Giant cell arteritis–associated temporomandibular joint arthritis confirmed by imaging
Miyu Wakatsuki, Hiroyuki Yamashita, Ami Isoda, Takuya Harada, Hiroshi Kaneko

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
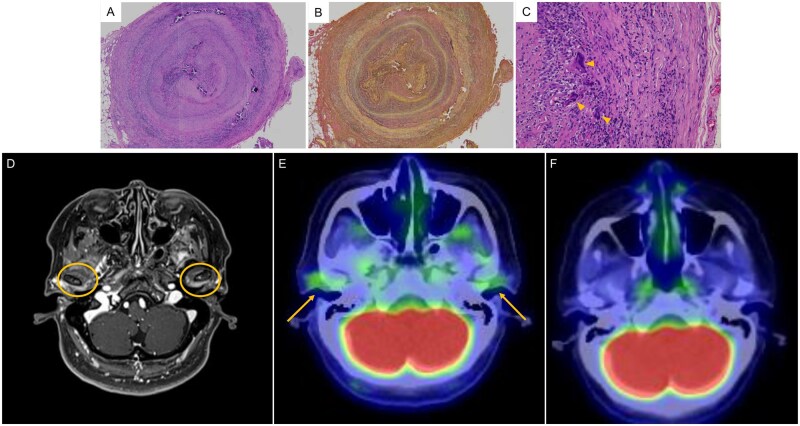 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · IgG4-Related and Inflammatory Diseases · Otitis Media and Relapsing Polychondritis
Dear Editor, Giant cell arteritis (GCA) is a large-vessel vasculitis that typically presents with headache and jaw claudication. As GCA can result in blindness, early diagnosis and prompt initiation of treatment are crucial [1]. Patients with GCA may also present with reduced jaw opening (i.e. trismus) [2], but trismus is rarely recognized as a symptom of GCA and is often misattributed to other causes, resulting in diagnostic delay [3]. There is long-standing uncertainty regarding the mechanism of underlying trismus in GCA. This case report describes a patient with GCA initially presenting as trismus, while both MRI and FDG-PET/CT demonstrated enhancement of the temporomandibular joint (TMJ), indicating TMJ arthritis.
A 78-year-old woman presented with a 1-month history of trismus, which was initially diagnosed with TMJ arthritis and treated with antibiotics by dental and otolaryngology specialists, without resolution of symptoms. Afterwards, the patient developed low-grade fever and scalp tenderness, as well as diplopia for 1 week, prompting admission to our hospital for further evaluation. Upon admission, there was mild dilatation and tenderness of the temporal artery, left abducens nerve palsy, pain in both TMJ regions, and trismus (maximum unassisted mouth opening: 28 mm). Laboratory tests showed elevated C-reactive protein (CRP) (10.05 mg/dl) and ESR (>120 mm/h). Temporal artery ultrasound revealed a halo sign. Contrast-enhanced T1-weighted MRI demonstrated high signal intensity in the superficial temporal artery with a corresponding high signal on diffusion-weighted imaging, suggestive of GCA. Temporal artery biopsy revealed marked inflammatory cell infiltration of the vessel wall, severe wall thickening with near luminal occlusion, disruption of the internal elastic lamina, and occasional multinucleated giant cells, leading to the diagnosis of GCA (Fig. 1A–C). Notably, contrast-enhanced T1-weighted MRI revealed high signal intensity in the posterior wall of the TMJ (Fig. 1D), and the TMJ also had increased fluorodeoxyglucose uptake on FDG-PET/CT (Fig. 1E). These findings implicate TMJ arthritis as the cause of trismus. Other potential causes of TMJ inflammation, including inflammatory arthritis (e.g. rheumatoid arthritis and infectious arthritis), were considered. However, the absence of arthritis in other joints, negative rheumatoid serology, imaging findings, and the clinical course made these diagnoses unlikely. Treatment was started with intravenous methylprednisolone pulse therapy (250 mg daily for 3 days), followed by oral prednisolone (40 mg). Afterwards, there was prompt resolution of headache, TMJ arthritis, and trismus along with decreased CRP levels. The patient was discharged on day 20. Follow-up FDG-PET/CT at 3 months was performed to assess overall disease activity of GCA and to evaluate for newly developed vascular involvement or alternative diagnoses. The scan revealed complete resolution of fluorodeoxyglucose uptake in the TMJ (Fig. 1F), with no abnormal FDG uptake elsewhere.
Unlike jaw claudication, trismus is a rare symptom of GCA, observed in only 6.8% of cases [2]. Trismus has previously been associated with the ocular manifestations of GCA, but another study found no such relationship [4]. Diplopia, which arises from ischaemia of the branches of the ophthalmic artery, occurs in 5–10% of patients with GCA [5] and serves as a warning sign preceding blindness [6]. In this case, the patient developed diplopia after trismus due to abducens nerve palsy. Previous reports of GCA presenting with trismus noted a diagnostic delay of 1–2 months, with symptom improvement after prednisolone therapy [7, 8].
Trismus in GCA is often overlooked, and its underlying mechanism remains unclear. Some hypotheses include ischaemia of the maxillary artery supplying the masseter muscle, as well as involvement of the trigeminal and facial nerves [7, 8]. To our knowledge, this is the first report of GCA presenting with trismus and evidence of TMJ arthritis on both FDG-PET/CT and MRI. The TMJ is supplied by branches of the external carotid artery, such as the superficial temporal and maxillary arteries [9], which are often involved in giant cell arteritis. In the present case, imaging confirmed that inflammatory changes were localized to the TMJ. These findings support the possibility that localized inflammatory TMJ arthritis associated with GCA may contribute to trismus. In conclusion, trismus should be recognized as a possible clinical manifestation of GCA, wherein localized TMJ arthritis is a potential underlying mechanism.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ponte C , Grayson PC, Robson JC et al; DCVAS Study Group. American College of Rheumatology/EULAR classification criteria for giant cell arteritis. Arthritis Rheumatol 2022;74:1881–9.36350123 10.1002/art.42325 · doi ↗ · pubmed ↗
- 2Nir-Paz R , Gross A, Chajek-Shaul T. Reduction of jaw opening (trismus) in giant cell arteritis. Ann Rheum Dis 2002;61:832–3.12176811 10.1136/ard.61.9.832PMC 1754221 · doi ↗ · pubmed ↗
- 3Lim J , Dures E, Bailey LF et al Jaw claudication and jaw stiffness in giant cell arteritis: secondary analysis of a qualitative research dataset. Rheumatol Adv Pract 2024;8:rkad 082.38152390 10.1093/rap/rkad 082PMC 10751230 · doi ↗ · pubmed ↗
- 4Liozon E , Jauberteau MO, Ly K et al Reduction of jaw opening in giant cell arteritis. Ann Rheum Dis 2003;62:287–8; author reply 288.
- 5Héron E , Sedira N, Dahia O, Jamart C. Ocular complications of giant cell arteritis: an acute therapeutic emergency. J Clin Med 2022;11:1997.35407604 10.3390/jcm 11071997 PMC 8999894 · doi ↗ · pubmed ↗
- 6Biousse V , Newman NJ. Ischemic optic neuropathies. N Engl J Med 2015;372:2428–36.26083207 10.1056/NEJ Mra 1413352 · doi ↗ · pubmed ↗
- 7Hasegawa E , Kurosawa Y, Wakamatsu A et al Giant cell arteritis that presented with buccal skin ulceration along the facial artery. Intern Med 2023;62:1541–5.36198595 10.2169/internalmedicine.0395-22PMC 10258095 · doi ↗ · pubmed ↗
- 8Kraemer M , Metz A, Herold M, Venker C, Berlit P. Reduction in jaw opening: a neglected symptom of giant cell arteritis. Rheumatol Int 2011;31:1521–3.21161530 10.1007/s 00296-010-1690-0 · doi ↗ · pubmed ↗