The cervico‐vaginal DNA methylation WID‐qEC test: An epigenetic marker associated with ovarian cancer in the absence of endometrial and cervical cancer
Elisa Redl, Chiara Herzog, Charlotte Vavourakis, James Barrett, Allison Jones, Iona Evans, Daniel Reisel, Ranjit Manchanda, Line Bjørge, Michal Zikan, David Cibula, Twana Alkasalias, Angelique Flöter Rådestad, Kristina Gemzell‐Danielsson, Louis Dubeau, Nicola MacDonald

TL;DR
A DNA methylation test originally for cervical and endometrial cancers also shows potential for detecting ovarian cancer in some cases.
Contribution
The study identifies a link between WID-qEC test positivity and ovarian cancer risk in the absence of other gynecological cancers.
Findings
WID-qEC positivity was associated with ovarian cancer (adjusted OR 2.93).
Positivity was also linked to more lifetime ovulatory cycles (adjusted OR 2.67).
WID-qEC could be used in a two-step triage approach for ovarian cancer detection.
Abstract
The DNA methylation‐based WID‐qEC test, applied to cervico‐vaginal samples, has been validated for the accurate detection of endometrial and cervical cancers. However, a small proportion of women test positive despite the absence of these cancers. The aim of this study was to explore the biological and clinical characteristics associated with such WID‐qEC‐positive cases to inform potential follow‐up strategies. We analyzed 1269 cervico‐vaginal samples from women without endometrial or cervical cancer, including healthy controls (n = 624), women with benign gynecological conditions (n = 324), and ovarian cancer cases (n = 321). Of the 80 WID‐qEC‐positive results, 43 (54%) were from women with ovarian cancer. WID‐qEC positivity was associated with the presence of ovarian cancer (adjusted odds ratio [OR] 2.93; 95% CI 1.75–4.95) and with a higher number of lifetime ovulatory cycles…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
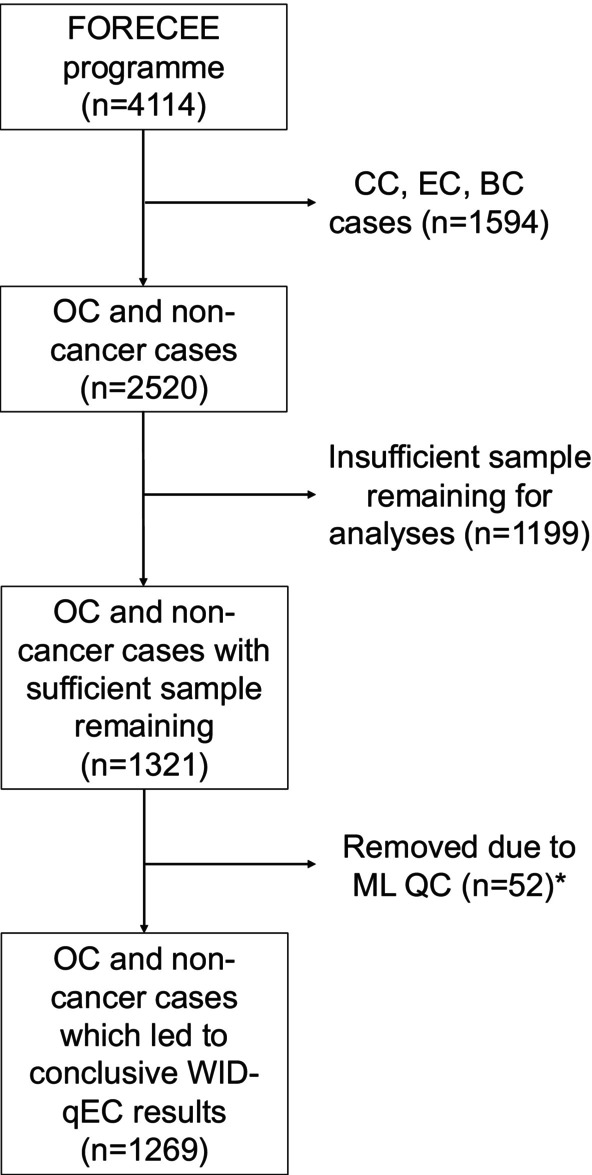 FIGURE 1
FIGURE 1| Total | WID‐qEC negative | WID‐qEC positive | Odds ratio |
| Odds ratio (adjusted) | Adjusted | |
|---|---|---|---|---|---|---|---|
| Age | 1269 | 51.2 (20.1) | 57.8 (14.8) |
|
|
|
|
| BMI (kg/m2) | |||||||
| Healthy (18.5–24.9) | 631 | 596 (50.13) | 35 (43.75) | 1 (reference) | — | 1 (reference) | — |
| Underweight (<18.5) | 50 | 47 (3.95) | 3 (3.75) | 1.09 (0.26–3.17) | 0.893 | 1.16 (0.26–3.61) | 0.816 |
| Overweight (25–29.9) | 344 | 320 (26.91) | 24 (30) | 1.28 (0.74–2.17) | 0.372 | 1.18 (0.67–2.05) | 0.569 |
| Obese (>30) | 239 | 222 (18.67) | 17 (21.25) | 1.3 (0.7–2.34) | 0.386 | 1.16 (0.61–2.13) | 0.636 |
| Missing or unknown | 5 | 4 (0.34) | 1 (1.25) | — | — | — | — |
| Menopausal status | |||||||
| Premenopausal | 598 | 570 (47.94) | 28 (35) | 1 (reference) | — | 1 (reference) | — |
| Postmenopausal | 659 | 608 (51.14) | 51 (63.75) |
|
| 0.45 (0.2–1) | 0.051 |
| Missing or unknown | 12 | 11 (0.93) | 1 (1.25) | — | — | — | — |
| Hormone replacement therapy | |||||||
| Never | 1097 | 1030 (86.63) | 67 (83.75) | 1 (reference) | — | 1 (reference) | — |
| <5 years | 106 | 99 (8.33) | 7 (8.75) | 1.09 (0.44–2.28) | 0.839 | 1.15 (0.45–2.54) | 0.749 |
| ≥5 years | 61 | 56 (4.71) | 5 (6.25) | 1.37 (0.47–3.23) | 0.512 | 0.91 (0.29–2.33) | 0.852 |
| Missing or unknown | 5 | 4 (0.34) | 1 (1.25) | — | — | — | — |
| First degree relatives with breast cancer | |||||||
| No | 1112 | 1035 (87.05) | 77 (96.25) | 1 (reference) | — | 1 (reference) | — |
| Yes | 157 | 154 (12.95) | 3 (3.75) |
|
|
|
|
| First degree relatives with ovarian cancer | |||||||
| No | 1193 | 1117 (93.94) | 76 (95) | 1 (reference) | — | 1 (reference) | — |
| Yes | 75 | 71 (5.97) | 4 (5) | 0.83 (0.25–2.07) | 0.720 | 0.88 (0.26–2.27) | 0.816 |
| Missing or unknown | 1 | 1 (0.08) | 0 (0) | — | — | — | — |
| Estimated lifetime ovulatory cycles | |||||||
| <191 | 297 | 290 (24.39) | 7 (8.75) | 1 (reference) | — | 1 (reference) | — |
| 191–315 | 298 | 283 (23.8) | 15 (18.75) | 2.2 (0.91–5.82) | 0.091 | 1.67 (0.67–4.52) | 0.285 |
| 316–404 | 300 | 279 (23.47) | 21 (26.25) |
|
| 1.74 (0.7–4.8) | 0.254 |
| ≥404 | 300 | 266 (22.37) | 34 (42.5) |
|
|
|
|
| Missing or unknown | 74 | 71 (5.97) | 3 (3.75) | — | — | — | — |
| Current ovarian cancer | |||||||
| No | 948 | 911 (76.62) | 37 (46.25) | 1 (reference) | — | 1 (reference) | — |
| Yes | 321 | 278 (23.38) | 43 (53.75) |
|
|
|
|
| Total | Control | Cancer | Odds ratio |
| Odds ratio (adjusted) | Adjusted | |
|---|---|---|---|---|---|---|---|
| Age | 1269 | 49.8 (18.3) | 59.9 (17.1) |
|
|
|
|
| BMI (kg/m2) | |||||||
| Healthy (18.5–24.9) | 631 | 487 (51.37) | 144 (44.86) | 1 (reference) | — | 1 (reference) | — |
| Underweight (<18.5) | 50 | 33 (3.48) | 17 (5.3) | 1.74 (0.92–3.18) | 0.076 |
|
|
| Overweight (25–29.9) | 344 | 257 (27.11) | 87 (27.1) | 1.14 (0.84–1.55) | 0.386 | 0.93 (0.66–1.3) | 0.679 |
| Obese (>30) | 239 | 170 (17.93) | 69 (21.5) | 1.37 (0.98–1.92) | 0.065 | 1 (0.69–1.44) | 0.990 |
| Missing or unknown | 5 | 1 (0.11) | 4 (1.25) | — | — | — | — |
| Menopausal status | |||||||
| Premenopausal | 598 | 529 (55.8) | 69 (21.5) | 1 (reference) | — | 1 (reference) | — |
| Postmenopausal | 659 | 411 (43.35) | 248 (77.26) |
|
|
|
|
| Missing or unknown | 12 | 8 (0.84) | 4 (1.25) | — | — | — | — |
| Hormone replacement therapy | |||||||
| Never | 1097 | 824 (86.92) | 273 (85.05) | 1 (reference) | — | 1 (reference) | — |
| <5 years | 106 | 86 (9.07) | 20 (6.23) | 0.7 (0.41–1.14) | 0.170 |
|
|
| ≥5 years | 61 | 37 (3.9) | 24 (7.48) |
|
| 0.88 (0.48–1.57) | 0.658 |
| Missing or unknown | 5 | 1 (0.11) | 4 (1.25) | — | — | — | — |
| First degree relatives with breast cancer | |||||||
| No | 1112 | 829 (87.45) | 283 (88.16) | 1 (reference) | — | 1 (reference) | — |
| Yes | 157 | 119 (12.55) | 38 (11.84) | 0.94 (0.63–1.37) | 0.737 | 0.83 (0.54–1.26) | 0.391 |
| First degree relatives with ovarian cancer | |||||||
| No | 1193 | 893 (94.2) | 300 (93.46) | 1 (reference) | — | 1 (reference) | — |
| Yes | 75 | 54 (5.7) | 21 (6.54) | 1.16 (0.67–1.92) | 0.582 | 1.07 (0.6–1.86) | 0.814 |
| Missing or unknown | 1 | 1 (0.11) | 0 (0) | — | — | — | — |
| Estimated lifetime ovulatory cycles | |||||||
| <191 | 297 | 272 (28.69) | 25 (7.79) | 1 (reference) | — | 1 (reference) | — |
| 191–315 | 298 | 246 (25.95) | 52 (16.2) |
|
| 1.68 (1–2.9) | 0.055 |
| 316–404 | 300 | 205 (21.62) | 95 (29.6) |
|
|
|
|
| ≥404 | 300 | 178 (18.78) | 122 (38.01) |
|
|
|
|
| Missing or unknown | 74 | 47 (4.96) | 27 (8.41) | — | — | — | — |
| WID‐qEC | |||||||
| Negative | 1189 | 911 (96.1) | 278 (86.6) | 1 (reference) | — | 1 (reference) | — |
| Positive | 80 | 37 (3.9) | 43 (13.4) |
|
|
|
|
- —The Eve Appeal
- —Land Tirol
- —Horizon 2020 Framework Programme10.13039/100010661
- —European Research Council10.13039/501100000781
- —Standortagentur Tirol10.13039/501100011035
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpigenetics and DNA Methylation · Cervical Cancer and HPV Research · Endometrial and Cervical Cancer Treatments
INTRODUCTION
1
The Women's Cancer Risk Identification – quantitative polymerase chain reaction test for endometrial cancer (WID‐qEC) is a molecular assay that evaluates DNA methylation of the ZSCAN12 and GYPC genes.1, 2, 3, 4, 5 The WID‐qEC test utilizes PCR reactions against the fully methylated alleles of CpG island regions within these two genes, with primers and probes covering 10 and 8 cytosines within the CpG dinucleotide context, respectively. The summed percentage of fully methylated reference (∑PMR) values for both genes determines the test result, with a ∑PMR ≥0.3 considered positive.3, 4, 5 The WID‐qEC test has demonstrated 91%–100% sensitivity for detecting endometrial and cervical cancers,1, 2, 3, 4, 5 with a reported false‐positive rate of 2.7% in a prospective cohort of 399 women ≥45 years of age with abnormal uterine bleeding (AUB).3 In the same prospective study, endometrial thickness of >3 mm measured with transvaginal ultrasound had a false‐positive rate of 54.2%.3
The WID‐qEC test is currently offered to women aged 45 years and older who present with AUB or postmenopausal bleeding (PMB), to identify those at highest risk of endometrial cancer and prioritize them for urgent hysteroscopy and curettage. Effective clinical implementation of the WID‐qEC test will benefit from clear guidance on managing positive test results when neither endometrial nor cervical cancer is detected.
A non‐negligible subset of women diagnosed with ovarian cancer present with AUB: In a case–control study of ovarian carcinoma, 13% and 15% of women with localized and regional disease reported AUB in the year leading up to diagnosis, making it one of the most predictive symptoms alongside abdominal pain and palpable mass.6 Among 43,756 Danish women with PMB, the standardized incidence ratio (SIR) comparing the observed ovarian cancer incidence with that expected in the general population was highly elevated during 0–3 months (SIR = 21.17 [95% CI: 22.47–32.56]) after hospital presentation and remained high in the following 3–12 months (SIR = 3.91 [95% CI: 2.88–5.18]) and 1–5 years (SIR = 1.45 [95% CI: 1.14–1.80]).7 Given these observations, we sought to explore whether WID‐qEC positivity in the absence of endometrial or cervical cancer might correlate with ovarian cancer presence or risk factors such as lifetime ovulatory cycles. This exploratory work was not designed to evaluate the WID‐qEC test as a diagnostic tool for ovarian cancer.
MATERIALS AND METHODS
2
Here, we analyzed the WID‐qEC test in 1269 cervico‐vaginal samples from women without endometrial or cervical cancer. Women were recruited as part of the FORECEE (Female cancer predictiOn using ceRvical omics to individualisE sCreEning and prEvention) programme,8 which aimed to develop predictive tests for breast,9 ovarian,10 and endometrial11 cancers using cervico‐vaginal samples. In total, the sample set included 624 controls from women in cervical screening programs; 324 controls from women with benign/borderline conditions (48 endometriosis/adenomyosis, 72 uterine fibroids, 123 benign adnexal masses, and 81 borderline tumors); and 321 samples from women newly diagnosed with ovarian cancer and prior to any treatment (217 high‐grade serous, 24 low‐grade serous, 16 mucinous, 19 endometrioid, 24 clear cell ovarian cancers, 5 ovarian carcinosarcomas, 14 non‐epithelial malignant tumors, and 2 other malignant ovarian tumors).
Cervico‐vaginal samples were collected using Cervex brushes (Rovers Medical Devices) and preserved in ThinPrep™/PreservCyt™ (Hologic) solution. Only samples with sufficient DNA remaining in the FORECEE biobank were included (Figure 1).
*Composition of the study population with exclusion criteria. WID‐qEC was attempted but insufficient DNA was available to reach a conclusive result. BC, breast cancer; CC, cervical cancer; EC, endometrial cancer; ML, MethyLight; OC, ovarian cancer; QC, quality control.
After bisulfite conversion of the DNA, both target regions (ZSCAN12 and GYPC) and a reference region (COL2A1)—which lacks CpG sites and serves as a human DNA input control and a bisulfite conversion efficiency control—were amplified using one duplex and one singleplex qPCR reaction. Samples were analyzed in technical replicates, and the test result was expressed as the ∑PMR value, calculated as previously described.3, 4, 5 Lifetime ovulatory cycle numbers were determined by calculating the number of months between menarche and the last menstrual cycle, subtracting months of pregnancy and oral contraceptive use. All data are available in Table S1.
RESULTS AND DISCUSSION
3
A total of 6.3% (80/1269) of samples were WID‐qEC positive (Table 1), This includes 2.9% (18/624) of women in cervical screening programs, 5.9% (19/324) of women with benign conditions or borderline tumors, and 13.4% (43/321) of women with malignant ovarian tumors (Table 2). The vast majority of ovarian cancers (300 out of 321; 93.5%) were classified as serous, mucinous, endometrioid, or clear cell subtypes.
Age, menopausal status, family history of breast cancer, lifetime ovulatory cycles, and the presence of ovarian cancer were associated with WID‐qEC positivity in an unadjusted logistic regression analysis. After adjusting for all factors, only age (adjusted OR: 1.04; 95% CI: 1.00–1.07), family history of breast cancer (adjusted OR: 0.26; 95% CI: 0.06–0.71), the top quartile of lifetime ovulatory cycles (adjusted OR: 2.67; 95% CI: 1.06–7.50), and ovarian cancer presence (adjusted OR: 2.93; 95% CI: 1.75–4.95) remained significant. Neither body mass index (BMI) nor hormone replacement therapy was significantly associated with WID‐qEC positivity (Table 1). Overall, the presence of ovarian cancer was the strongest predictor of a WID‐qEC positive result (54% [43/80] and adjusted OR 2.95; 95% CI: 1.78–4.93; Table 2).
Among patients with epithelial ovarian cancer, cervico‐vaginal WID‐qEC positivity was observed in 13.3% (32/241) of serous, 12.5% (2/16) of mucinous, 10.5% (2/19) of endometrioid, and 16.7% (4/24) of clear cell subtypes.
The WID‐qEC test was developed for the early detection of endometrial cancer, where aberrant DNA methylation is predominantly present in cancerous compared to normal endometrial tissue.1 Hence, WID‐qEC positivity in a patient with ovarian cancer could suggest tumor DNA drainage via the fallopian tubes and uterus, as previously proposed by researchers assessing somatic genetic alterations.12, 13 However, given that the number of lifetime ovulatory cycles, a well‐established ovarian cancer risk factor,14, 15, 16, 17 remained an independent predictor of WID‐qEC positivity, even after adjusting for ovarian cancer presence and other covariates, we cannot exclude the possibility that WID‐qEC positivity may reflect underlying ovarian cancer risk rather than merely the presence of tumor‐derived DNA. This raises the hypothesis that WID‐qEC may act as a biological readout of cumulative ovulatory exposure in women predisposed to develop ovarian cancer.
In summary, we found that WID‐qEC positivity, in the absence of endometrial or cervical cancer, serves as a biological readout of lifetime ovulatory cycles and independently detects or predicts ovarian cancer. Because this study used a case–control design enriched for ovarian cancer, the observed associations cannot be extrapolated to population‐level performance or clinical screening metrics.
The study's limitations include incomplete information on menopausal status and lifetime ovulatory cycles, as well as the inherent challenges associated with case–control study designs. Additional limitations include the absence of direct comparison with serum biomarkers such as CA‐125 or HE4, which was beyond the scope of this study focused on understanding WID‐qEC false positives. Future studies could explore these relationships where appropriate.
The following calculation is presented purely to illustrate theoretical implications for research. It does not represent a clinical recommendation, and future modeling or prospective validation would be required to determine any practical triage value. Based on a nationwide Danish cohort study, the annual prevalence of ovarian cancer in women with PMB is 0.38%.7 While we did not record symptoms in the FORECEE study, under the assumption that the sensitivity of 13.4% and 3.9% false positive rate of the WID‐qEC test described in Table 2 apply to a hypothetical population of 10,000 women with PMB (38 OCs, 9962 controls), this would yield 5.1 true positives (38 × 13.4%) and 388.5 false positives (9962 × 3.9%), with a positive predictive value (PPV) of 1.29%. Although this PPV would not justify diagnostic procedures, women presenting with AUB and a positive WID‐qEC in the absence of endometrial or cervical cancer could be recommended additional triage with plasma‐based cell‐free DNA methylation,18 or any other test with an extremely high specificity.19, 20 In a symptomatic population, the Galleri® test for instance has a sensitivity of 64.3% and a specificity of 98.4%,18 and will refine true positives to 3.3 (5.1 × 64.3%) and false positives to 6.2 (388.5 × 1.6%), resulting in a PPV of 34.5%. This would suggest that in women presenting with AUB that have both a positive WID‐qEC test and a positive plasma cell‐free DNAme test, around three patients have to undergo an intraperitoneal procedure to detect one ovarian cancer.
Future studies utilizing cohort‐based cervical biobanks with long‐term follow‐up will be necessary to determine whether the WID‐qEC test appears to reflect biological correlates of lifetime ovulatory cycles and is independently associated with the presence of ovarian cancer. Further research is needed to determine whether this association could have predictive relevance.
AUTHOR CONTRIBUTIONS
Elisa Redl: Investigation; writing – review and editing; formal analysis; methodology; project administration. Chiara Herzog: Investigation; formal analysis; data curation; writing – review and editing. Charlotte Vavourakis: Writing – review and editing; visualization; investigation; data curation; validation. James Barrett: Investigation; supervision; data curation; writing – review and editing. Allison Jones: Writing – review and editing; investigation; data curation; project administration. Iona Evans: Investigation; writing – review and editing; data curation; project administration. Daniel Reisel: Writing – review and editing; data curation. Ranjit Manchanda: Writing – review and editing; investigation; resources. Line Bjørge: Investigation; writing – review and editing; resources. Michal Zikan: Writing – review and editing; investigation; data curation; resources. David Cibula: Resources; data curation; writing – review and editing; investigation. Twana Alkasalias: Writing – review and editing. Angelique Flöter Rådestad: Writing – review and editing; investigation; resources. Kristina Gemzell‐Danielsson: Investigation; writing – review and editing; resources. Louis Dubeau: Writing – review and editing; investigation. Nicola MacDonald: Investigation; writing – review and editing; resources. Davor Jurkovic: Writing – review and editing; investigation; resources. Nora Pashayan: Resources; writing – review and editing; investigation. Martin Widschwendter: Conceptualization; investigation; funding acquisition; writing – original draft; supervision; resources.
FUNDING INFORMATION
This work received funding from the European Union's Horizon 2020 research and innovation program under grant agreement No 634570 (FORECEE) and the European Union's Horizon 2020 European Research Council under grant agreement No 742432 (BRCA‐ERC); The Eve Appeal and the Land Tirol and the Standortagentur Tirol.
CONFLICT OF INTEREST STATEMENT
E.R., C.H., J.B., A.J., I.E., and M.W. are inventors of WID‐qEC‐related patent applications. C.H., J.B., and M.W. are shareholders of Sola Diagnostics GmbH. Sola Diagnostics GmbH holds an exclusive licence to the intellectual property that protects the commercialization of the WID‐qEC test. R.M. has research grant funding for ovarian cancer surveillance/prevention from Barts Charity, Yorkshire Cancer Research, Rosetrees Trust, GSK and North East London Cancer Alliance outside this work and received honoraria for advisory board membership or lectures from Astra Zeneca/MSD/GSK/EGL. All the other authors do not have a conflict of interest.
ETHICS STATEMENT
This study is a sub‐study within the FORECEE program, which received ethical approval from the UK Health Research Authority (REC 14/LO/1633). All participants provided written informed consent.
Supporting information
Table S1. All relevant data supporting this work on cervico‐vaginal samples.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Herzog C , Marin F , Jones A , et al. A simple cervicovaginal epigenetic test for screening and rapid triage of women with suspected endometrial cancer: validation in several cohort and case/control sets. J Clin Oncol. 2022;40:3828‐3838.36001862 10.1200/JCO.22.00266 PMC 9671754 · doi ↗ · pubmed ↗
- 2Schreiberhuber L , Herzog C , Vavourakis CD , et al. The WID‐q EC test: performance in a hospital‐based cohort and feasibility to detect endometrial and cervical cancers. Int J Cancer. 2023;152:1269‐1274.36056582 10.1002/ijc.34275 PMC 10092332 · doi ↗ · pubmed ↗
- 3Evans I , Reisel D , Jones A , et al. Performance of the WID‐q EC test versus sonography to detect uterine cancers in women with abnormal uterine bleeding (EPI‐SURE): a prospective, consecutive observational cohort study in the UK. Lancet Oncol. 2023;24:1375‐1386.37944542 10.1016/S 1470-2045(23)00466-7 · doi ↗ · pubmed ↗
- 4Illah O , Scott M , Redl E , et al. High performance of the DNA methylation‐based WID‐q EC test for detecting uterine cancers independent of sampling modalities. Int J Cancer. 2024;155:800‐806.38739012 10.1002/ijc.35000 · doi ↗ · pubmed ↗
- 5Ken‐Amoah S , Redl E , Domson BKS , et al. Performance of the WID‐q EC test to detect uterine cancers in black women with abnormal uterine bleeding: a prospective observational cohort study in Ghana. Int J Cancer. 2025;156:1055‐1064.39655721 10.1002/ijc.35260 PMC 11701417 · doi ↗ · pubmed ↗
- 6Lurie G , Thompson PJ , Mc Duffie KE , Carney ME , Goodman MT . Prediagnostic symptoms of ovarian carcinoma: a case‐control study. Gynecol Oncol. 2009;114:231‐236.19464044 10.1016/j.ygyno.2009.05.001PMC 2736603 · doi ↗ · pubmed ↗
- 7Bengtsen MB , Veres K , Norgaard M . First‐time postmenopausal bleeding as a clinical marker of long‐term cancer risk: a Danish Nationwide Cohort Study. Br J Cancer. 2020;122:445‐451.31806879 10.1038/s 41416-019-0668-2PMC 7000815 · doi ↗ · pubmed ↗
- 8Widschwendter M , Jones A , Evans I , et al. Epigenome‐based cancer risk prediction: rationale, opportunities and challenges. Nat Rev Clin Oncol. 2018;15:292‐309.29485132 10.1038/nrclinonc.2018.30 · doi ↗ · pubmed ↗