Persistent peristomal pain due to an exposed cutaneous nerve
Iain Noel Encarnacion, Kaylin Beiter, Natasha Hakkal, Emily Hejazi, Paul Hernandez, Melissa Laughter, Shannon Nugent, Samir Thaker, Xiaowei Xu, Misha Rosenbach

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1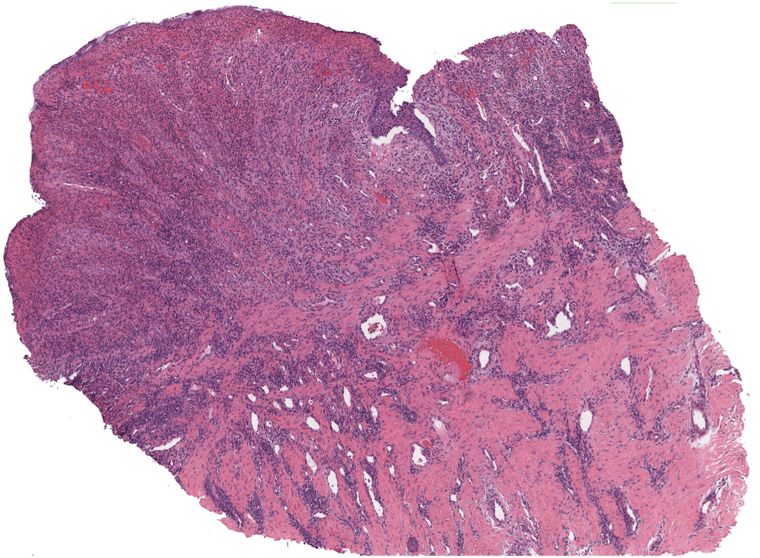 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStoma care and complications · Pain Management and Opioid Use · Myasthenia Gravis and Thymoma
Case description
A 25-year-old woman with a history of ulcerative colitis treated with multiple abdominal surgeries complicated by peristomal pyoderma gangrenosum (PPG) presented with severe peristomal pain and ulceration. Treatment course was complicated; disease control was achieved via combination infliximab 10 mg/kg every 4 weeks, corticosteroids (topical triamcinolone 0.1% ointment, intralesional 10 mg/ml injections, and oral prednisone 30 mg daily with a gradual taper), and cyclosporine 125 mg tapering by 25 mg every 3 weeks, ultimately tapered to infliximab monotherapy.
Four months later, she proceeded with diverting loop ileostomy and bolster placement complicated by PPG flare at the new stomal site. Physical exam revealed erythema and ulcerations at 3 and 9 o’clock positions, along with peristomal skin breakdown and appliance leakage (Fig 1, A and B). Infectious and intra-abdominal etiologies were excluded. PPG improved with corticosteroids (systemic, topical, and intralesional) and infliximab.Fig 1A, Concave ostomy site requiring a bolster, which placed additional focal pressure on the lateral aspects of the peristomal skin. B, Active peristomal pyoderma gangrenosum with cribriform scarring and erythematous ulcerations at the 3 and 9 o’clock positions. C, Peristomal site with no active pyoderma gangrenosum inflammation, cribriform scarring around the periphery at sites of previously active PPG, and a pinpoint papule at the 3 o’clock position (black arrow). PPG, Peristomal pyoderma gangrenosum.
Though her ulcer improved with rapid initiation with oral steroids, she continued to experience intractable, stabbing/burning 10/10 lancing pain localized to a pinpoint papule in the 3 o’clock position (Fig 1, C). This pain was reproducible to light touch and refractory to immunosuppressants and systemic analgesics including gabapentin and opioids.
Question: Which of the following is an appropriate next step in management for this scenario?
- **A.**Increase systemic immunosuppression
- **B.**Inject intralesional lidocaine at tender site
- **C.**Initiate long-acting opioid therapy
- **D.**Begin topical calcineurin inhibitor
- **E.**Perform debridement of peristomal tissue
Answer discussion
Answer: B.
Given the resolution of inflammation with persistent, reproducible pinpoint pain, a neuropathic source such as an exposed cutaneous nerve or traumatic neuroma should be considered. Diagnostic administration of intralesional lidocaine is a simple bedside maneuver that can confirm a nerve-mediated pain source when immediate but transient relief occurs.
For this patient, test administration of 0.1 mL intralesional lidocaine directly into the lesion resulted in immediate pain resolution. The return of her pain approximately 3 hours later after the anesthetic wore off further supported a nerve-mediated source. Nerve block with liposomal bupivacaine provided short-lived benefit, and ultimately punch excision under local anesthesia resulted in sustained pain relief and discontinuation of all analgesia. While the histologic features of the excised tissue are nonspecific and consistent with common features seen adjacent to chronic ulcers (Fig 2), the marked response to anesthetics and pain resolution post-excision supports the clinical diagnosis of an exposed cutaneous nerve as the pain source.Fig 24× magnification of punch biopsy with fibrosis, sparse mixed dermal inflammatory cell infiltrate composed of neutrophils, lymphocytes, plasma cells, and histiocytes, and epidermal hyperplasia, which are common features adjacent to chronic ulcers.
Ulcer management, including as with PPG, is complex and requires a multipronged approach including immunosuppression, wound care, and pain control.1 The ulcer-associated pain should be monitored over the course of wound healing; persistent or disproportionate pain should prompt consideration for alternate etiologies, such as incompletely controlled underlying pathology (eg, pyoderma gangrenosum reactivation), superimposed infection, or other complications.
A percutaneous nerve/neuroma is a non-neoplastic proliferation of an injured nerve, which can arise as a response to trauma (eg, postsurgical or chronic inflammation) as the skin attempts to heal, causing localized hypersensitivity or allodynia.2 Trauma can lead to maladaptive alterations in cutaneous nociceptive signaling, resulting in sensitization and ectopic firing of peripheral nerve endings, leading to exaggerated afferent input to central nervous system pathways.3
Early recognition of neuropathic pain in similar patients is critical to improve quality of life and reduce unnecessary systemic immunosuppression and analgesia.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maverakis E.Marzano A.V.Le S.T.Pyoderma gangrenosum Nat Rev Dis Primers 6120208110.1038/s 41572-020-0213-x 33033263 · doi ↗ · pubmed ↗
- 2Yang H.Dong Y.Wang Z.Traumatic neuromas of peripheral nerves: diagnosis, management and future perspectives Front Neurol 132023103952910.3389/fneur.2022.1039529 PMC 987502536712443 · doi ↗ · pubmed ↗
- 3Stucky C.L.Mikesell A.R.Cutaneous pain in disorders affecting peripheral nerves Neurosci Lett 765202113623310.1016/j.neulet.2021.136233 PMC 857981634506882 · doi ↗ · pubmed ↗