assessment Form, a checklist adapted from Dow et al. (2007), which evaluates verbal and non-verbal behaviors across five communication domains. Each item was scored on a 10-point Likert scale (1 = very poor to 10 = excellent).
The final role-play sessions were independently assessed by both the professional actor and faculty physician using the same checklist as the baseline. This allowed for a direct comparison of pre- and post-intervention performance.
Results
Eighteen students enrolled in the intervention, but six were excluded due to incomplete attendance, resulting in a final sample of twelve third-year medical students (58.3% female; mean age = 21.25, SD = 0.75). None had prior acting experience. All twelve participants provided complete data for every outcome; no values were missing.
Paired-sample t-tests showed statistically significant improvements across all domains of empathetic communication (p < 0.001). The largest gains were observed in Relating to the Listener (mean difference = +2.6), Verbal Communication (+2.4), and Empathetic Communication (+2.2). Improvements in Non-verbal Communication, Respect for Dignity, and the Overall Score were also significant ( Table 1; Figure 1).
Mean change in empathy-domain scores before and after training.Light-grey bars show the pre-intervention mean (± 1 SD) for each domain in 12 medical students; hatched dark-grey bars show the post-intervention mean (± 1 SD) after the four-week actor-led workshop. Numeric labels above each bar give the exact group mean. Post-intervention scores were significantly higher than pre-intervention in every domain (paired two-tailed t-tests, all p < 0.001).
All 28 checklist items showed significant score increases, including vocal expressiveness, emotional integration, and positioning relative to the patient. The most substantial change was in “integration of self,” which rose from 5.1 to 8.7 (t = -9.03, p < 0.001) ( Table 2).
Each participant showed statistically significant individual gains (range: +0.8 to +3.1). No gender-based differences were found ( Table 3).
Discussion
This study demonstrated that a structured, actor-led empathy training program significantly improved third-year medical students’ communication across all assessed domains, including verbal and non-verbal behaviors, emotional responsiveness, and integration of self. These findings reinforce the value of performance-based learning in fostering not just the conceptual understanding of empathy, but its practical, observable expression in clinical settings.
Gains in non-verbal behaviors such as eye contact, body posture, and vocal modulation indicate enhanced physical awareness and intentionality in patient encounters. The marked increase in "integration of self" suggests that experiential training can help students bring authenticity to clinical roles, potentially reducing emotional detachment often associated with early clinical exposure.
These results align with previous literature emphasizing the teachability of empathy through structured, reflective, and feedback-rich experiences ( Batt-Rawden et al., 2013; Riess et al., 2012). By incorporating character immersion and dual role-play, the intervention provided students with an emotionally safe space to explore difficult scenarios and develop nuanced interpersonal responses. Unlike traditional approaches focused primarily on cognitive empathy or written reflection, this training offered embodied practice of empathy as a relational act.
The consistency of improvement across all participants suggests the intervention is broadly applicable regardless of baseline communication ability or gender. Although female students showed slightly higher average gains, the difference was not statistically significant, highlighting the inclusivity of the approach.
Despite these promising findings, several limitations warrant consideration. The small sample size and absence of a control group limit generalizability. Additionally, the voluntary nature of participation introduces potential self-selection bias, as students predisposed to valuing communication may have been more likely to enroll. Finally, while immediate improvements were documented, the long-term retention and real-world clinical application of these skills remain to be assessed.
Given the observed benefits and high feasibility, the program will be integrated into the formal third-year curriculum, coinciding with the transition from pre-clinical to clinical training.
Conclusion
This study shows that actor-led empathy training significantly enhances medical students’ ability to convey empathy through both verbal and non-verbal behaviors. Performance-based methods provide a valuable, scalable approach to cultivating emotionally attuned and communicatively skilled physicians. Future studies should examine whether these improvements persist longitudinally and translate into enhanced patient care during real-world clinical practice.
Ethics approval
This study received ethics approval from Biomedical Research Ethics Committee at Ken Walker International University (Approval Number: #1-2024/001). All procedures complied with institutional guidelines and the principles of the Declaration of Helsinki.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Archer R Meyer EC : Empathy in patient care: from clinical communication to therapeutic alliance. J Gen Intern Med. 2021;36(4):1123–1130.33432432
- 2Batt-Rawden SA Chisolm MS Anton B : Teaching empathy to medical students: an updated, systematic review. Acad Med. 2013;88(8):1171–1177. 10.1097/ACM.0b 013e 318299 f 3e 3 23807099 · doi ↗ · pubmed ↗
- 3Chen DC Lew R Hershman W : A cross-sectional measurement of medical student empathy. J Gen Intern Med. 2007;22(10):1434–1438. 10.1007/s 11606-007-0298-x 17653807 PMC 2305857 · doi ↗ · pubmed ↗
- 4Derksen F Bensing J Lagro-Janssen A : Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63(606):e 76–e 84. 10.3399/bjgp 13X 660814 23336477 PMC 3529296 · doi ↗ · pubmed ↗
- 5Dow AW Leong D Anderson A : Using theater to teach clinical empathy: a pilot study. J Gen Intern Med. 2007;22(8):1114–1118. 10.1007/s 11606-007-0224-2 17486385 PMC 2305755 · doi ↗ · pubmed ↗
- 6Haider AS Siddiqui H Ahmed W : A multidimensional model of clinical empathy: evaluating verbal and non-verbal contributors to patient perception. Med Teach. 2024; [Epub ahead of print].
- 7Hemmerdinger JM Stoddart SDR Lilford RJ : A systematic review of tests of empathy in medicine. BMC Med Educ. 2007;7: 24. 10.1186/1472-6920-7-24 17651477 PMC 1988794 · doi ↗ · pubmed ↗
- 8Hojat M Louis DZ Markham FW : Physicians' empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–364. 10.1097/ACM.0b 013e 3182086 fe 1 21248604 · doi ↗ · pubmed ↗